Advancements in computed tomography and MR imaging have greatly improved the detection of ocular abnormalities, necessitating a systematic diagnostic approach. Understanding globe anatomy and recognizing imaging features of both traumatic and non-traumatic conditions are essential for accurate diagnosis and appropriate referral. Awareness of incidental findings, such as degenerative changes or implants, helps avoid unnecessary investigations. This article highlights common pathologic processes affecting the various anatomic layers of the globe, illustrated through case examples, and aims to familiarize readers with the imaging features of frequently encountered ocular diseases.
Key points
-
•
Since the advent of computed and MR imaging, ophthalmic imaging has significantly advanced, allowing for detailed evaluation of the eye globe allowing even detection of subtle globe abnormalities on dedicated and non-dedicated studies.
-
•
This article aims to highlight the relevant anatomy of the globe and illustrate the imaging features of common ocular conditions.
-
•
This article covers commonly encountered clinical conditions; congenital and acquired ocular abnormalities, ocular detachments, inflammatory disorders, trauma, incidental ocular calcifications, and post-surgical changes with illustrative imaging examples.
Abbreviations
| CT | computed tomography |
| MR | magnetic resonance |
| GDD | glaucoma drainage device |
| PFV | persistent fetal vasculature |
| ROP | Retinopathy of prematurity |
| RPE | retinal pigment epithelium |
Introduction
Advances in computed tomography (CT) and MR imaging (MRI) have significantly enhanced the visualization and detection of ocular abnormalities. With improved spatial resolution, assessment of the globes and orbits now requires a more structured and systematic diagnostic approach. In order to interpret the globe abnormality, a proficient understanding of the globe anatomy is essential. Knowledge of the imaging features of both traumatic and non-traumatic globe abnormalities is necessary to ensure accurate diagnosis and appropriate ophthalmology referral. In addition, recognizing incidental findings such as degenerative changes, globe implants, and fillers are important to prevent unnecessary investigations. This article highlights common pathologic processes affecting the various anatomic layers of the globe, illustrated through case examples, and aims to familiarize readers with the imaging features of frequently encountered ocular diseases.
Globe anatomy
The globe occupies about one-third of the bony orbit. Its wall has 3 concentric layers: an outer fibrous coat (sclera and cornea), a vascular uvea (choroid, ciliary body, and iris), and an inner neural retina; the whole globe is invested by Tenon’s fascial capsule. The lens divides the globe into an anterior segment, filled with aqueous humor and accounting for roughly one-sixth of globe volume, and a posterior segment, filled with vitreous humor, which constitutes the remaining five-sixths.
Tenon’s Capsule
The outermost fibrous layer of the eye comprises the sclera and the cornea. The sclera is enveloped in Tenon’s capsule, a thin fascial sheath that separates the globe from orbital fat and creates a socket-like enclosure. Anteriorly the capsule merges with the bulbar conjunctiva, and posteriorly it fuses with the optic nerve sheath. The optic nerve, its sheath, and the ciliary nerves and vessels perforate the capsule posteriorly. , Tendons of all extraocular muscles pass through the capsule to insert on the sclera, and the capsule reflects along each tendon to form a tubular sheath around the muscle. The capsule’s inner surface is smooth and shiny and is separated from the outer sclera by the episcleral or Tenon’s space, a potential interval that can extend between fascia and sclera.
Cornea and Sclera
The cornea and sclera together form the tough, outer fibrous layer of the eye, providing protection and structural support for the intraocular contents. The cornea functions as a transparent window that permits the passage of light, and transitions into the sclera at the limbus. The opaque sclera forms the external coat of the globe, which extends posteriorly from the limbus to the optic nerve sheath. , On MR imaging, the cornea is a low signal intensity structure due to collagen but may be highlighted by an overlying slightly hyperintense tear film on T1-weighted images. The sclera is also composed of collagen, appearing hypointense on MR imaging ( Fig. 1 ).
Normal globe anatomy on MR imaging of the orbits. ( A ) Axial T2-weighted, ( B ) T1-weighted, and ( C ) T1-weighted fat-suppressed contrast-enhanced MR imaging of the orbits. The anterior chamber aqueous humor ( asterisk ) and vitreous humor ( double asterisk ) are diffusely hyperintense on T2-weighted images. The lens ( black arrow ), cornea, and sclera ( white arrow ) appear hypointense on all sequences. The choroid ( white arrowhead ) and ciliary body ( black arrowhead ) show T1-weighted hyperintensity with thin uniform enhancement. ( D ) Simplified annotated illustration of the globe.
Uvea Tract
The uveal tract is the middle vascular layer of the eye and includes the iris, the ciliary body, and the choroid. These 3 parts are continuous, forming an unbroken coat that has an anterior opening, the pupil, and a posterior gap at the optic nerve canal where the choroid is absent.
The iris is a pigmented, circular diaphragm that controls pupil size and the amount of incoming light. It attaches to the ciliary body, a triangular structure with an anterior ridged pars plicata and a posterior pars plana. The aqueous producing pars plicata contains the ciliary processes, which provide attachment for the zonular fibers of the lens. The pars plana extends posteriorly from the ciliary processes to the ora serrata, the anterior boundary of the retina.
The choroid forms the posterior part of the uvea, lying between the sclera and the retina. This highly vascular membrane runs from the optic nerve to the ora serrata and is firmly bound to the sclera near the optic nerve and at the sites where the vortex veins exit the eye, which drain into the ophthalmic veins. On MR imaging the uveal tract appears hyperintense on T1-weighted images and hypointense on T2-weighted images (see Fig. 1 ).
Retina
The retina is the innermost sensory layer of the globe and is composed of 2 layers: the outer retinal pigment epithelium (RPE), which is firmly attached to the underlying choroid, and the inner neurosensory retina responsible for visual perception. The sensory retina extends from the optic nerve head to the ora serrata, where it terminates and forms a crenated wavy ring. At this junction, the RPE becomes continuous with the pigmented and non-pigmented layers of the ciliary body and its processes. The retina is firmly adherent only at the margins of the optic nerve head and at the ora serrata. On MR imaging, the retina is in close apposition to the choroid in normal circumstances and cannot be discerned separately.
Lens
Anterior to the lens lie the iris and the aqueous humor, while posteriorly it is bordered by the vitreous humor. The zonular fibers attach to the outer surface of the equatorial region of the lens capsule and extend outward to the ciliary body, anchoring the lens in place. ,
The space in front of the lens and zonules is divided into 2 chambers by the iris: the larger anterior chamber and the smaller posterior chamber. These chambers are in direct communication through the pupil. On CT, the lens is hyperdense, while on MR imaging it shows hypointensity on both T1-weighted and T2W-weighted images (see Fig. 1 ).
Globe pathology
Disorders in the Size and Shape of the Globe
Anophthalmia and microphthalmia
Anophthalmia and microphthalmia are rare congenital eye abnormalities. There is usually a small eye or a dysplastic remnant and complete anophthalmia is extremely rare ( Fig. 2 ). Microphthalmia is commonly unilateral, but can be bilateral in syndromic cases ( Fig. 3 ).
Axial T2-weighted fat-suppressed sequence demonstrates right anophthalmia with no discernible ocular tissue and a dysplastic optic nerve ( white arrow ).
Unenhanced CT orbits demonstrates small volume globes which appear otherwise normal in configuration, consistent with microphthalmia.
During development, failure in the formation of the optic vesicle or regression of ocular structures already formed may cause microphthalmia or anophthalmia. These may occur in isolation or be associated with ocular disorders including persistent fetal vasculature (PFV), retinopathy of prematurity (ROP), syndromes (eg, fetal alcohol syndrome, and CHARGE syndrome), and congenital infections (e., rubella, toxoplasmosis, varicella, cytomegalovirus). There can also be failure of optic fissure closure, which prevents normal intraocular pressure and produces colobomatous microphthalmia.
Coloboma
Coloboma is a congenital defect that arises when the embryonic optic fissure fails to close, leaving a tissue gap that may involve the iris, lens, retina, choroid, sclera, or optic nerve. Unlike a staphyloma, it reflects tissue loss rather than thinning. The defect usually appears at the fissure site along the inferior globe, and imaging can show a posterior gap with vitreous herniation or a retrobulbar cyst ( Fig. 4 ).
Axial T2-weighted fat-suppressed sequence showing left micropthalmia with a focal defect at the left posterior globe with associated vitreous humor herniation and retrobulbar cyst ( black arrow ).
Staphyloma
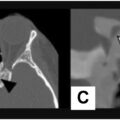
Staphyloma is an outpouching of the wall of the globe, caused by thinning and ectasia of the scleral–uveal coats ( Fig. 5 ). All layers of the globe are present but thinned, distinguishing it from coloboma.
Unenhanced CT orbits in a patient with myopia showing bilateral posterior staphylomas with elongated globes, focal ectatic appearance of the posterior globe with no scleral defect ( black arrows ).
Intraocular potential spaces and ocular detachments
Intraocular Potential Spaces
The eye contains several potential spaces where fluid can accumulate, leading to detachment of ocular layers. Table 1 lists the types of intraocular detachments and potential spaces.
Table 1
Types of intraocular detachments, their corresponding potential spaces and involved ocular layers
| Type of Detachment | Potential Space | Layers Involved |
|---|---|---|
| Posterior hyaloid detachment | Posterior hyaloid space | Fluid between the body of the vitreous and the neurosensory retina |
| Retinal detachment | Subretinal space | Fluid between the sensory retina and the RPE |
| Choroidal detachment | Suprachoroidal space | Fluid between the choroid and the sclera |
Posterior Vitreous Detachment
Posterior vitreous detachment is an age-related process in which the posterior vitreous separates from the retina as the vitreous gel degenerates and liquefies. Weakened adhesions allows liquefied vitreous to dissect between the posterior hyaloid membrane and the retina. When detachment is incomplete, residual focal adhesions, often near the optic disc, can mimic retinal detachment on imaging ( Fig. 6 ). Traction from the partially detached vitreous may produce retinal tears, and vitreous fluid entering a tear can then create retinal detachment.
Unenhanced CT brain with hyperdense fluid along the posterior right globe which crosses the optic disc without attachment, compatible with a posterior hyaloid detachment ( white arrow ).
Retinal Detachment
Retinal detachment is the separation of the sensory retina from the underlying RPE. It is classified as either rhegmatogenous or non-rhegmatogenous. Rhegmatogenous detachment involves a retinal tear that allows fluid to pass into the subretinal space and is most commonly seen in adults, often resulting from vitreous degeneration and traction. Non-rhegmatogenous detachment results from accumulation of fluid beneath the sensory retina without a tear. This implies a breakdown of the blood–retina barrier and may be associated with underlying tumors, infections, inflammatory conditions (eg, posterior scleritis), or vasculopathy. Trauma can lead to retinal detachment with subretinal hemorrhage, which may occur with or without a retinal tear.
On CT and MR imaging, retinal detachment is limited anteriorly by the ora serrata and posteriorly by the margins of the optic disc, resulting in a characteristic V-shaped configuration ( Fig. 7 ).
( A ) Unenhanced CT showing a right retinal detachment and V-shaped hyperdense subretinal fluid ( white arrow ) extending from the ora serrata to optic disc. ( B ) Axial T2-weighted fat-suppressed and ( C ) axial T1-weighted MR sequences in another patient demonstrates a left retinal detachment ( black arrows ) with T2-weighted and T1-weighted hyperintense subretinal fluid.
Choroidal Detachment and Choroidal Effusion
Choroidal detachment is the separation of the choroid from the sclera due to accumulation of fluid or blood in the suprachoroidal space. Serous choroidal detachment is primarily caused by ocular hypotony, which increases choriocapillaris permeability and leads to fluid transudation into the suprachoroidal space. It commonly follows intraocular surgery, penetrating trauma, or inflammatory choroidal conditions. Hemorrhagic choroidal detachment is typically associated with blunt or penetrating ocular injuries or may occur as a complication of intraocular surgery.
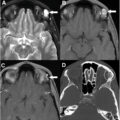
On CT and MR imaging, choroidal detachment is often seen as a lenticular collection that can extend anteriorly to the ciliary body and is not limited by the ora serrata. Posteriorly, the choroidal detachments are limited by the vortex vein insertions leading to a classic biconvex morphology ( Fig. 8 ).
Contrast-enhanced CT orbits ( top ) and axial T2 fluid attenuated inversion recovery (FLAIR) MR sequence ( bottom ) in 2 patients show characteristic biconvex choroidal detachments, bilateral on CT, and in the left globe on MR ( white arrowheads ). The detachments extend to the ciliary body ( white arrows ) beyond the expected location of the ora serrata ( black arrowheads ).
Ocular inflammatory disorders
Scleritis is inflammation of the sclera and the episcleral vascular plexus. It is usually non-infectious and either idiopathic or associated with systemic autoimmune diseases, most commonly rheumatoid arthritis or granulomatosis with polyangiitis. , Infectious scleritis is rare and typically occurs post-surgery or trauma. Anatomically the condition is anterior or posterior according to its relation to the extraocular muscle insertions. Anterior scleritis presents with pain and visible scleral erythema, whereas posterior scleritis causes pain without erythema. Each form may be diffuse, nodular, or necrotizing.
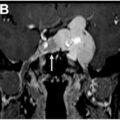
Imaging is seldom required for anterior scleritis, as the diagnosis is clinical. When CT or MR imaging is performed, it can show scleral enhancement, scleral thickening, and focal periscleral cellulitis ( Fig. 9 ). Enhancement may be diffuse, peripheral, or may track along the optic nerve sheath, suggesting optic perineuritis. Nodular scleritis can mimic tumors ( Fig. 10 ).
Axial T2-weighted fat-suppressed ( top ) and fat-suppressed gadolinium-enhanced T1-weighted ( bottom ) MR sequences demonstrate left posterior scleritis with focal scleral enhancing thickening ( white arrow ), episcleral edema and enhancement ( black arrow ). Associated reactive thin subretinal fluid is also seen ( black arrowhead ).
Axial fat-suppressed gadolinium-enhanced T1-weighted MR sequence demonstrating left posterior scleritis ( black arrow ). This is nodular in appearance and can mimic a choroidal tumor ( arrowhead ). Follow-up imaging showed post-treatment resolution.
Uveitis is inflammation of the uveal tract, including the iris, the ciliary body and the choroid. It may be idiopathic or linked to systemic disease, often HLA-B27 seronegative spondyloarthropathies or rheumatoid arthritis ( Fig. 11 ). Diagnosis rests on radiologic findings, laboratory data and evidence of extra-ocular involvement. Imaging can show uveal thickening and enhancement, subretinal effusions ( Fig. 12 ) and abnormal vitreous signal.
Axial fat-suppressed gadolinium-enhanced T1-weighted MR sequences of a 52 year old woman with bilateral panuveitis and a history of Behcet’s disease. There is diffusely thickened uvea with marked enhancement bilaterally ( white arrows ).
Axial T2-weighted ( top ) and gadolinium-enhanced T1-weighted ( bottom ) MR sequences of the orbits demonstrating uveitis with bilateral uveal thickening and enhancement ( black arrows ) and subretinal fluid ( black arrowheads ) in a known case of Vogt-Koyanagi-Harada (VKH) disease.
Leukocoria and intraocular tumors
Leukocoria is loss of the normal red retinal reflex and signals an intraocular process that alters light reflection. It is non-specific and can result from a mass, membrane, retinal detachment or other retinal pathology; frequent causes include retinoblastoma, PFV, Coats’ disease, ROP, among others.
Retinoblastoma
Retinoblastoma is the most common primary intra-ocular tumor of childhood, diagnosed in about 80% of patients by age 3 years, and in 95% by age 5 years. It often arises from mutations in the RB1 tumor-suppressor gene. The hereditary form can affect both eyes and predisposes survivors to later malignancies such as sarcomas, melanomas, and central nervous system tumors. When bilateral ocular tumors are accompanied by a midline intracranial lesion in the suprasellar or pineal region the constellation is termed trilateral retinoblastoma ( Fig. 13 ). Leptomeningeal spread can also occur.
Axial fat-suppressed gadolinium-enhanced T1-weighted MR sequences of the orbit ( A ) and brain ( B ) demonstrating trilateral retinoblastoma: an enhancing left globe tumor ( white arrow ), right enucleation due to retinoblastoma ( black arrow ) and an enhancing pineal mass ( white arrowhead ).
On CT, the presence of a hyperattenuating intraocular mass that demonstrates moderate contrast enhancement is characteristic. The presence of intraocular calcification in a child under the age of 3 years is highly suggestive of retinoblastoma. On MR imaging, the lesion typically appears slightly hyperintense on T1-weighted images and hypointense on T2-weighted images relative to the surrounding vitreous. T2∗-weighted images typically demonstrate low signal voids; linear peripheral areas of low signal may indicate hemorrhage while central nodular low signal suggests calcification ( Fig. 14 ). Following gadolinium administration, the lesion typically demonstrates heterogeneous enhancement.
Related posts:
 Orbital Imaging Modalities and Recent Updates
Orbital Imaging Modalities and Recent Updates
 Imaging of the Cavernous Sinus
Imaging of the Cavernous Sinus
 Multidisciplinary Management of Tumors of the Orbit
Multidisciplinary Management of Tumors of the Orbit
 Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
 Imaging of Central Nervous System Diseases that Affect Vision
Imaging of Central Nervous System Diseases that Affect Vision
 Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


