Orbit is a complex and intricate structure composed of conical bony walls, globe, lacrimal apparatus, soft tissues, optic nerve and cranial nerves III to VI. High-resolution MRI delineates these delicate anatomical structures in orbit, and emerging radiologic techniques including cone beam CT and photon counting CT have shown potentials for added benefit in orbital imaging. Multiple different imaging modalities including US, CT, MRI, and PET play complementary roles; US excels in superficial structures; CT shines in bone assessment; MR offers better tissue characterization; PET can add biochemical metabolic information in addition to other anatomical imaging modalities.
Key points
-
•
Knowledge in complex orbital anatomy is essential in recognizing orbital pathology on imaging.
-
•
Imaging is often necessary to assess retrobulbar pathology as this area cannot be reliably assessed by clinical ophthalmologic examination alone.
-
•
Various imaging modalities including ultrasound (US), computed tomography (CT), MR, PET-CT are available and play complementary role with each other.
-
•
Continued technical evolution contributed to recent updates on each imaging modality, further emphasizing clinical utilities of imaging examinations.
Abbreviations
| 18 F-FDG | 18 Fluoride-fluorodeoxyglucose |
| 18 F-NaF PET | 18 F-sodium fluoride PET |
| 3D | 3-dimensional |
| ASL | arterial spine labeling |
| CT | computed tomography |
| CTV | computed tomography venogram |
| DCE | dynamic contrast enhanced |
| DSA | digital subtraction angiography |
| DWI | diffusion-weighted image |
| MRA | MR angiogram |
| TOF | time of flight |
| US | ultrasound |
Introduction
Orbit is a small space; however, it contains many crucial anatomic structures, not only contributing to vision, the vital function, but also in protecting its own orbital contents to maintain the function.
There is a broad spectrum of pathologies that originate from the orbit proper as well as arising from the adjacent structures affecting the orbit. Some of these pathologies are visible externally and ophthalmologic examination plays a crucial role. On the other hand, some of the pathologies, especially in the retrobulbar location, can be difficult to assess the entire extent by physical examination alone, for which orbital imaging is useful.
Orbital imaging is usually performed with special dedicated protocols including thin slice thickness images with multiplanar reconstruction due to its unique cone-shaped anatomy and small delicate contents. In addition, different imaging modalities play complementary roles in evaluating its substructures. In this article, we will go over each imaging modality used in orbital imaging as well as their recent technological updates.
Discussion
Orbit
The orbit is an interesting anatomic structure which is confined by complex cone-shaped bony walls and nerve foramina ( Fig. 1 ). Multiple different bones form bony orbit, including frontal, ethmoid, zygomatic, maxilla, lacrimal, palatine, and sphenoid bones.
Orbital bony anatomy illustration showing multiple bones comprise bony orbital walls. Bony foramina including optic canal, superior orbital fissure, and inferior orbital fissure are also depicted.
( Image Courtesy Kelly Kage, MFA, CMI.)
Within the orbit, there are multiple extraocular muscles coordinating delicate ocular movement. In terms of its neural contents, optic nerve is coursing in the center of intraconal space, which is an extension of central nervous system not enveloped by Schwann cells. Cranial nerve III, IV, V and VI which are part of peripheral nervous system lined by Schwann cells also course within the orbit.
Orbit contains unique anatomic structures that are not present elsewhere in the rest of the body, such as orbital globe. Thanks to the evolving imaging techniques, some of the globe linings are visible on high resolution orbit MR, with choroid/uveal layer visible on high resolution postcontrast MR as thin enhancing layer, and the outer most sclera layer visible as a hypointense layer on T1-weighted as well as T2-weighted images.
Lacrimal apparatus is another unique structure, secreting, controlling and draining tears to lubricate and protect the orbital structures ( Fig. 2 ). Lacrimal gland is considered an exocrine gland which contains plasma cells and lymphocytes histologically.
Illustration of lacrimal apparatus, a unique structure seen in the orbit. Tears produced in lacrimal gland travels along the ocular surface and drains sequentially via punctum, canaliculi, lacrimal sac, nasolacrimal duct, and eventually into nasal cavity.
( Image Courtesy Kelly Kage, MFA, CMI.)
A detailed review of orbital anatomy will be provided in the subsequent Orbital Anatomy article. As we can infer from above, orbital anatomy is complex. Therefore, appropriate orbital imaging is beneficial in depicting this complex anatomy, mapping important anatomic landmarks especially for preoperative planning, as well as in recognizing pathology especially retrobulbar process which may be difficult to evaluate solely by ophthalmologic examination, while clinical history and ophthalmologic examination remain as essential part of orbital assessment.
Imaging Modalities
Ultrasound
Ultrasound (US) is a useful tool in assessing superficial orbital structures, although it is more commonly used by ophthalmologists than by radiologists. One of the well-known techniques is Ossoinig’s standardized echography suggested by Dr Karl Ossoinig, where the combination of A-scan, B-scan and Doppler US scan, enables reliable assessment of the optic nerve and extraocular muscles and can evaluate the posterior segment pathologies. , US has an advantage of its real-time examination capacity, although it is highly dependent on operator experience, limiting standardization and universal accessibility.
In cases of periorbital/eyelid melanoma or nonmelanomatous skin cancer such as squamous cell carcinoma or sebaceous carcinoma, regional and/or cervical nodal metastases can often occur. For example, the incidence of nodal metastasis is reported in up to 24% of eyelid squamous cell carcinomas. Among the nodal stations, intraparotid and periparotid nodal stations are reported to be most frequently involved, followed by submandibular and jugular chain nodal stations. ,, These suggest intraparotid and periparotid nodal stations may be a gateway for further disease spread below the facial level, necessitating careful evaluation of cervical nodes. Furthermore, the presence of parotid and/or cervical nodal metastasis would alter the management plan including the need for parotidectomy, extent of neck dissection, and need for adjuvant radiation treatment. Luckily, most of these areas are superficially located and can be efficiently assessed by US.
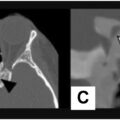
At our institution, a US neck nodal survey examination routinely includes lateral neck compartments from the supraclavicular region up to the superior neck and submandibular regions, the posterior triangle, as well as the central neck compartment. In cases of head and neck cutaneous malignancy including squamous cell carcinoma or melanoma, we also include parotid, periauricular and suboccipital regions in addition to a routine neck survey protocol. In addition, if the patient has a palpable abnormality, US is useful for focused evaluation at the area of interest. Frequently, we perform same-day fine needle aspiration and/or core needle biopsy if a suspicious morphology lymph node or a lesion is detected at the time of diagnostic US. Then, sampled tissues are simultaneously reviewed by a cytologist for adequacy to ascertain a diagnostic quality of sampled tissue, before the patient is released from our institution. This approach has multiple benefits for the patient: increased convenience, decreased scheduling conflicts by reducing the need for a return visit on different date for a repeat procedure, decreased rates of nondiagnostic samples, and expediting clinical management by shortening overall time spent on diagnosis and staging workup ( Fig. 3 ).
Patient with history of lateral canthus melanoma, with new subcutaneous nodule on dermatologic examination. Punch biopsy performed at dermatology clinic was negative for melanoma. ( A ) US image shows 1.1 cm hypoechoic subcutaneous nodule in left temple near surgical scar ( arrow ). ( B ) Simultaneously performed US guided fine needle aspiration of the nodule was positive for melanoma ( arrow ). ( C ) Subsequent 18 F-FDG PET-CT demonstrates FDG avidity at the site of biopsy proven melanoma recurrence in left temple ( arrowhead ).
Plain radiograph and computed tomography
Plain radiograph and conventional computed tomography
Nowadays plain radiograph is often used to screen foreign bodies in orbital regions, especially to rule out metallic foreign bodies before MR when patient has a pertinent history.
Computed tomography (CT) is one of main modalities used not only to assess the presence of orbital pathology, but also to help characterize the process. It is a preferred tool in facial-orbital trauma or other urgent indications, as CT is easily accessible compared to MR, with a quicker acquisition time especially using modern multidetector technology and enabling multiplanar reconstruction in any plane deemed necessary. Additionally, CT is useful in evaluating integrity or lesion involvement of the bony orbital wall. Relatively large amounts of inherent background fat content in orbital space aids in detection of soft tissue mass in orbital space by inherently providing contrast from default background hypodensity.
At our institution, CT of the orbit is obtained from the top of the frontal sinus down to maxilla level. It is usually acquired in bone and soft tissue algorithm with 1.25 mm or 1.5 mm slice thickness and multiplanar reconstruction images are often made in 0.625 mm slice thickness, balancing spatial resolution and signal-to-noise ratio.
Computed tomography angiogram and computed tomography venogram
Oftentimes, orbital–periorbital pathology can be of vascular etiology or closely associated with adjacent vascular structures, necessitating vascular imaging for further investigation. For example, vascular imaging is helpful in detection and characterization of orbital cavernous malformation, hemangiopericytoma, venous varix (with a Valsalva maneuver), arteriovenous fistula/carotid-cavernous fistula, other various types of vascular malformations, and ophthalmic artery aneurysm. In addition, vascular imaging may be useful in assessing tumor vascularity, identifying tumor feeding arteries as well as draining veins, and locating landmark vessels for preoperative vascular mapping when surgical treatment is planned for known orbital tumors.
The gold standard diagnostic tool is digital subtraction angiography (DSA) which can accurately depict vascular anatomy and temporal vascular flow dynamics. It can also provide endovascular treatment as indicated. However, this requires arterial puncture harboring small but nonnegligible risk of bleeding, thrombus, iatrogenic dissection, pseudoaneurysm or arteriovenous fistula formation. In this context, CT based vascular imaging is a good noninvasive alternative option for baseline diagnostic purpose or follow-up of known or treated lesions, unless the patient has a contraindication to iodinated contrast media.
CT arteriography is focused on arterial structure assessment, in which imaging at the peak arterial phase following intravenous contrast administration is essential before venous contamination dominates. To achieve this, most institutions use a bolus tracking technique.
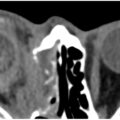
On the other hand, CT venogram (CTV) aims at venous structure assessment by obtaining images in the venous phase. Additional postprocessed images are typically provided with bone subtraction and 3-dimensional (3D) multiplanar reconstruction, which are helpful in conjunction with raw image interpretation. Variation in CTV protocol can be made when orbital venous varix is suspected. In this case, noncontrast orbit CT in resting status can be first obtained, followed by CTV with provocative maneuvers—commonly Valsalva maneuver—that cause elevated venous pressure resulting in characteristic dynamic appearance of venous varix on imaging ( Fig. 4 ).
Patient with history of lymphoma with new orbital mass reported on surveillance neck CT. ( A ) Noncontrast orbit CT in resting status shows minimal soft tissue fullness in right orbit near the orbital apex ( arrow ). ( B ) Postcontrast orbit CT with Valsalva maneuver shows enlarged enhancing mass in right orbit which has similar density as the vessels (dashed circle). This dynamic appearance is most consistent with orbital venous varix and imaging with a provocative maneuver helps clenching the diagnosis.
Cone beam computed tomography
Cone beam CT is a relatively new technique which is being explored for its clinical utilities. Images are generated by cone-shaped radiograph beam detected by 2-dimensional detectors, while conventional CT is acquired by fan shaped radiograph beam detected by 1-dimensional detector. This allows reduction in number of gantry rotations during image acquisition, which in turn saves imaging time. It is also advantageous in that patient radiation dose is lower than that of conventional CT. High spatial resolution and 3D volume rendering capacity are other strengths of cone beam CT.
However, there are drawbacks of cone beam CT mostly derived inherently from the above-mentioned imaging acquisition principle. These include under sampling error, imaging distortion resulted from unequal degree of radiograph attenuation between the center and periphery of the patient, increased scatter radiation with decreased signal to noise ratio and decreased soft tissue contrast resolution, which limits evaluation for soft tissue structures.
Cone beam CT has been clinically applied in dentistry, breast imaging, and imaging guidance for interventional radiology procedures, taking advantage of its accuracy and 3D reconstruction ability in relatively short acquisition time.
In terms of orbital imaging, cone beam CT has also been attempted experimentally, for example, in bony orbital wall integrity assessment in trauma, and relationship of radio-dense graft and bony wall evaluation following orbital reconstruction surgery. Its potential utilities in quantitative measurement of orbital volume and evaluation of bony orbit anatomic landmarks, such as the infraorbital canal have also been reported. In some of these reported cases, cone beam orbit CT produced acceptable quality images for osseous structure evaluation with decreased radiation dose, which has merit over conventional CT, considering the risk of cataract development following repetitive cumulative radiation to the ocular lens. In addition, Raz and colleagues reported that the central retinal artery could be detected on cone beam CT in the orbit region obtained with DSA suggesting its potential role in delicate orbital vessel evaluation, although the study was performed in only small number of patients. However, it needs to be kept in mind that cone beam CT is inferior in the evaluation of soft tissue anatomic structures, characterization of soft tissue mass, and orbital hematoma. Therefore, further validation studies in larger number of cases and careful scrutinization of indication for cone beam CT will be necessary before universal clinical application.
Photon Counting computed tomography
This new emerging CT technique is becoming popular due to its superior spatial and contrast resolution with decreased noise allowing for sharper crisp images optimal to assess minute delicate structures. There are additional benefits of reduced radiation dose and decreased iodine contrast dose needed. These advantages over conventional CT were facilitated by key differences in radiograph detectors. Unlike conventional CT with a scintillator where radiograph beams are converted to light then to electronic signals, photon counting CT uses a semiconductor with voltage across, converting incoming radiograph photons directly to an electronic signal; by skipping the middle light conversion step, septa-related dead space related problems are resolved while achieving smaller pixel size. Another powerful advantage of photon counting CT is multi-energy spectral imaging which has potential applications such as in material composition evaluation or in vascular imaging by reducing calcification related artifacts or with virtual noncalcium mapping. , There is a reported potential utility of photon counting CT in orbital arterial imaging, although there remain technical limitations and data in orbital imaging application in general is sparse, requiring further elucidation.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


