The lacrimal gland produces the aqueous component of the tear film, and its disease can cause dry eye, pain, proptosis, or diplopia. Lacrimal gland lesions are diverse: roughly half inflammatory, a quarter lymphoproliferative, and a quarter epithelial tumor, with substantial overlap in imaging features. Consequently, tissue sampling remains essential for accurate diagnosis and management. Conventional CT and MR imaging aid in diagnosis and define anatomic extent; correlating imaging with clinical history and examination is vital. Advanced MR techniques may offer tissue-specific information. The lacrimal sac and extra-orbital sites should also be considered in formulating differential diagnoses and treatment strategies.
Key points
-
•
The lacrimal gland secretes the aqueous component of the tear film, and its disease can cause dry eye, pain, proptosis, or diplopia.
-
•
Lacrimal gland lesions are roughly 50% inflammatory, 25% lymphoproliferative, and 25% epithelial; significant overlap in imaging features makes tissue sampling essential for accurate diagnosis.
-
•
CT and MR imaging support diagnosis and delineate anatomic extent; clinical history and examination are crucial, and advanced MR techniques can provide tissue-specific insights.
-
•
The lacrimal sac and extra-orbital sites should be considered to refine differential diagnoses and guide management.
Abbreviations
| ACC | adenoid cystic carcinoma |
| ADC | apparent diffusion coefficient |
| AJCC | American Joint Commission on Cancer |
| ASL | arterial spin labeling |
| CT | computed tomography |
| DWI | diffusion weighted imaging |
| IgG4-RD | IgG4-related disease |
| IOI | idiopathic orbital inflammation |
| MALT | mucosa-associated lymphoid tissue |
| NLDA | nasolacrimal drainage apparatus |
| PA | pleomorphic adenoma |
| PSMA | Prostate Specific Membrane Antigen |
| SS | Sjogren syndrome |
| TED | thyroid eye disease |
Introduction
The lacrimal gland, located in the superolateral orbit, secretes the aqueous component of the tear film, essential for maintaining eye surface health and lubrication. Pathology of the lacrimal gland can lead to dry eye, pain, proptosis, and/or diplopia. Roughly 50% of lacrimal gland lesions are inflammatory, 25% are lymphoproliferative, and 25% are tumors of epithelial origin analogous to salivary gland tumors. In conjunction with clinical history and physical examination, computed tomography (CT) and magnetic resonance (MR) imaging can help support or narrow a differential diagnosis. Given the considerable overlap between imaging features of inflammatory and lymphoproliferative processes, as well as benign and malignant neoplasms, tissue sampling plays a key role in the diagnosis and management of lacrimal gland disorders.
The lacrimal gland is part of the lacrimal system ( Fig. 1 ), a network of structures that produces, distributes, and drains tears from the eyes. Though the lacrimal glands are the focus of this review, we will also briefly discuss the anatomy and pathology of the lacrimal sac. The lacrimal sac, located in the inferomedial orbit, serves as a dynamic reservoir for tears and actively facilitates their movement into the nasolacrimal duct. Like the lacrimal gland, it may be affected by epithelial tumors, inflammatory disease, or lymphoproliferative processes. ,
Lacrimal system. The lacrimal gland is located in the superolateral orbit and secretes the aqueous component of tear film. Tears are then distributed across the ocular surface and evaporate or drain into the lacrimal sac and nasolacrimal duct apparatus. [ Permission will be assessed by editorial team after submission .]
Normal anatomy
Lacrimal Gland
The exocrine lacrimal gland sits in the lacrimal fossa, a depression in the superolateral bony orbit formed by the frontal bone. Its vascular supply comes from the lacrimal artery, a branch of the ophthalmic artery. The gland is comprised of 2 lobes, the palpebral lobe and the orbital lobe, separated by the lateral horn of the aponeurosis of the levator palpebrae superioris muscle. The smaller palpebral lobe is located anteriorly and inferiorly and extends into the eyelid, while the larger orbital lobe is located posteriorly and superiorly. Inflammatory and lymphoproliferative processes tend to involve the lacrimal gland diffusely and may be unilateral or bilateral, whereas tumors of epithelial origin more commonly arise from the orbital lobe and are characteristically unilateral. The lacrimal glands are typically relatively symmetric, and the presence of asymmetry in conjunction with ipsilateral signs and symptoms suggests a pathologic process.
Lacrimal Apparatus
The upper and lower eyelids spread tears across the ocular surface and toward the lacrimal lake near the medial canthus. Tears then either evaporate from the ocular surface or are drawn into the nasolacrimal duct system. During blinking, the contraction of orbicularis oculi muscle attachments creates a “tear pump,” drawing tear film into the superior, inferior, and common lacrimal canaliculi and then into the lacrimal sac. The lacrimal sac is lined with epithelium and sits in a second lacrimal fossa formed by the anterior lacrimal crest of the frontal process of the maxilla and the posterior lacrimal crest of the lacrimal bone. Tears drain from the lacrimal sac into the nasolacrimal duct and then through the valve of Hasner (plica lacrimalis) into the inferior meatus of the nasal cavity.
Imaging technique
The lacrimal glands are well assessed on cross-sectional imaging. CT with intravenous contrast is often the first line imaging modality ( Fig. 2 ), particularly when patients present acutely with pain and/or signs of infection/inflammation. Lacrimal gland enlargement can be detected on CT, as can surrounding soft tissue changes and the presence of calcifications or foreign bodies. Osseous remodeling or more aggressive bone erosion is well assessed on CT and can help characterize a lacrimal lesion.
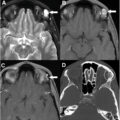
CT appearance of normal lacrimal glands. ( A ) Axial and ( B ) coronal contrast-enhanced CT scans demonstrate the normal and symmetric appearance of the lacrimal glands ( solid arrows ). The glands are located in the superolateral orbits and demonstrate mild homogeneous enhancement.
Because of its superior soft tissue resolution, MR imaging with intravenous contrast helps identify and characterize lacrimal gland pathology ( Fig. 3 ). While the orbits are typically included within the field of view on MR imaging of the brain, dedicated MR imaging of the orbits performed before and after the administration of intravenous contrast is recommended for evaluation of lacrimal gland lesions. An optimal MR orbits protocol , should include small field-of-view non-contrast axial and coronal T1-weighted imaging (T1WI) and T2-weighted imaging. Posteriorly, it is helpful to extend the field of view past the chiasm to capture sellar and cavernous sinus pathologies contributing to visual field defects. Non-contrast T1-weighted imaging should be performed without fat suppression in order to exploit inherent T1 hyperintense fat signal to delineate anatomic structures. Post-contrast imaging, commonly but not universally performed with fat suppression, is also recommended to characterize intraorbital lesions and assess the presence or absence of enhancement.
MR appearance of normal lacrimal glands ( solid arrows in all figure parts). ( A ) Axial non-contrast T1WI demonstrates symmetric lacrimal glands, which are intermediate in signal. ( B ) Coronal T2 with fat suppression (FS) shows T2 intermediate signal in both lacrimal glands. ( C ) Coronal post-contrast T1FS shows mild homogenous enhancement of both lacrimal glands. In this patient, on ( D ) DWI, the glands show symmetric mild diffusion restriction, and on ( E ) ASL, the glands show symmetric mildly elevated perfusion. The glands are normally difficult to perceive on DWI and ASL, as normal glands do not demonstrate significant diffusion restriction or hyperperfusion. In some cases, normal lacrimal glands may show mild symmetric diffusion restriction or hyperperfusion on studies ordered for non-lacrimal-related indications, and this is considered to be within the spectrum of normal. ASL, arterial spin labeling; DWI, diffusion weighted imaging; MR, magnetic resonance.
In addition to conventional anatomic sequences, advanced imaging sequences are increasingly utilized to further characterize pathology of the lacrimal glands. The presence of restricted diffusion on diffusion weighted imaging (DWI) can suggest the presence of hypercellular tumor, and apparent diffusion coefficient (ADC) values can help distinguish lymphoma from inflammatory pathologies. Perfusion imaging, including arterial spin labeling (ASL) and bolus perfusion techniques, may also be helpful in differentiating lacrimal gland pathologies.
Ultrasound is a cost-effective and widely accessible imaging tool commonly used by ophthalmologists and in the emergency setting to evaluate retinal and ocular pathologies. While ultrasound can be used to detect anterior orbital lesions, CT and MR imaging are more commonly employed to evaluate lesions arising from the lacrimal glands.
The lacrimal glands can be assessed on PET, usually in the context of 18F-fluorodeoxyglucose (FDG) imaging for lymphoproliferative disorders and systemic staging of malignancy. Radiotracer-avid lacrimal lesions may also be detected incidentally when PET is performed for another indication. For most lacrimal gland pathologies, however, CT and MR imaging are the primary imaging modalities for lesion evaluation and characterization.
Pathologies involving the nasolacrimal drainage apparatus (NLDA) can be assessed with CT and MR imaging. Conventional dacryocystography has also been employed to investigate intrinsic functional abnormalities of the NLDA but offers limited soft tissue resolution.
Pathology of the lacrimal glands
Inflammatory, infectious, and neoplastic pathologies affecting the lacrimal glands can result in overlapping imaging features that lead to diagnostic uncertainty. Adopting a systematic approach considering laterality, morphology, and the presence or absence of aggressive features can help create or refine a list of differential diagnoses ( Fig. 4 ).
A systematic approach to the more commonly seen lacrimal gland lesions.
Inflammation
Inflammatory or autoimmune conditions comprise half of all lacrimal gland pathologies. These can be isolated to the glands themselves or accompanied by other orbital or systemic manifestations. Inflammatory pathologies are commonly bilateral, which can be helpful when creating a differential diagnosis. Huang and colleagues found that inflammatory conditions account for 60% of bilateral lacrimal gland pathologies, with idiopathic orbital inflammation and IgG4-related disease (IgG4-RD) being the most common. Lymphoproliferative processes are more commonly unilateral, though 13% to 25% of all cases can be bilateral. , In contrast, epithelial tumors are usually unilateral.
Idiopathic orbital inflammation (IOI) is a non-granulomatous inflammatory process also known as orbital pseudotumor, inflammatory dacryoadenitis, or non-specific orbital inflammation. A variety of orbital manifestations may accompany lacrimal gland involvement, including optic perineuritis, scleritis, myositis involving the extraocular muscles, and infiltration of orbital fat, often in a mass-like fashion. Patients with IOI involving a lacrimal gland or glands typically present with pain, diplopia, proptosis, and edema, which may improve rapidly with corticosteroids, a helpful diagnostic feature of this entity. Tissue sampling may be necessary for definitive diagnosis if the patient’s clinical picture is atypical, for example, non-steroid responsive or relapsing/remitting.
CT and MR imaging will both demonstrate diffuse enlargement of the affected gland(s) in IOI, typically involving both the orbital and palpebral lobes. The affected glands are usually relatively isointense or hypointense compared with extraocular muscles on T2-weighted MR imaging, though they can be mildly hyperintense, and they usually enhance avidly on post-contrast imaging ( Fig. 5 ). There is no associated bone erosion. CT and MR imaging may also demonstrate associated extra-lacrimal inflammation as noted above.
IOI: A 50 year old female patient presents with acute right periorbital swelling and pain with extraocular movements. ( A ) Coronal T2FS demonstrates a heterogeneous T2 intermediate to slightly hyperintense mass in the right superolateral orbit involving the lacrimal gland and superior rectus muscle with ill-defined margins ( solid arrow ). T2 hyperintense edema is present in adjacent pre-septal soft tissues ( asterisk ). ( B ) Non-contrast axial T1WI shows pre-septal T1 isointense soft tissue stranding within the subcutaneous fat ( asterisk ). ( C ) Axial post-contrast T1FS demonstrates avid enhancement of the mass in the right superolateral orbit ( solid arrow ) and adjacent ill-defined enhancement in the pre-septal soft tissues ( asterisk ). Enhancement and thickening of the right sclera are also present ( dashed arrow ). On ( D ) DWI and ( E ) ADC, the mass exhibits mildly reduced diffusivity with a mean ADC of 1.377 × 10 −3 mm 2/s. On ( F ) ASL perfusion, there is markedly elevated perfusion associated with the mass ( solid arrow ) and along the right sclera ( dashed arrow ). ADC, apparent diffusion coefficient; ASL, arterial spin labeling; DWI, diffusion weighted imaging; IOI, idiopathic orbital inflammation.
IOI has historically been considered a diagnosis of exclusion since its conventional imaging features overlap with other inflammatory and lymphoproliferative processes. Both IOI and lymphoma can cause unilateral or bilateral lacrimal gland enlargement that molds to the contour of the globe and shows avid enhancement and reduced diffusivity. Lymphoma typically demonstrates lower ADC values than inflammation due to its high cellularity , however, with studies demonstrating ADC values of less than 0.70 × 10 −3 mm 2/s for lymphoma and greater than 1.0 × 10 −3 mm 2/s for orbital inflammation. ,,
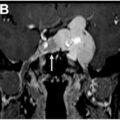
IgG4-RD ( Fig. 6 ), a multisystem inflammatory process characterized by lymphoplasmacytic infiltration and IgG4 deposition in involved organs, is a distinct clinicopathological entity that overlaps with IOI in its clinical and imaging features. Certain imaging characteristics are more specific to IgG4-RD, however, and can support the diagnosis. Lacrimal gland involvement in IgG4-RD is more commonly bilateral compared with IOI. IgG4-RD also more frequently involves the paranasal sinuses and salivary glands. Observing T2 intermediate mucosal thickening rather than the typical T2 hyperintense signal seen in acute rhinosinusitis may point toward IgG4-RD. Thickening of the infraorbital nerve(s) is also more specific to IgG4-RD. IgG4-RD can also involve almost every organ, with well-known systemic manifestations including autoimmune pancreatitis, retroperitoneal fibrosis, hypophysitis, and hypertrophic pachymeningitis. , Clinically, IgG4-RD usually presents less acutely and with a more indolent course than IOI syndrome.
IgG4-RD: A 60 year old female patient presents subacutely with diplopia, swelling, and proptosis of the left eye. ( A ) Coronal T2FS shows asymmetric enlargement of the left lacrimal gland with intermediate signal ( solid arrows ). Mild ill-defined inflammatory stranding is present in the adjacent intraconal fat ( asterisk ). T2 intermediate mucosal thickening is present within the paranasal sinuses ( dashed white arrow ), compatible with IgG4-related inflammation. ( B ) Axial and ( C ) coronal post-contrast T1FS images demonstrate avid enhancement of the enlarged left lacrimal gland ( solid arrow ). Mild ill-defined enhancement is present within the adjacent intraconal fat ( asterisk ). ( D ) ASL demonstrates elevated perfusion signal within the enlarged gland ( solid arrow ). ( E ) DWI and ( F ) ADC demonstrate low diffusivity ( solid arrow ), with a mean ADC of 0.789 × 10 −3 mm 2/s, a value that is low for IgG4-RD and demonstrates the non-specificity of this parameter. ADC, apparent diffusion coefficient; ASL, arterial spin labeling; DWI, diffusion weighted imaging; IgG4-RD, IgG4-related disease.
Diagnosing IgG4-RD can be challenging due to its variable manifestations and its tendency to mimic both infection and malignancy. Furthermore, serum IgG4 concentrations can be normal in greater than 30% of patients with IgG4-RD. The American College of Rheumatology and the European League Against Rheumatism have proposed a classification system to determine the likelihood of IgG4-RD, integrating histopathologic, serologic, and imaging features. Markedly elevated serum IgG4 concentrations, characteristic histologic features such as dense lymphocytic infiltrate, and the presence of one or more commonly involved organ systems make the diagnosis of IgG4-RD more likely.
Chronic inflammation of the lacrimal glands is also a common orbital manifestation of sarcoidosis , a multisystem inflammatory process characterized by granulomatous inflammation. CT and MR imaging both demonstrate diffuse enlargement of one or both lacrimal glands ( Fig. 7 ), with avid enhancement on post-contrast imaging. The diagnosis can be supported by thoracic imaging demonstrating mediastinal and hilar lymphadenopathy. Intracranial manifestations of sarcoidosis such as dural/leptomeningeal enhancement, cranial nerve enhancement, and thickening of the pituitary stalk may also be visible on orbital CT/MR imaging studies, but these findings also overlap with IgG4-RD.
Sarcoidosis with bilateral but asymmetric involvement of the lacrimal glands: A 65 year old female patient presents with progressive right eye swelling over 2 months with increasing pain. ( A ) Coronal T2FS demonstrates diffuse marked enlargement of the right lacrimal gland and mild enlargement of the left lacrimal gland with T2 intermediate signal ( solid arrow ). Mild T2 hyperintense inflammatory stranding is noted in the right preseptal soft tissues ( asterisk ). ( B ) Axial post-contrast T1FS shows avid enhancement in both glands ( solid arrows ). ( C ) On ASL perfusion, there is corresponding hyperperfusion in both glands ( solid arrows ). ( D ) DWI and ( E ) ADC demonstrate moderately reduced diffusivity (with a mean ADC value of 1.014 × 10 −3 mm 2/s; solid arrows ). ( F ) Coronal contrast-enhanced CT chest demonstrates mediastinal and right hilar lymphadenopathy ( dashed arrows ). ADC, apparent diffusion coefficient; DWI, diffusion weighted imaging.
Sjogren syndrome (SS) is an immune-mediated process affecting the salivary and lacrimal glands, causing dry mouth and dry eye. It can be primary or secondary, the latter occurring in conjunction with other autoimmune diseases like rheumatoid arthritis. In addition to the symptoms listed above, serology positive for anti-Sjogren syndrome antibodies (anti-SSA and anti-SSB) or minor salivary gland biopsy in those with negative serology can confirm the diagnosis. In the acute phase, patients may present with bilateral and symmetric lacrimal gland enlargement ( Fig. 8 ). In long-standing SS, the salivary and lacrimal glands may appear more heterogeneous, with fatty infiltration and atrophy. On CT, such glands may demonstrate heterogeneously hypodense fat density interspersed with gland parenchyma. On non-contrast T1WI, the lacrimal glands may appear small with areas of heterogeneous intrinsic T1 hyperintensity compatible with fat deposition. Given the increased risk of developing lymphoma in the setting of SS, new or progressive enlargement of previously atrophic salivary or lacrimal glands should warrant further investigation and consideration of tissue sampling.
SS in 2 different patients, one with acute disease and one chronic. ( A ) Coronal T2FS of the orbits in a patient with an acute presentation of SS demonstrates enlargement and T2 intermediate signal of both lacrimal glands ( solid white arrows ). ( B ) Coronal T2FS of the upper neck demonstrates enlargement and T2 intermediate signal of both parotid glands ( asterisk ). ( C ) Coronal non-contrast T1 of the orbits in a patient with longstanding SS demonstrates profound fatty atrophy/infiltration of the lacrimal glands ( dashed arrows ). ( D ) Axial non-contrast T1 of the neck demonstrates diffuse fatty infiltration of the parotid glands ( solid black arrows ). SS, Sjogren syndrome.
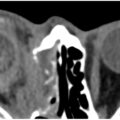
Orbital amyloidosis , characterized by extracellular deposition of misfolded sheets of amyloid protein in involved organs, can be localized or a manifestation of systemic amyloidosis. While orbital amyloidosis most commonly involves the eyelids, it can also involve the lacrimal glands and lacrimal sac unilaterally (most common) or bilaterally, as well as the extraocular muscles. CT scans demonstrate variable enlargement of one or both lacrimal glands, often with areas of coarse calcification ( Fig. 9 ), while MR imaging typically shows marked T2 hypointensity of the involved gland(s).