Orbital tumors are diverse and relatively rare. Imaging studies such as MR imaging, computed tomography (CT), PET/CT, and ultrasound are essential for narrowing the differential diagnosis before surgery. The specific surgical approach for orbital tumors depends on location of the mass, size, and proximity to important orbital structures. The authors advocate close collaboration between the neuroradiologist and the orbital surgical team through weekly or monthly teaching and planning conferences and collaborative investigations that can ultimately lead to new discoveries and more reliable diagnoses and outcomes for patients with newly diagnosed orbital malignancy.
Key points
-
•
Orbital tumors are varied, and radiologic assessment is critical to arriving at a short, relevant list of differential diagnoses prior to surgery.
-
•
Close collaborations between the neuroradiologist and the orbital surgical team can lead to a unique collective expertise in recognizing radiologic patterns of various orbital lesions, defining the extent of tumor involvement, and ultimately to better patient outcomes.
Abbreviations
| CT | computed tomography |
| RMS | rhabdomyosarcoma |
| US | ultrasound |
Introduction
Throughout this issue of Radiology Clinics , we are reminded of the importance of multidisciplinary expertise for the optimal management of orbital tumors, particularly the need for close collaboration between the neuroradiologist and the orbital surgeon. Familiarity with the wide spectrum of orbital tumors is key to forming a comprehensive differential diagnosis at the time of initial presentation of a patient with an orbital mass. The combined experience of the neuroradiologist and the orbital surgeon can help recognize radiologic patterns of presentation for various orbital lesions and arrive at the correct diagnosis.
Surgery is often necessary to confirm the diagnosis and may also be the definitive treatment for most orbital tumors. However, the exact surgical approach often depends on the presumptive diagnosis of the orbital tumor, the location of the mass, its size, and the extent of involvement of the various critical orbital structures.
For example, in the case of a newly diagnosed lacrimal gland mass, surgical management may differ significantly depending on whether the lesion is suspected to be lymphoid, in which case an incisional biopsy may be appropriate. , In contrast, for a suspected pleomorphic adenoma of the lacrimal gland, an incisional biopsy can lead to problematic multifocal recurrences and even the possibility of malignant transformation. , Recognizing the radiologic features typical of each of these entities greatly helps in planning the surgical management of lacrimal gland tumors. In the preoperative radiology report, the surgeon looks to the neuroradiologist to help distinguish among lacrimal gland lymphoma, pleomorphic adenoma, and lacrimal gland carcinoma, and ideally the differential diagnosis should be narrowed to the likely entity to aid surgical planning. ,,,,
We have found that regular monthly or weekly conferences with active participation by the neuroradiologist and the orbital surgical team are very helpful in building collective expertise in recognizing radiologic and clinical patterns of presentation of various orbital tumors, with the overall goal of arriving at the most likely preoperative diagnosis and planning the best surgical plan.
Indications for operative management
Indications for orbital surgery are varied. For some lesions, an incisional biopsy is appropriate to confirm the diagnosis. For example, in orbital lymphoid tumors, the goal of surgery is to confirm the histologic diagnosis and guide subsequent management. , In contrast, for many benign or malignant orbital tumors, complete surgical resection is desirable. ,,, Examples include cavernous venous malformations that may be causing proptosis or visual field defects and should be completely removed, and pleomorphic adenomas of the lacrimal gland, for which an incisional biopsy is contraindicated and complete surgical excision with the pseudocapsule intact is essential to avoid future multifocal recurrences or even malignant transformation. ,, For an in-depth discussion of this topic, refer to the Bradley A. Thuro and Bita Esmaeli’s article, “ Multi-disciplinary Management of Tumors of the Orbit ,” in this issue of Clinics of Radiology .
History and clinical examination
The oculoplastic surgeon begins by taking a detailed history, including eye-related issues, previous treatments and surgeries, and systemic health issues. This includes the patient’s symptoms, such as onset, pain, lesion growth, vision changes, eyelid malposition, tearing, and cosmetic concerns. Common findings associated with an orbital tumor may be new onset of proptosis, globe displacement, eyelid malposition, periorbital swelling, corneal exposure symptoms, and diplopia.
Ocular/periocular examination
The surgeon will perform a thorough examination of the patient’s eyes, eyelids, and periorbital soft tissues. The patient’s vision, eyelid position (including ptosis or retraction), extraocular muscle function, abnormal tear drainage, and any other abnormalities or asymmetry will be documented. The patient’s visual fields will be assessed for blind spots or loss of vision. The location, size, fixation, and any relationship to vital structures of a tumor will be documented. For potential lesions of the globe, a slit-lamp examination can provide information about the anterior chamber and ocular surface, and fundoscopy can be used to examine the retina and the optic nerve. Cranial nerve function should be evaluated particularly CN II through VII. Hertel exophthalmometry may help in measuring the amount of proptosis. Extraocular motility examination needs to be documented as well as the pupil size and function.
Choosing the appropriate imaging study
Preoperative Radiologic Evaluation
Upon referral, if preoperative imaging is available, the orbital surgeon and neuroradiologist should first determine whether repeat or additional imaging is needed. This determination may depend on the quality of the study, the location and extent of the lesion, including possible bone involvement, and the preliminary differential diagnosis.
Radiologic Studies
Direct involvement of a neuroradiologist may be needed to determine which imaging studies are most appropriate for diagnosing a particular orbital lesion. In general, MR imaging is the study of choice for evaluating a suspected orbital mass. MR imaging can assess soft tissue tumors, including signal characteristics, extent, and perineural tumor spread. , At our institution, the orbital MR imaging protocol includes axial T1 pre-contrast without fat saturation, axial and coronal T2 with fat saturation, and orthogonal T1 post-contrast with fat saturation. Images are acquired with a 3 mm thickness and a 3.3 mm spacing. An axial diffusion-weighted series is acquired with a 5 mm thickness and 5 mm spacing. Additional imaging may include a thick-section T2 series of the neck with fat saturation to assess the salivary gland and neck for adenopathy, at 4 mm thickness and 5 mm spacing. If there is concern for intracranial metastases, orthogonal T1 post-contrast and FLAIR sequences of the brain can be added. For lesions of the optic nerve, a T2 sequence with fat saturation obtained perpendicular to the nerve may be acquired.
Computed tomography (CT) may be needed instead of or in addition to MR imaging in some cases where the bony component of an orbital mass requires better evaluation. CT also aids in the evaluation of fractures and dislocations, intact but remodeled, eroded, or destroyed (more aggressive possibilities), or hyperostotic lesions, for example, adjacent to a meningioma. ,, In addition, CT provides a means for evaluating tumors of the dermal surface, including the eyelids, assessing for calcifications in retinoblastoma, and helping to avoid potential pitfalls such as physiologic calcifications, and for evaluating the orbit when there is susceptibility artifact on MR imaging related to metallic orbital devices. ,, At our institution, we acquire thin-section CT in the axial plane after the administration of intravenous contrast and reconstruct it in the sagittal and coronal planes. Imaging can be extended beyond the orbit to include the neck and brain to determine the full extent of the lesion, assess for parotid and neck adenopathy, and evaluate for bony and intracranial metastasis.
Preoperative CT angiography and CT venography can be used to assess the location of tumors adjacent to arteries and veins and to plan intra-arterial chemotherapy administration. Preoperative CT and MR imaging surgical navigation studies can also be used to create 3D models, which are loaded into a system that enables real-time instrument tracking during surgery by registering them to the patient’s anatomy, ensuring accuracy for delicate procedures.
For lesions suspected to have systemic metastases or when the growth rate of an orbital mass is of interest, a total-body PET/CT scan may be appropriate in addition to standard dedicated orbital imaging. The PET/CT provides information on tumor metabolic activity, local and distant metastases, staging, site selection for biopsy based on metabolic activity, and evaluation of treatment response.
Ultrasound (US) complements CT and MR imaging in evaluating the cervical chain, the posterior neck, the suboccipital and postauricular regions, and the salivary glands. Immediate US-guided fine needle aspiration biopsy is performed to confirm metastasis in lymph node basins and the salivary glands.
Specific features to include in a radiology report
From the orbital surgeon’s perspective, specific details that would be important to include in a neuroradiology report and that would help guide the choice of surgical approach may include the following:
General
-
•
The size of the orbital mass should be reported. This is important for surgical planning and for AJCC classification for lacrimal gland carcinomas and orbital sarcomas.
-
•
Whether the mass involves the intraconal space, extraconal space, or both ( Figs. 1 and 2 ). This is important in determining the resectability of the lesion and for surgical planning.
Fig. 1 Venous malformation: ( A ) Axial T2 MR image shows a well-circumscribed, homogeneously hyperintense intraconal mass ( arrow ). ( B , C ) Axial and sagittal T1 post-contrast MR images show heterogeneous enhancement of the mass after contrast administration in B , which demonstrates filling in of contrast in C , the later acquired sagittal sequence, in keeping with a low-flow vascular lesion ( arrows ).
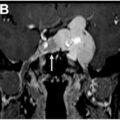
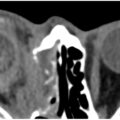
Fig. 2 Lacrimal gland adenoid cystic carcinoma. ( A ) Axial T1 post-contrast MR imaging shows a large, infiltrative, intraconal, and extraconal right lacrimal mass with extension through the lateral orbital wall into the suprazygomatic masticator space ( arrow ) and posteriorly into the sphenoid bone ( black arrow ). ( B ) Coronal T1 post-contrast MR imaging shows involvement of all 4 quadrants of the orbit with abutment of a medially displaced optic nerve ( black arrow ) and destruction of the orbital floor with extension into the maxillary sinus ( white arrow ).
Which quadrants of the orbit are involved? Inferior, superior, nasal, temporal quadrants, or a combination of all the above (see Fig. 2 ). This is important in planning the skin incisions and entry point into the orbit as described in Bradley A. Thuro and Bita Esmaeli’s article, “ Multi-disciplinary Management of Tumors of the Orbit ,” in this issue.
-
•
Are the extraocular muscles involved? Which ones are involved? Is there abutment, displacement, or invasion of the nerve ( Fig. 3 )?
Fig. 3 Idiopathic orbital inflammation. ( A ) Axial T1 MR imaging without contrast shows multifocal infiltrative disease in the premaxillary soft tissues ( large white arrows ) with involvement of the infraorbital nerves ( small white arrows ), and the retromaxillary soft tissues and pterygopalatine fossae ( black arrows ). ( B ) Axial T1 post-contrast shows disease involving the infraorbital nerves ( small white arrows ), bilateral inferior rectus muscles ( large white arrows ), and the left superior orbit and left levator palpebrae muscle, and lacrimal glands ( black arrow ).
-
•
Is the lesion multifocal or bilateral in nature (see Fig. 3 ; Fig. 4 )?
Fig. 4 Metastatic breast carcinoma and leptomeningeal disease. ( A ) Axial T1 post-contrast MR imaging shows metastatic disease in the left orbit involving the intra-and extraconal spaces and medial canthus and medial rectus muscle ( white arrows ). An intraconal metastasis is present in the right orbit ( black arrow ) and there is posterior fossa leptomeningeal disease ( white circle ). ( B ) Sagittal T1 post-contrast MR imaging shows an intracranial metastasis ( arrow ).
-
•
Does the orbital mass have a well-circumscribed or irregular contour (see Fig. 1 ; Figs. 5 and 6 )?
Fig. 5 Lacrimal gland pleomorphic adenoma. ( A , B ) Axial and coronal T1 post-contrast MR images show a well-circumscribed, homogenously enhancing left lacrimal gland mass ( arrows ).
Fig. 6 Lacrimal gland adenoid cystic carcinoma. ( A , B ) Axial and coronal T1 post-contrast MR images show an infiltrating left lacrimal gland mass with intraconal extension that encases the left optic nerve ( black arrows ), involves extraocular muscles, the left orbital roof ( large white arrow ), and extends posteriorly through the left superior orbital fissure ( small white arrow ).
-
•
Is it infiltrative and molds to surrounding structures (see Fig. 6 ; Figs. 7 and 8 )?
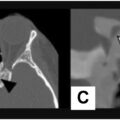
Fig. 7 Marginal zone lymphoma. ( A , B ) Axial and coronal T1 post-contrast MR images show an infiltrative mass in the superior right orbit ( large white arrow ) that extends into the intraconal space and encases the optic nerve ( small white arrow ). ( C ) Apparent diffusion coefficient map shows signal hypointensity (restricted diffusion) in the mass ( arrow ). ( D ) Axial PET/CT shows FDG-avidity of the mass ( arrow ).
Fig. 8 Follicular lymphoma (grade 1). ( A , B ) Axial and coronal T1 post-contrast MR image shows a homogeneously enhancing left lacrimal gland mass that molds to the superotemporal orbital wall ( arrows ) with inferonasal displacement of the globe.
-
•
Is the orbital mass homogeneous or heterogeneous in appearance (see Figs. 5 and 8 ; Fig. 9 )? Is it fluid-filled ( Fig. 10 )?
Fig. 9 Recurrent anaplastic solitary fibrous tumor (WHO grade III). ( A , B ) Axial T1 post-contrast and axial T2 MR images show a heterogeneously enhancing right orbital mass with significant proptosis. Note the flow voids within the mass ( arrows ).