Pathology of the cavernous sinus encompasses a broad and heterogeneous group of conditions that reflect the complex anatomy and critical neurovascular contents of this region. Accurate diagnosis relies on careful integration of clinical presentation with high-resolution imaging that delineates lesion location, extent, and behavior relative to the cavernous sinus walls, cranial nerves, and internal carotid artery. While many disease entities share overlapping imaging and clinical features, recognition of key distinguishing characteristics allows meaningful narrowing of the differential diagnosis and guides appropriate management strategies.
Key points
-
•
Overlapping clinical and imaging manifestations of cavernous sinus (CS) pathologies require careful differential diagnosis.
-
•
Identification of CS invasion by pituitary adenoma is critical to guiding treatment and heavily relies on high resolution MR imaging.
-
•
Meningiomas and schwannomas of the CS can often be differentiated based on their high-resolution MR imaging features.
-
•
Toloso-Hunt syndrome is a diagnosis of exclusion.
-
•
Acute septic thrombosis of the CS is a rare life-threatening condition that radiologists should remember to include in their workup.
Abbreviations
| AIFS | acute invasive fungal sinusitis |
| CCF | carotid-cavernous fistulas |
| CICA | cavernous internal carotid artery |
| CIFS | chronic invasive fungal sinusitis |
| CS | cavernous sinuses |
| FS | fungal sinusitis |
| ICA | internal carotid artery |
| IgG4-RD | immunoglobulin G4-related disease |
| ILT | inferolateral trunk |
| MHT | meningohypophyseal trunk |
| NHL | Non-Hodgkins lymphoma |
| PA | pituitary adenomas |
| THS | Tolosa-Hunt syndrome |
| VMs | venous malformations |
Introduction
The cavernous sinuses are complex anatomic crossroads where critical neurovascular structures traverse a confined dural space, making them uniquely vulnerable to a wide spectrum of pathologic processes. Lesions involving the cavernous sinuses often present significant diagnostic and therapeutic challenges because diverse etiologies, including neoplastic, inflammatory, infectious, and vascular disorders—can produce overlapping clinical manifestations and imaging appearances. A thorough understanding of cavernous sinus anatomy, patterns of cranial nerve involvement, venous drainage, and arterial relationships is therefore essential for accurate localization, differential diagnosis, and treatment planning. This article reviews the detailed anatomy of the cavernous sinus, correlates clinical presentations with underlying pathophysiology, and systematically discusses the imaging features of common and uncommon cavernous sinus pathologies, with an emphasis on practical distinctions that guide clinical management.
Anatomy
The cavernous sinuses (CS) are paired venous spaces enclosed within dural layers on either side of the sella turcica. Bony borders of the CS include the tuberculum sella and the anterior clinoid process anteriorly, the posterior clinoid process posteromedially, the petroclival fissure posteroinferiorly. The CS is laterally confined by the double layered dura of the middle cranial fossa. The superficial (meningeal, outer or lateral) layer covers the temporal lobe. The deep (inner or medial) layer envelops the oculomotor (CNIII), trochlear (CNIV), ophthalmic (CNVi), and maxillary (CNVii) nerves. The roof of the CS is made by a horizontal projection of the middle cranial fossa dura named as the transverse plate. The transverse plate attaches to the anterior and posterior clinoid processes and medially continues as the diaphragma sella. The medial wall of the cavernous sinus is made by a single layer of dura. The floor of the CS is formed by the dura lining the greater wing of the sphenoid bone.
The contents of the CS include endothelium lined fibrous septa that separate venous caverns, ligaments, the abducens (CNVI) nerve, the internal carotid artery (ICA), sympathetic ganglia and fat. CNs III, IV, Vi and Vii are embedded withing the lateral wall of the CS ( Fig.1 ). The intracavernous ligaments anchor the medial wall to the other walls and the ICA and are important structures in the context of transcavernous surgery but will not be further described here.
Coronal contrast-enhanced CISS image through the CS. The CNVI ( short white arrow ) is surrounded by enhancing venous space. The CNIII ( black arrow ), ophthalmic (Vi) and maxillary (Vii) nerves are embedded within the lateral wall of the cavernous sinus. Cc, Cavernous ICA; Cs, Supraclinoid ICA; P, pituitary gland; Viii, Mandibular nerve.
Along the posterior wall of the CS is a triangular area called the basin, which is bordered superiorly by the transverse plate, laterally by the petroclinoid folds (extensions of tentorium) and inferiorly by Meckel’s cave. The CNIII and CNIV enter the CS through the basin. The CNIII carries a 6 to 8 mm long pocket of arachnoid around it which is readily visible on MR imaging along the superior lateral margin of the CS. The CNVi and CNVii leave the Meckel’s cave to enter the CS along its posterolateral margin. The CNVI exits the prepontine cistern by piercing the dural layers and travels through venous spaces (the basilar plexus and the inferior petrosal sinus) before entering the cavernous sinus, usually below the ligament extending from the petrous apex to the dorsum sellae. The CNVI carries dura, arachnoid and fibrous bands around it as it travels through the CS. All other cranial nerves travel anteriorly enclosed within the lateral wall of the CS and exit the CS through the superior orbital fissure.
The CS receives venous blood from the superior and inferior ophthalmic veins, sphenoparietal sinus, superficial middle cerebral vein and the pterygoid plexus of the masticator space and drains into the superior and inferior petrosal sinuses. The anterior and posterior intercavernous sinuses connect the right and left CS.
The branches of the cavernous ICA can be variable and most consistently include the meningohypophyseal trunk (MHT) and the inferolateral trunk (ILT). The MHT is located along the medial surface of the posterior genu and gives off branches to supply the posterior pituitary, clivus, cranial nerves, and the tentorium. The ILT arises as a single trunk or multiple vessels from the lateral surface of the cavernous ICA and supplies the adjacent dura and cranial nerves. Both ILT and MHT have extensive collaterals with each other and external carotid artery branches.
The persistent trigeminal artery, present in 0.2 %-0.4% of the population, serves as a conduit between the cavernous ICA (cICA) and the basilar artery. It travels in the CS within a course parallel to CN VI and leaves the CS through the dorsum sellae near Meckel’s cave.
Symptoms
Most patients with CS pathologies are symptomatic and most frequently present with progressive cranial neuropathy of the CNs II-IV. Visual impairment due to CNII compression and/or ischemia is common at presentation. A thorough neuro-ophthalmologic assessment is essential and should include evaluation of the visual acuity, ocular mobility, facial and corneal sensation. Exophthalmos and chemosis may result from mass effect and compression of veins. While routine endocrinologic assessment is not indicated hormonal disturbance may be present in tumors of the CS and most frequently include hyperprolactinemia due to disturbance of the pituitary infundibulum.
Cranial neuropathies can be isolated or multiple and include sympathetic and parasympathetic dysfunction. A specific combination of symptoms and examination findings may help pinpoint the exact anatomic location of the pathology as in orbital apex syndrome (ophthalmoplegia + vision loss + sensory loss in CNVi distribution), superior orbital fissure syndrome (ophthalmoplegia + sensory loss in CNVi distribution) and cavernous sinus syndrome (ophthalmoplegia + sensory loss in CNVi and CNVii distributions + Horner’s syndrome). However, it’s difficult to ascertain etiology as many different pathologies give rise to similar symptoms and findings.
Cavernous sinus pathologies
Neoplasms
Pituitary adenoma
In surgical series, up to 10% of pituitary adenomas (PA) are found to be invading the CS typically by violating the medial wall of the CS which is made of only a single layer of dura ( Fig.2 ). PAs invading the CS are the most common tumors of the CS. CS invasion by PA is a major predictor of incomplete surgical resection, failure to achieve remission in endocrinologically active PAs and recurrence thus presurgical recognition of CS invasion is important. Cottier and colleagues tested the hypothesis proposed by Knosp and colleagues by assessing PA relationship with the cICA on the coronal MR images as a predictor of CS invasion. , In their series CS invasion was found to be highly probable if (1) PA extended lateral to the lateral intercarotid line (tangent connecting the lateral edges of the cICA and supraclinoid ICA), or (2) PA encased greater than 67% of the cICA circumference or (3) PA effaced the carotid sulcus venous compartment (the venous space inferior to the cavernous cICA). There was no CS invasion if (1) PA did not extend lateral to the medial intercarotid line (tangent connecting the medial edges of the cICA and supraclinoid ICA) or (2) PA encased less than 25% of the cICA circumference.
Coronal contrast-enhanced T1W image through the sella shows a large PA infiltrating the right CS. The right cICA is completely encased but not narrowed ( arrowhead ). A small normal appearing pituitary gland is noted on the left ( long arrow ). The medial venous space in the left CS is maintained indicating no CS invasion ( short arrow ).
Micko and colleagues further refined the Knosp classification and established a 6-tier probabilistic scheme for PA invasion of CS. In this work, the medial, middle and lateral intercarotid lines differentiated 4 tiers with 2 additional tiers identified based on PA invasion inferior to the cICA and complete circumferential encasement of cICA ( Fig. 3 ). Only 25% of the patients were assigned either the lowest (0) or the highest grade (4) which predicted 0% and 100% probability of CS invasion, respectively. The intermediate grades predicted an increasing likelihood of PA invasion with increasing grade, underscoring the difficulty of providing a definitive evaluation on preoperative MR imaging. One of the observations common in multiple surgical series is that even small microadenomas may invade the CS while the likelihood of CS invasion increases with increasing tumor size.
Medial intercarotid (MICL), intercarotid (ICL) and lateral intercarotid (LICL) lines and Knosp’s grades are superimposed on coronal CISS image. Grade 4 occurs when PA completely encircles the cICA as seen in Fig. 2 .
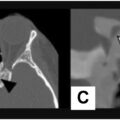
To improve surgical outcomes new techniques such as endoscopic transcavernous approach and medial wall resection have been developed. Intraoperative and histologic examination of the medial wall allowed identification of 3 distinct patterns of CS involvement: (1) Focal invasion, (2) Wall thickening, and (3) Wall destruction. High resolution MR imaging of the pituitary has shown some success in identifying subtle forms of CS invasion preoperatively ( Figs. 4 and 5 ).
Contrast-enhanced coronal T1W image ( A ) shows a small adenoma in the left lateral aspect of the pituitary with extension to the intercarotid line ( arrow ). Contrast-enhanced coronal CISS image ( B ) shows the lesion abutting the anterior clinoid process ( arrow ) implying grade 3a disease.
Contrast-enhanced coronal T1W image ( A ) shows a small adenoma ( arrow ) in the left lateral aspect of the pituitary with the medial venous compartment of the CS being uneffaced, suggesting no CS invasion. Contrast enhanced coronal ( B ) and axial ( C ) CISS images reveal a tiny nubbin of tissue ( arrow ) protruding into the cavernous sinus. A small dural defect and CS invasion was found in surgery.
Meningioma
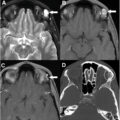
Meningiomas are the most common primary tumors of the CS and make up to 40% of all CS tumors. They can arise from within the CS proper, CS walls or adjacent dura. When the CS proper is involved by meningioma, either primarily or by secondary invasion, curative surgery becomes unfeasible due to high rate of neurovascular complications ( Fig.6 ). , Surgical resection of the extracavernous portion of meningioma followed by stereotactic radiotherapy targeting the residual CS component is a common treatment strategy in today’s practice. , Imaging plays a critical role in surgical planning and differential diagnosis. Encasement of the ICA and CNs is readily visualized on high resolution images. Meningiomas arising from the lateral wall and growing toward the middle cranial fossa are good surgical candidates ( Fig. 7 ). A homogenously enhancing tumor infiltrating the CS and encasing the CNs is almost invariably a meningioma as other tumors tend to displace or replace the CNs ( Fig. 8 ). Narrowing of the ICA by a CS tumor implies meningioma; although this finding is not always present in meningiomas it is rarely seen with other tumors. Hyperostosis in the adjacent bones and dural tail sign are other helpful imaging findings that point to meningioma although their absence would not necessarily exclude meningioma.
Coronal ( A ) and axial ( B ) contrast-enhanced T1W images show a typical CS meningioma completely filling the CS and extending to the middle and posterior cranial fossa along dural reflections. Notice dural tails ( arrows ) and narrowing of the cICA.
Axial ( A ) and coronal ( B ) contrast-enhanced CISS images show a meningioma arising from the lateral wall of the left cavernous sinus which doesn’t involve the CS proper ( arrow in a). The CNIII ( black arrow ), CNVi ( white arrow ) and CNVii ( arrowhead ) are visible separate from the mass on image b. Surgical resection is feasible.
Related posts:
 Orbital Imaging Modalities and Recent Updates
Orbital Imaging Modalities and Recent Updates
 Imaging of the Globe
Imaging of the Globe
 Multidisciplinary Management of Tumors of the Orbit
Multidisciplinary Management of Tumors of the Orbit
 Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
 Imaging of Central Nervous System Diseases that Affect Vision
Imaging of Central Nervous System Diseases that Affect Vision
 Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


