This article provides a comprehensive imaging-based description of central nervous system diseases that impair vision, spanning infectious, inflammatory, neoplastic, vascular, metabolic, neurodegenerative, congenital, traumatic, and idiopathic etiologies. It integrates visual pathway anatomy with characteristic clinical and imaging findings, emphasizing lesion localization from the retina to the occipital cortex. Advanced neuroimaging techniques, particularly MRI and CT, are highlighted as essential tools for diagnosis, prognostication, and management. By correlating areas of structural pathology with visual field deficits and pupillary abnormalities, this study underscores the critical role of imaging in preserving visual function and guiding clinical care.
Key points
-
•
Visual dysfunction in central nervous system disease reflects lesions anywhere along the visual pathway, from the retina and optical nerve to the occipital cortex.
-
•
Lesion localization along the visual pathway strongly predicts the pattern of visual field deficits and pupillary abnormalities.
-
•
A wide spectrum of vascular, inflammatory, infectious, neoplastic, metabolic, and neurodegenerative disorders can involve the visual pathways.
-
•
Advanced imaging techniques, including diffusion and tractography, enhance assessment of optical radiations and occipital lobe involvement.
Abbreviations
| CMV | Cytomegalovirus |
| CNS | central nervous system |
| CT | Computed tomography |
| CZS | Congenital Zika syndrome |
| DWI | diffusion-weighted imaging |
| EW | Edinger-Westphal |
| HSV | Herpes Simplex Virus |
| ICP | intracranial pressure |
| IIH | idiopathic intracranial hypertension |
| LGN | lateral geniculate nucleus |
| MCA | middle cerebral artery |
| MLF | medial longitudinal fasciculus |
| MS | multiple sclerosis |
| NMOSD | neuromyelitis optica spectrum disorder |
| PCA | posterior cerebral artery |
| RGC | retinal ganglion cell |
| SC | superior colliculus |
| TBI | traumatic brain injury |
| TORCH | Toxoplasmosis, CMV, Rubella, Syphilis, HSV |
Introduction
Central nervous system (CNS) diseases encompass a wide spectrum of pathologies capable of impairing vision and significantly reducing quality of life. Visual dysfunction in these diseases may arise from direct involvement of the optical nerve, optical chiasm, optical tract, lateral geniculate nucleus (LGN), optical radiations, or visual cortex, as well as from secondary processes such as increased intracranial pressure (ICP) or vascular compromise. CNS pathologies that affect vision can be broadly classified into infectious, inflammatory, neoplastic, vascular, metabolic, neurodegenerative, congenital, traumatic, and idiopathic categories, with each class affecting distinct components of the visual pathway and manifesting with characteristic clinical and imaging findings ( Table 1 ).
Table 1
CNS diseases affecting vision: classification, anatomic location, imaging findings, and clinical features
| Disease Category | Example Disorders | Anatomical Location | Key Imaging Findings | Clinical Features |
|---|---|---|---|---|
| Infectious | Tuberculosis, CMV retinitis, Herpes retinitis, TORCH, Congenital Zika Syndrome (CZS) | Optical nerve, chiasm, occipital lobe, retina | MR imaging: T2/FLAIR hyperintensity, contrast enhancement of optical nerve/chiasm; CT: cortical calcifications (in CZS) | Vision loss, visual field defects, cortical visual impairment, retinal necrosis |
| Inflammatory | Multiple sclerosis, NMOSD, neurosarcoidosis | Optical nerve, optical tract, brain parenchyma, meninges | MR imaging: T2 hyperintense demyelinating lesions, optical nerve enhancement, granulomas (sarcoidosis) | Optical neuritis, monocular or bilateral visual loss, visual field deficits |
| Neoplastic | Optical nerve glioma, pituitary adenoma, craniopharyngioma, meningioma, lymphoma, brain metastases | Optical nerve, chiasm, occipital lobe | MR imaging: Mass lesion, contrast enhancement, edema, possible optical nerve compression; CT: mass effect, calcifications | Visual field defects (bitemporal hemianopia, homonymous hemianopia), progressive vision loss, papilledema |
| Vascular | Retinal artery/vein occlusion, ischemic optical neuropathy, PCA infarct, temporal arteritis | Retina, optical nerve, visual cortex | MR imaging: Diffusion restriction (stroke), T2/FLAIR hyperintensity; CT angiography: vessel occlusion | Hemianopia, quadrantanopia, cortical blindness, visual hallucinations, visual agnosia, prosopagnosia |
| Metabolic | Adrenoleukodystrophy, MELAS, Leigh syndrome, thiamine deficiency, Batten disease, small vessel disease | Optical nerve, optical radiations, visual cortex | MR imaging: White matter abnormalities, cortical atrophy, basal ganglia lesions; MR spectroscopy: lactate peaks | Visual loss, optical neuropathy, cortical visual impairment, diplopia |
| Neurodegenerative | Alzheimer’s disease, Parkinson’s disease, Lewy body dementia, posterior cortical atrophy, Creutzfeldt–Jakob disease | Visual cortex, parietal/occipital association areas, retina | MR imaging: Cortical and subcortical atrophy, occipital/parietal cortical thinning; FDG-PET: hypometabolism | Visual hallucinations, visuospatial deficits, cortical visual syndrome, rapid cortical blindness, impaired eye movement control |
| Congenital | Holoprosencephaly, septo-optical dysplasia, periventricular leukomalacia, congenital hydrocephalus, perinatal stroke | Optical nerve, optical radiations, visual cortex, white matter | MR imaging: Malformations (absent septum pellucidum, polymicrogyria, agenesis of corpus callosum), white matter injury, cortical thinning | Congenital visual impairment, cortical visual deficits, visual field abnormalities |
| Traumatic | TBI, shearing injury, posterior circulation stroke post-trauma | Optical nerve, chiasm, optical tract, visual cortex | MR imaging: Susceptibility-weighted imaging for microhemorrhages, DTI for axonal injury, CT for acute hemorrhage | Cortical blindness, hemianopia, visual neglect, motion perception loss, visual attention deficits |
| Idiopathic | Idiopathic intracranial hypertension, functional/psychogenic visual loss, idiopathic occipital atrophy | Optical nerve, visual cortex | MR imaging: Normal or subtle cortical atrophy, empty sella (IIH) | Visual field loss, papilledema (IIH), inconsistent exam (functional), progressive cortical visual loss (idiopathic occipital atrophy) |
Abbreviations : CMV, cytomegalovirus; CT, computed tomography; CZS, Congenital Zika syndrome; DTI, diffusion tensor imaging; FDG- PET, fluorodeoxyglucose positron emission tomography; FLAIR, fluid-attenuated inversion recovery; IIH, idiopathic intracranial hypertension; MELAS, mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes; MR, magnetic resonance; MR imaging, magnetic resonance imaging; NMOSD, neuromyelitis optica spectrum disorder; PCA, posterior cerebral artery; T2, T2-weighted imaging; TORCH, toxoplasmosis, other infections [including syphilis], rubella, cytomegalovirus, and Herpes Simplex Virus.
Infectious Diseases
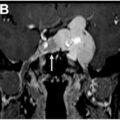
Infectious CNS diseases can involve the visual pathway at multiple levels, leading to optical neuritis, uveitis, retinitis, or encephalitis. Bacterial infections, such as tuberculosis, may directly affect the optical nerve, optical chiasm, or occipital lobe. Cat scratch disease caused by Bartonella henselae can result in optical neuropathy and neuroretinitis. Viral infections also pose significant risk; cytomegalovirus (CMV) can cause retinitis, particularly in immunocompromised patients such as those with HIV/AIDS, transplant recipients, or chemotherapy patients, at times leading to blindness. Herpes viruses, including Herpes Simplex Virus (HSV) ( Fig. 1 ) and varicella-zoster virus, can cause acute retinal necrosis and/or cerebritis. Congenital infections, as part of the TORCH complex (Toxoplasmosis, CMV, Rubella, Syphilis, HSV), can produce visual impairment by damaging the developing brain and visual cortex, as well as the retina and choroid. Congenital Zika syndrome (CZS) is associated with microcephaly, cortical malformations, and profound visual deficits. Computed tomography (CT) and MR imaging studies have demonstrated occipital cortical volume loss in 95% of affected infants, even in cases where the ocular examination is normal, highlighting the importance of neuroimaging in identifying cortical visual impairment.
Sequela of HSV encephalitis involving the optical radiations within the right temporal lobe. Axial T2-weighted ( A ), axial FLAIR ( B ), axial postcontrast T1 ( C – D ), and coronal postcontrast T1 showing encephalomalacia ( white arrows ) involving the right temporal lobe, including portions of the optical radiations (Meyer’s Loop) in a patient with sequela of HSV encephalitis. HSV, Herpes Simplex Virus.
Inflammatory Diseases
Inflammatory disorders frequently target the optical nerve and optical pathway. Multiple sclerosis (MS) ( Fig. 2 ) and neuromyelitis optica spectrum disorder (NMOSD) are prototypical demyelinating diseases that produce optical nerve inflammation and white matter lesions. Myelin oligodendrocyte glycoprotein antibody-associated disease frequently affects vision through acute optical neuritis with prominent inflammatory signs. Visual recovery after high-dose corticosteroids is often favorable, however, relapses are common and can lead to cumulative optical nerve damage and permanent visual impairment. Neurosarcoidosis is characterized by granulomatous lesions that may affect the optical nerves, meninges, or brain parenchyma, at times leading to irreversible visual impairment. Imaging modalities, including contrast-enhanced MR imaging and PET-CT, are critical for detecting inflammatory lesions and monitoring response to therapy.
Multiple sclerosis lesions involving the optical radiations. Axial FLAIR imaging in a patient with long-standing history of multiple sclerosis, including old demyelination lesions involving the optical radiations, with an example on the right noted by a white arrow.
Neoplastic Diseases
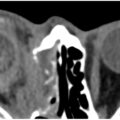
Neoplasms affecting the visual pathway can be primary or secondary and involve structures from the optical nerve to the occipital cortex. Optical nerve gliomas, commonly associated with neurofibromatosis type 1, are slowly growing tumors that can compromise visual function. Pituitary macroadenomas ( Fig. 3 ) and craniopharyngiomas frequently exert mass effect on the optical chiasm, producing bitemporal hemianopia. Meningiomas arising from the dura mater near the optical nerve or chiasm may similarly cause progressive visual loss. Occipital lobe tumors interfere with visual processing and may result in homonymous visual field defects. Lymphomas and brain metastases may infiltrate visual pathway structures, depending on their location, resulting in variable visual symptoms. Additionally, tumors can increase ICP, leading to papilledema and secondary optical nerve damage. Early recognition using MR imaging and CT is vital, as timely intervention may preserve visual function.
Pituitary macroadenoma extending into the suprasellar cistern and exerting mass effect on the inferior aspect of the optical chiasm. Coronal ( A ) and sagittal ( B ) post-contrast T1-weighted imaging showing a heterogeneously enhancing mass lesion contacting and elevating the left aspect of the optical chiasm ( white arrow ).
Vascular Diseases
Vascular disorders are a major cause of vision loss, affecting both the eye and the brain. Local vascular compromise in the retina can result in retinal artery or vein occlusion, ischemic optical neuropathy, or retinopathy secondary to systemic diseases such as diabetes or hypertension. Large vessel occlusions involving the posterior cerebral artery (PCA), which supplies the occipital lobe and visual cortex, can cause homonymous hemianopia or quadrantanopia. The clinical spectrum of vascular injury extends beyond field defects to include visual hallucinations, visual agnosia, neglect, prosopagnosia, and cortical blindness. ,, Imaging modalities such as diffusion-weighted MR imaging and CT angiography are crucial for identifying ischemic injury and guiding intervention.
Metabolic Diseases
Metabolic disorders can disrupt vision through direct effects on the optical nerve, retina, or visual cortex. X-linked adrenoleukodystrophy causes demyelination, predominantly involving the parietal and occipital white matter that frequently compromises visual pathways ( Fig. 4 ). Mitochondrial disorders, such as MELAS and Leigh syndrome, impair energy metabolism, leading to optical neuropathy and cortical visual impairment. Thiamine deficiency, hepatic encephalopathy, and storage diseases, such as Batten disease, may similarly produce vision loss by damaging neuronal tissue, particularly through involvement of the retina, optical nerve, optical radiations, and visual cortex. Systemic metabolic diseases, including diabetes and hypertension, can compromise the vasa nervorum of cranial nerves, resulting in diplopia or other ocular motor deficits. , Neuroimaging, including MR spectroscopy, may help identify metabolic abnormalities affecting visual pathways.
Adrenoleukodystrophy involving the optical radiations. Axial ( A ), sagittal ( B ), and coronal ( C ) FLAIR imaging in a case of adrenoleukodystrophy showing extensive involvement of the white matter tracts of the optical radiations.
Neurodegenerative Diseases
Neurodegenerative disorders can affect vision through ocular involvement or cortical degeneration. Disorders such as age-related macular degeneration, glaucoma, and retinitis pigmentosa primarily involve the retina or optical nerve, while diseases like Alzheimer’s and Parkinson’s disease affect visual perception and processing through cortical and subcortical degeneration. Posterior cortical atrophy, a variant of Alzheimer’s disease, presents with cortical visual syndrome, including visuospatial and perceptual deficits. The Heidenhain variant of Creutzfeldt–Jakob disease produces rapid cortical blindness. Lewy body dementia is characterized by visual hallucinations and perceptual errors, while Parkinsonian syndromes may cause subtle visuospatial and ocular motor deficits. Neuroimaging, particularly volumetric MR imaging and functional imaging, aids in assessing structural and functional changes underlying visual dysfunction.
Congenital Disorders
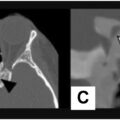
Congenital cerebral visual impairment arises from maldevelopment or early damage to visual pathways. Structural brain malformations, such as holoprosencephaly, septo-optical dysplasia ( Fig. 5 ), lissencephaly, pachygyria, polymicrogyria, schizencephaly, and corpus callosum agenesis, can all affect optical nerves, optical radiations, or the visual cortex. Posterior fossa malformations, including Chiari and Dandy–Walker malformations, may distort visual pathways. White matter abnormalities (such as periventricular leukomalacia), congenital hydrocephalus, or arachnoid cysts, can compromise the optical radiations. Perinatal hypoxic-ischemic injury is the most common cause of congenital visual impairment worldwide, while congenital stroke or intracranial hemorrhage affecting visual structures further contributes to early-life vision loss. Genetic, metabolic, infectious, and inflammatory disorders may also manifest as congenital visual pathway deficits, highlighting the importance of neuroimaging for early detection and intervention, particularly when reversible causes can be identified.
Septo-optical dysplasia. ( A ) Coronal STIR showing diminutive bilateral optical nerves ( white arrows ). ( B ) Small optical canal bilaterally with diminutive canalicular segment of the bilateral optical nerves. ( C ) Axial T2 weighted imaging showing the lateral ventricles with an absent septum pellucidum.
Traumatic Disorders
Traumatic brain injury (TBI), brainstem injury, or cranial nerve trauma can disrupt vision. Focal cortical injury may cause immediate cortical blindness or hemianopia, while diffuse axonal injury can produce delayed visual field deficits and impaired visual attention. Traumatic ischemia involving the PCA territory may result in occipital lobe stroke with homonymous hemianopia. Injury to the optical chiasm or optical tracts may produce specific visual field defects, and higher-order cortical injury may result in visual neglect, agnosia, or impaired motion perception. MR imaging, particularly with susceptibility-weighted imaging and diffusion tensor imaging, plays a central role in assessing post-traumatic visual pathway injury.
Idiopathic Disorders
Idiopathic visual loss encompasses conditions in which no structural, infectious, inflammatory, traumatic, or metabolic cause can be identified. Idiopathic intracranial hypertension (IIH) is characterized by elevated ICP of unknown etiology, producing papilledema and visual field loss. Functional or psychogenic visual disorders may present with apparent blindness in the setting of normal imaging and inconsistent examination findings. Idiopathic occipital atrophy is a rare condition associated with slowly progressive cortical visual loss. Neuroimaging may reveal subtle cortical atrophy or be entirely normal, necessitating careful correlation with clinical findings.
In summary, CNS diseases affecting vision encompass a broad range of etiologies, each with unique mechanisms of injury, clinical manifestations, and imaging characteristics. Infectious, inflammatory, neoplastic, vascular, metabolic, neurodegenerative, congenital, traumatic, and idiopathic disorders may impact any level of the visual pathway, from the retina to the occipital cortex. Advanced imaging modalities, particularly MR imaging and CT, are critical in identifying the location, extent, and nature of these lesions. Clinicians must integrate clinical examination, neuroimaging, and functional assessments to accurately localize pathology, guide treatment, and predict visual outcomes. Understanding the diverse causes of CNS-related visual impairment is essential for timely diagnosis, intervention, and preservation of visual function.
Visual pathway anatomy overview
The visual system is a highly specialized and complex neural network responsible for the reception, transmission, and processing of visual information. The pathway begins in the retina, where light stimuli are converted into electrical signals through a process called phototransduction. Photoreceptors—comprising rods and cones—are specialized neurons that detect light and color. Rods are highly sensitive to dim light and facilitate scotopic vision, whereas cones are responsible for color perception and high-acuity photopic vision. Upon stimulation, photoreceptors release neurotransmitters that activate bipolar cells, which, in turn, transmit signals to retinal ganglion cells (RGCs).
The axons of RGCs converge in the retinal nerve fiber layer to form the optical nerve head. The optical nerve is a collection of over one million axons that exit the globe via the lamina cribrosa and extend posteriorly toward the brain ( Fig. 6 ). At the optical chiasm, fibers from the nasal half of each retina cross to the contralateral optical tract, while temporal fibers remain ipsilateral. This partial decussation enables the visual cortex to integrate binocular visual input, providing depth perception and a cohesive visual field.
Retinal neural elements and optical nerve formation. The retinal photoreceptors, cones and rods, receive light information and pass an electrical signal to the bipolar cells, which synapse with ganglion cells and transmit the information. The ganglion cells have long axons that extend to form the optical nerve at the optical papilla (optical nerve head), subsequently continuing toward the brain.
After the chiasm, the fibers continue as the optical tracts, which terminate primarily in the LGN of the thalamus. The LGN acts as a relay and processing hub, where information is organized and sent via the optical radiations to the primary visual cortex (V1) in the occipital lobe. The optical radiations follow a precise trajectory: fibers representing the superior visual field pass through the parietal lobe, whereas fibers representing the inferior visual field travel via Meyer’s loop in the temporal lobe. This organization is clinically significant, as lesions along specific portions of the pathway result in predictable visual field deficits, such as homonymous hemianopia, quadrantanopia, or scotomas.
The visual cortex receives its blood supply predominantly from the posterior cerebral arteries and their branches, including the calcarine, posterior temporal, and parieto-occipital arteries. Notably, the occipital pole, which mediates central vision, may receive dual blood supply from anastomoses between PCA branches and the superior temporo-occipital branch of the middle cerebral artery. This dual vascularization is clinically relevant because ischemic or hemorrhagic events affecting one arterial territory may produce selective visual field deficits while sparing central vision.
Visual field defects correlate with the anatomic location of lesions along the pathway. For instance, retinal or optical nerve injuries typically produce monocular visual loss, whereas chiasmal lesions—such as pituitary adenomas—classically result in bitemporal hemianopia. Lesions of the optical tract, LGN, or optical radiations often cause homonymous hemianopia, with the location of quadrantic or hemianopic defects determined by the portion of the visual field represented by the affected fibers. Lesions affecting the occipital cortex may produce cortical blindness or scotomas, which are often congruous between both eyes due to the precise retinotopic organization of the primary visual cortex (V1) ( Fig. 7 ).