Orbital trauma is a common consequence of craniofacial injury with potential for permanent vision loss. Rapid, accurate imaging interpretation is essential for triage and surgical planning. Multidetector computed tomography is the primary modality, enabling detection of fracture patterns, globe injury, extraocular muscle entrapment, and vascular complications. This article offers a systematic approach to orbital trauma evaluation, emphasizing findings that require urgent intervention, such as globe rupture, retrobulbar hematoma, muscle entrapment with ischemia, and orbital apex involvement. Diagnostic pitfalls and indications for surgical consultation are also discussed.
Key points
-
•
Most orbital fractures do not require emergent intervention. Urgent management is reserved for those with globe rupture, muscle entrapment causing ischemia, or associated retrobulbar hematoma.
-
•
Intraocular air and anterior chamber depth asymmetry are specific signs of globe rupture on computed tomography (CT), even when other signs are absent.
-
•
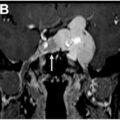
A dilated superior ophthalmic vein on CT suggests vascular injury, including carotid-cavernous fistula.
-
•
Muscle entrapment may be suggested by subtle rounding or deviation, even without obvious displacement.
-
•
Detection of an intraocular foreign body escalates management urgency, as these require removal within 24 hours to prevent infection and vision loss.
Abbreviations
| ACD | anterior chamber depth |
| CSF | cerebrospinal fluid |
| CT | computed tomography |
| DWI | diffusion-weighted imaging |
| ENT | ear, nose, and throat |
| IOFB | intraocular foreign body |
| MCT | medial canthal tendon |
| MIP | maximum intensity projection |
| NOE | naso-orbito-ethmoid |
| SOV | superior ophthalmic vein |
| STIR | short tau inversion recovery |
| ZMC | zygomaticomaxillary complex |
Introduction
Orbital trauma is a common and clinically important subset of craniofacial injury that carries a substantial risk of vision loss. Imaging plays a central role in the acute setting, where radiologic findings directly inform triage and surgical planning. In the United States, eye injuries account for nearly 3% of all emergency department visits, with an estimated 2.5 million incidents annually and a lifetime risk approaching 1 in 70.
Orbital fractures represent a major component of ocular trauma. Between 2006 and 2017, more than 350,000 orbital fractures were treated in US emergency departments, corresponding to an age-adjusted incidence of 10.9 per 100,000 population. Incidence is nearly twice as high in men and boys and demonstrates a bimodal distribution, with peaks in adults aged 21 to 30 and again in those older than 70. Assault is the leading cause among younger adults, whereas falls predominate in the elderly.
This article provides radiologists with a systematic approach to evaluating orbital trauma in the emergency setting. It outlines mechanisms of injury and their imaging correlates, with attention to fractures, globe injury, extraocular muscle entrapment, optic nerve injury, and vascular complications. Imaging modalities are reviewed with emphasis on computed tomography (CT) as the first-line tool, supported by MR imaging and ultrasound in selected cases. The article highlights imaging findings that require urgent intervention and reviews indications for surgical referral. Common diagnostic pitfalls are also discussed.
Orbital anatomy and mechanisms of injury
The orbit is a pyramidal bony cavity formed by 7 craniofacial bones: the frontal, sphenoid, zygomatic, maxillary, ethmoid, lacrimal, and palatine bones, which together define the 4 orbital walls (roof, floor, medial wall, and lateral wall). The roof comprises the orbital plate of the frontal bone and the lesser wing of the sphenoid. The floor, formed mainly by the maxilla, is among the thinnest orbital walls and is the most frequently fractured. The medial wall, or lamina papyracea of the ethmoid, also serves as the lateral boundary of the ethmoid air cells. The lateral wall, formed by the zygomatic bone and greater wing of the sphenoid, is the thickest and most structurally robust.
At the orbital apex lie the optic canal and superior orbital fissure. The optic canal transmits the optic nerve (CN II) and the ophthalmic artery and veins, whereas the superior orbital fissure transmits cranial nerves III, IV, and VI, as well as the ophthalmic division of CN V. The inferomedial strut is the bony junction where the orbital floor meets the medial wall at the posterior margin of the infraorbital canal. Integrity of this strut preserves orbital volume and buttress continuity.
The orbit contains the globe, extraocular muscles, cranial nerves, retrobulbar fat, vascular structures, and the lacrimal gland. The globe consists of the following 3 concentric layers: an outer fibrous coat (cornea and sclera), a middle vascular layer (uvea), and an inner retinal layer. The lens, suspended by zonular fibers, divides the globe into anterior and posterior segments. The anterior segment is subdivided into the anterior chamber, which lies between the cornea and iris, and the posterior chamber, which lies between the iris and lens. The vitreous chamber, filled with gelatinous vitreous humor, occupies most of the globe’s volume posterior to the lens.
Orbital trauma results from blunt or penetrating mechanisms. Blunt trauma results from objects wider than the orbital aperture, such as fists, balls, or dashboards. Two theories describe fracture patterns in blunt injury. The buckling theory posits that a force to the orbital rim is transmitted along the bony walls, particularly the floor or medial wall. The hydraulic theory suggests that extrinsic orbital compression increases intraorbital pressure, fracturing at structurally weak points. Most injuries reflect elements of both mechanisms. Penetrating trauma results from objects narrower than the orbital aperture, such as knives, wires, or projectiles. These forces follow a linear trajectory, disrupting soft tissues and often injuring the globe, optic nerve, or orbital apex, with potential for intracranial extension.
Imaging modalities and protocols
Multidetector CT is the first-line imaging modality for evaluating orbital trauma. CT offers rapid acquisition, high-spatial resolution, and simultaneous assessment of osseous and soft tissue structures. Thin axial sections (≤1.25 mm) should be obtained using both bone and soft tissue algorithms. Multiplanar reformats should include coronal, sagittal, and oblique planes oriented parallel to the optic nerve. Intravenous contrast is reserved for specific indications, such as suspected vascular injury or concern for optic nerve pathologic condition. It is not routinely indicated without a defined soft tissue concern. ,, Radiation dose can be reduced substantially without loss of diagnostic utility. Lowering the tube current to 100 mA, compared with the standard 300 mA, can reduce effective dose by up to 70%.
MR imaging has a very limited role in acute orbital trauma. In the rare instance that CT is inconclusive, MR imaging can evaluate optic neuropathy, globe wall integrity, and orbital apex pathologic condition. A standard orbital protocol includes axial and coronal T1-weighted sequences, fat-saturated T2-weighted images, short tau inversion recovery (STIR) or fluid-attenuated inversion recovery, diffusion-weighted imaging (DWI), and postcontrast fat-saturated T1-weighted sequences. MR imaging is contraindicated in cases of suspected metallic foreign bodies. In acute trauma, MR imaging is further limited by scan duration, patient instability, and restricted availability. ,
Ocular ultrasound is useful for evaluating the globe and anterior orbit, provided globe integrity is preserved. High-frequency linear transducers enable real-time assessment of vitreous hemorrhage, retinal detachment, lens dislocation, and posterior scleral contour. Ultrasound should not be used when globe rupture is suspected, as probe pressure may exacerbate the injury. Ultrasound evaluation of retrobulbar structures is limited.
Conventional radiography has minimal utility in orbital trauma. Radiographs may detect radiopaque foreign bodies and displaced fractures and may suggest nondisplaced fractures when orbital emphysema or sinus air-fluid levels are present, but generally lack the sensitivity required for subtle osseous or soft tissue findings. In the absence of CT, radiographs may screen for metallic fragments before MR imaging. Caldwell and Waters views detect orbital fractures with reported sensitivities between 64% and 78% and false-negative rates up to 29%. ,
Advanced imaging techniques can supplement standard protocols in selected cases. Dual-energy CT distinguishes iodine from hemorrhage and reduces beam-hardening artifacts near metallic implants. Cinematic rendering provides enhanced three-dimensional visualization of orbital anatomy and fracture trajectories. These tools can aid surgical planning.
Orbital fracture patterns and features
Facial fractures frequently involve the orbit owing to its central position in the midface. These injuries follow predictable patterns governed by craniofacial buttress anatomy. The major classifications include Le Fort patterns, naso-orbito-ethmoid (NOE) injuries, zygomaticomaxillary complex (ZMC) fractures, and isolated orbital wall disruptions. A summary of classification systems and their relationship to orbital involvement is presented in Table 1 .
Table 1
Classification of facial fracture patterns involving the orbit
| Classification | Orbit Involved? | Notes |
|---|---|---|
| Le Fort I | No | Maxilla only |
| Le Fort II | Yes | Inferior rim and floor |
| Le Fort III | Yes | Lateral wall, floor, roof |
| ZMC | Usually | Lateral rim, floor, wall |
| NOE | Yes | Medial wall |
| Isolated floor | Yes | Blow-out, muscle herniation |
| Isolated medial | Yes | May trap medial rectus |
| Isolated roof | Sometimes | Often pediatric, possible CSF leak |
| Nasal arch | No | Unless extension |
Le Fort and Naso-Orbito-Ethmoid Fractures
The Le Fort system describes patterns of midface separation involving bilateral pterygoid plate fractures. Le Fort I is a horizontal maxillary fracture below the nasal floor. Le Fort II involves the inferior orbital rims and floors. Le Fort III traverses the orbital floor, lateral walls, and roof, detaching the midface from the cranial base. Although historically important, the Le Fort system has limited specificity for surgical planning. , Le Fort II and III fractures frequently involve the orbit and should prompt detailed evaluation of orbital walls and apex.
NOE fractures result from medial midface trauma. The Markowitz-Manson classification stratifies these fractures into 3 types based on medial canthal tendon (MCT) involvement and central fragment comminution. The MCT provides structural support for the medial eyelids and is essential for normal blink mechanics and eyelid apposition to the globe. Type I preserves the MCT on an intact fragment. Type II involves comminution with attached MCT. Type III disrupts MCT insertion entirely. These injuries often affect the medial orbital wall and roof, with potential for traumatic telecanthus and lacrimal duct injury. ,
Zygomaticomaxillary Complex Fractures
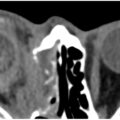
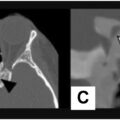
ZMC fractures involve the zygomatic bone at its articulations with the frontal, maxillary, sphenoid, and temporal bones ( Fig. 1 ). The Zingg classification distinguishes isolated arch (type A), monofragment (type B), and comminuted (type C) fractures. Displacement at the zygomaticosphenoid suture or blowout of the orbital floor may increase orbital volume, leading to enophthalmos or hypophthalmos. Axial and coronal CT should assess fragment rotation and floor continuity. Surgical repair is indicated for significant displacement or cosmetic deformity. Minimally displaced fractures may be managed conservatively.
Left ZMC fracture with globe rupture. ( A ) Lateral orbital wall fracture ( arrow ) and concomitant blowout fracture ( arrowheads ). ( B ) Rupture and flattening of the left globe ( star ). ( C ) Zygomatic arch fracture ( arrow ) and fractures of all the walls of the maxillary sinus.
Isolated Orbital Wall Fractures
Orbital floor (blowout) fractures
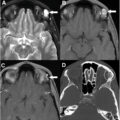
Orbital floor fractures frequently cause herniation of orbital fat or the inferior rectus muscle into the maxillary sinus ( Fig. 2 ). When the fracture disrupts the inferomedial strut, surgical repair becomes more challenging, and the risk of developing enophthalmos increases. Fractures involving the infraorbital canal or groove carry a high likelihood of infraorbital nerve injury, resulting in loss of sensation in the cheek and upper gingiva.
Left orbital floor blowout fracture. ( A ) Displaced fracture of the orbital floor ( arrow ), with preservation of the inferomedial orbital strut ( arrowhead ). ( B ) Flattening and displacement of the inferior rectus muscle ( arrow ) with clinical entrapment. ( C ) Intraconal retrobulbar hemorrhage ( star ) and asymmetric proptosis of the left globe.
Rounding or displacement of the inferior rectus muscle indicates fascial sling disruption and raises concern for entrapment. Muscle entrapment carries the risk of ischemia and fibrosis, both of which may cause lasting morbidity if diagnosis and intervention are delayed.
Several CT features predict the likelihood of clinically significant enophthalmos. These include a defect size greater than 2 cm 2, involvement of more than 25% to 50% of the orbital floor, disruption of the inferomedial strut, and herniation of more than 1.5 mL of orbital soft tissue. , Surgical repair is generally indicated for patients with persistent diplopia, documented muscle entrapment, or hypophthalmos exceeding 2 mm.
Medial wall fractures
Fractures of the medial wall (lamina papyracea) typically involve herniated fat and may compromise medial orbital wall support, resulting in enophthalmos and diplopia. Rarely, the medial rectus may be herniated. Fractures near the optic canal require careful preoperative assessment to avoid iatrogenic optic nerve injury.
Orbital roof fractures
Orbital roof fractures can violate the dura and cause cerebrospinal fluid (CSF) leak, particularly in high-energy or NOE-related trauma. Neurosurgical consultation is advised for CSF fistulas, although most resolve with conservative measures. , Surgery is generally unnecessary without CSF leak, globe displacement, or diplopia.
Orbital apex fractures
Fractures involving the orbital apex endanger the optic canal and superior orbital fissure. Bony impingement on these structures may produce traumatic optic neuropathy, which may require urgent decompression.
Pediatric considerations
Related posts:
 Orbital Imaging Modalities and Recent Updates
Orbital Imaging Modalities and Recent Updates
 Imaging of the Cavernous Sinus
Imaging of the Cavernous Sinus
 Imaging of the Globe
Imaging of the Globe
 Multidisciplinary Management of Tumors of the Orbit
Multidisciplinary Management of Tumors of the Orbit
 Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
 Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


