This article provides a comprehensive overview of imaging in the evaluation of laryngeal and hypopharyngeal squamous cell carcinomas. It highlights the critical role of computed tomography (CT), MR imaging, and PET/CT in staging, treatment planning, and surveillance. Key anatomic landmarks, patterns of tumor spread, imaging features relevant to TNM staging, and post-treatment changes are discussed. Emphasis is placed on identifying imaging findings that alter management, such as subsite evaluations, cartilage invasion, extralaryngeal extension, and regional nodal metastasis. The article also addresses common diagnostic challenges and pearls for accurate interpretation.
Key points
-
•
Understanding laryngeal and hypopharyngeal anatomy is key to assessing tumor extent, spread, and staging on cross-sectional imaging.
-
•
Cross-sectional imaging is essential for evaluating deep tumor spread, tissue invasion, and nodal disease, complementing endoscopy in staging and treatment planning.
-
•
Following therapy, imaging is essential for detecting recurrent disease and distinguishing it from expected postradiation or postsurgical changes, often requiring a multimodality approach.
Abbreviations
| CT | computed tomography |
| ENE | extranodal extension |
| NIRADS | Neck Imaging Reporting and Data System |
| tvc | true vocal cord |
Introduction
Laryngeal and hypopharyngeal squamous cell carcinomas (SCCs) account for less than 20% of head and neck cancers and predominantly affect men between the ages of 50 and 70. The primary risk factors are tobacco and alcohol use, although human papillomavirus is an emerging contributor in a subset of cases. This review focuses on the role of imaging for diagnosis, staging, and post-treatment evaluation, which plays a critical role in the choice of therapy, which is a combination of chemoradiation and surgery.
Anatomy
A thorough understanding of this complex anatomy is essential for accurately interpreting cross-sectional imaging, as the patterns of tumor spread and staging are closely tied to these distinct anatomic compartments.
The larynx serves as both the airway and the voice box, extending from the oropharynx above to the trachea below, and situated anterior to the hypopharynx. It is divided into 3 anatomic regions: the supraglottis, glottis, and subglottis. The supraglottis extends from the tip of the epiglottis to the level of the laryngeal ventricle and contains key structures including the epiglottis, aryepiglottic folds, false vocal cords, portions of the arytenoid cartilages, and the pre-epiglottic and paraglottic spaces. The glottis spans approximately 1 cm inferiorly from the laryngeal ventricle to the lower margin of the true vocal cords and includes the true vocal cords along with the anterior and posterior commissures. The subglottis lies below, extending from the undersurface of the true vocal cords to the inferior border of the cricoid cartilage ( Box 1 , Figs. 1–4 ).
Box 1
Imaging anatomy and implications
| True vocal cord (tvc) | Includes vocal ligament and thyroarytenoid muscle | Crucial for sound production. Fixation implies tumor involvement of the tvc or cricoarytenoid joint |
| Pre-epiglottic and paraglottic spaces | Anterior to epiglottis and lateral to glottis | Crucial in the spread of laryngeal malignancies; involvement upstages cancer to T3 and increases the occurrence of metastatic lymphadenopathy |
| Laryngeal saccule | Outpouching from the anterosuperior portion of laryngeal ventricle, between the vestibular fold and thyroid cartilage and contains mucous glands to lubricate vocal folds | Secondary laryngocele due to obstruction by glottic or supraglottic carcinoma |
| Conus elasticus | Fibroelastic membrane extending superiorly from cricoid to the medial margin of tvc | Acts as a relative barrier to the spread of malignancies from the glottis downward |
| Lymphatics | Supraglottis: rich in lymphatics | Prone to bilateral nodal spread |
| Glottis: sparse lymphatics | Small tumors rarely cause nodal spread | |
| Subglottis: less dense lymphatics compared with supraglottis | Drains primarily to central compartment nodes | |
| Nerve supply | Recurrent laryngeal nerve innervates all intrinsic muscles of larynx except cricothyroid muscle which is supplied by superior laryngeal nerve | The pathway of the nerves affects both the surgical approach and potential complications |
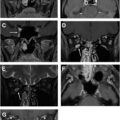
CECT of larynx. ( A ) Axial section along hyoid (h) shows transition from oropharynx to supraglottic larynx and hypopharynx. The pharyngoepiglottic folds (p) attached to the lateral aspect of epiglottis (e) separate supraglottis subsites and pyriform sinus (ps) from vallecula (v), while the median glossoepiglottic fold (g) connects epiglottis to the tongue base forming the boundary between valleculae. ( B ) Axial section along the inferior portion of hyoid (h) shows the fixed portion of epiglottis (e), hyoepiglottic ligament (hel) connecting the hyoid to the epiglottis in the midline, pre-epiglottic space fat (pes), aryepiglottic fold (ae), and pyriform sinus (ps). ( C ) Axial section along the superior portion of thyroid cartilage (t) shows paraglottic space fat (pgs) along the lateral aspect. Aryepiglottic folds (ae) separate the supraglottic larynx and pyriform sinuses (ps). ( D ) Axial section at the level of thyroid cartilage (t) shows false vocal cord with prominent paraglottic fat laterally (fvc), arytenoid cartilage (a), pyriform sinus (ps), cricoid cartilage (c), and postcricoid hypopharynx (pc). ( E ) Axial section along the lower portion of thyroid cartilage (t) shows change in the anterior contour which is less angulated, true vocal cord (tvc) attached to the vocal process of arytenoid cartilage (a), cricoid cartilage (c), and postcricoid hypopharynx (pc). ( F ) Axial section at the level of cricoid cartilage (c) shows inferior cornu of thyroid cartilage (t), posterior cricoarytenoid muscle (pcm), and apposing mucosa of the postcricoid hypopharynx and posterior wall of hypopharynx (m) flanked by submucosal fat anteriorly and posteriorly.
CECT of larynx. ( A ) Coronal reformat along the anterior portion shows hyoid (h), pre-epiglottic space with fat (pes), strap muscle (sm), thyroid cartilage (t), paraglottic space with fat (pgs), false vocal cord with fat density (fvc), true vocal cord (tvc), the laryngeal vestibule in between the true and false cords (lv), and cricoid cartilage (c). ( B ) Coronal reformat posteriorly shows greater cornu of hyoid (h), thyroid cartilage (t), lamina of cricoid (c) articulating with arytenoid (a). The corniculate cartilage (co) is above the arytenoid along the base of aryepiglottic fold (ae) with pyriform sinus (ps) laterally. Epiglottis (e) attaches laterally to the pharyngeal wall by pharyngoepiglottic fold (p). Thin paraglottic space is seen extending to the cricoid (pgs). Thyroid gland (tg).
CECT of larynx. Midsagittal ( A ) to parasagittal ( B , C ) reformats show suprahyoid epiglottis (se), infrahyoid fixed epiglottis (ie), hyoid (h), pre-epiglottic space (pes), median thyrohyoid ligament (thl), thyroid cartilage (t), anterior arch of cricoid (c), lamina of cricoid (cl), true vocal cord (tvc), false vocal cord (fvc), laryngeal ventricle (lv), arytenoid (a), aryepiglottic fold (ae), corniculate cartilage (co), and strap muscle (sm).
( A , B ) Sagittal and coronal graphics show suprahyoid epiglottis (se), infrahyoid fixed epiglottis (ie), hyoid (h), pre-epiglottic space (pes), paraglottic space (pgs), hyoepiglottic ligament (hel), median thyrohyoid ligament (thl), thyroid cartilage (t), cricothyroid ligament (ctl), anterior arch of cricoid (c), lamina of cricoid (cl), true vocal cord (tvc), thyroarytenoid muscle (tam) false vocal cord (fvc), laryngeal ventricle (lv), arytenoid (a), aryepiglottic fold (ae), and corniculate cartilage (co).
(Surjith Vattoth, Imaging Anatomy: Head and Neck, 2nd Edition, 2024, Elsevier.)
The larynx is suspended from the hyoid bone and supported by a cartilaginous framework composed of 3 unpaired cartilages (epiglottis, thyroid, and cricoid) and 4 paired cartilages (arytenoid, corniculate, cuneiform, and triticeous). The thyroid and cricoid cartilages provide the primary structural support, whereas the corniculate, cuneiform, and triticeous cartilages, though part of the framework, have limited clinical significance ( Box 2 , see Figs. 1–4 ).
Box 2
Cartilages and clinical significance
| Cartilages | Features | Clinical Significance |
|---|---|---|
| Thyroid | Shield shaped-lamina, superior and inferior cornua, offers pathway for tumor spread through attachments like the thyrohyoid membrane to hyoid | Protects vocal cords, essential for voice production; tumor invasion here can affect voice and require complex treatment approaches |
| The vocal ligaments attach anteriorly to the inside of the thyroid cartilage | Lack of perichondrium at the site of attachment and relatively narrow distance between the mucosa and thyroid cartilage increase the vulnerability for tumor invasion | |
| Cricoid | Signet ring shaped, only complete ring of cartilage, provides foundational support for the larynx. Cricothyroid membrane connects to thyroid cartilage | Involvement in tumors often precludes voice preservation surgeries due to its structural role in the larynx |
| Epiglottis | Leaf-shaped stalk (petiole) and free portion. Perforations in the cartilage is susceptible to tumor invasion. Hyoepiglottic and thyroepiglottic ligament connects to hyoid and thyroid cartilage | Closes the laryngeal inlet preventing food entry into the airway during swallowing; its invasion by tumors can compromise this function |
| Arytenoid | Pyramid-shaped base, vocal process, lateral process and apex. Articulates with the cricoid via synovial joints | Key for vocal cord functionality; changes or invasions here can affect voice modulation and breathing |
The hypopharynx links the oropharynx to the esophagus and communicates directly with the laryngeal inlet. It begins at the posterior aspect of the pharyngoepiglottic folds, near the inferior margin of the hyoid bone, and extends inferiorly to the cricopharyngeus muscle, which encircles the junction between the hypopharynx and the esophagus at the level of the cricoid cartilage (see Figs. 1–4 ).
Anatomically, the hypopharynx is subdivided into 3 principal subsites: the pyriform sinuses, the posterior wall, and the postcricoid region (see Fig. 1 ). The pyriform sinuses create bilateral recesses that envelop the larynx. Each pyriform sinus extends from the pharyngoepiglottic folds inferiorly to the level of the true vocal cords, bordered medially by the aryepiglottic folds and laterally by the thyroid cartilage and thyrohyoid membrane. The posterior hypopharyngeal wall is a direct continuation of the posterior wall of the oropharynx, while the postcricoid region represents the lower anterior hypopharyngeal wall, situated posterior to the cricoid cartilage and collapsing against the posterior wall when not distended. From a clinical perspective, tumors involving the posterior wall are particularly aggressive, with a higher propensity for bilateral cervical lymph node metastases.
Imaging techniques
Imaging plays a crucial role in determining the extent of the tumor, its spread to nearby tissues or organs, and the presence of metastases. The role of the commonly used imaging is summarized in Box 3 .
Box 3
Overview of imaging modalities
| Imaging Modality | Advantages | Disadvantages | Usage |
|---|---|---|---|
| Computed tomography (CT) |
Widely available
Fast imaging time that mitigates patient’s motion High resolution for assessing cartilage invasion and lymph nodes |
Suboptimal soft tissue contrast
Equivocal thyroid cartilage invasion due to age-related variations in cartilage mineralization |
Commonly first imaging choice |
| MR imaging |
Superior soft tissue contrast
Multiparametric tissue characterization For assessment of prevertebral space, esophageal involvement |
Longer imaging time that is prone to motion artifact | Often used in equivocal CT assessment of cartilage or paraglottic space invasion and tumor delineation that is crucial for surgical or radiation planning |
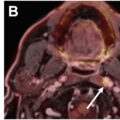
| FDG PET-CT or PET-MR imaging | Metabolically active tumors, regional and distant metastases that is undetectable by CT/MR imaging | False positive of inflammation | In advanced disease, treatment response assessment and detecting recurrence |
| Ultrasound | Useful in evaluating vocal cord mobility and lymph nodes | Operator-dependence | Valuable for assessing and guiding biopsy of suspicious lymph nodes |
Each imaging technique has its strengths and limitations, and often complementary to provide a comprehensive assessment. The choice of imaging often depends on the stage of the disease, the patient’s condition, and institutional preferences with the aims for accurate staging, appropriate treatment plan, and predicting prognosis. Both computed tomography (CT) and MR imaging should be tailored to the relevant anatomy, and the specific clinical question, utilizing a combination of both standard and available advanced techniques (dual energy, diffusion-weighted imaging, contrast-enhanced perfusion imaging, arterial spin labeling techniques when available). Some of these advanced techniques will be covered by other authors in this issue.
Tumor staging
Imaging evaluation of laryngeal and hypopharyngeal SCC requires a thorough understanding of the AJCC TNM staging—the extent of the main tumor (T), the spread to nearby lymph nodes (N), and distant metastasis (M). The initial clinical staging relies on presurgical assessments (physical examinations, imaging), while the pathologic staging is determined by examining the resected tissue from the surgery.
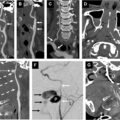
The stages of laryngeal and hypopharyngeal cancers are slightly different and are summarized in Boxes 4 and 5 . In laryngeal cancer, key detections that upstage to T3 disease are any of these findings: fixation of vocal cord; invasion of the pre-epiglottic and/or paraglottic space; invasion of the inner cortex of thyroid cartilage. Tumor erosion of the outer cortex of thyroid cartilage, tumor involvement of the cricoid, and/or extralaryngeal soft tissue further upstages to T4a disease. Both laryngeal and hypopharyngeal T4b is generally considered unresectable disease when tumor invades the prevertebral space, mediastinum, and/or encases the carotid.
Box 4
Laryngeal carcinoma staging
Adapted from Itamura K, Hsue VB, Barbu AM, et al. Diagnostic assessment (imaging) and staging of laryngeal cancer. Otolaryngol Clin N Am 2023;56(2):215–31.
-
TX and Tis
-
TX and Tis are the same for all 3 sites of the larynx
-
•
TX : primary tumor cannot be assessed
-
•
Tis : carcinoma in situ
-
•
-
T1, T2, and T3
-
T1 through T3 are defined differently by laryngeal site:
-
Supraglottis
-
•
T1 : limited to one subsite of supraglottis, with normal vocal cord mobility:
-
○
Suprahyoid epiglottis
-
○
Aryepiglottic folds, laryngeal aspect
-
○
Infrahyoid epiglottis
-
○
False vocal cords (ventricular folds/bands)
-
○
Arytenoids
-
○
-
•
T2 : invades mucosa of more than one adjacent area, with normal vocal cord mobility:
-
○
Subsite of supraglottis
-
○
Glottis
-
○
Region outside supraglottis, for example, base of tongue, vallecula, medial wall of pyriform sinus
-
○
-
•
T3 : limited to larynx with vocal cord fixation and/or invasion of any of the following:
-
○
Inner cortex of thyroid cartilage
-
○
Paraglottic space
-
○
Pre-epiglottic space
-
○
Postcricoid area
-
○
-
•
-
Glottis
-
•
T1 : limited to vocal cord(s) with normal vocal cord mobility (may involve anterior or posterior commissure)
-
○
T1a : limited to one vocal cord
-
○
T1b : involves both vocal cords
-
○
-
•
T2 : extends to supraglottis and/or subglottis, and/or with impaired vocal cord mobility
-
•
T3 : limited to larynx with vocal cord fixation and/or invasion of paraglottic space and/or inner cortex of thyroid cartilage
-
•
-
Subglottis
-
•
T1 : limited to subglottis
-
•
T2 : extends to vocal cord(s) with normal or impaired vocal cord mobility (no cord fixation)
-
•
T3 : limited to larynx with vocal cord fixation and/or invasion of paraglottic space and/or inner cortex of thyroid cartilage
-
•
-
T4
-
T4 is the same for all 3 sites of the larynx:
-
•
T4 : moderately or very advanced
-
○
T4a : moderately advanced local disease:
-
▪
Invades through outer cortex of thyroid cartilage
-
▪
Invades cricoid cartilage
-
▪
Invades tissues beyond the larynx (eg, trachea, deep extrinsic muscles of the tongue, strap muscles, thyroid gland, esophagus)
-
▪
-
○
T4b : very advanced local disease:
-
▪
Invades the mediastinum
-
▪
Invades the prevertebral space
-
▪
Encases the carotid artery
-
▪
-
○
-
•
-
Regional lymph node (N)
-
Regional nodal status is defined the same as for most other cancers of the head and neck. See the main article, cervical lymph node (staging).
-
-
Distant metastases (M)
-
The following categories may be used, either in the clinical classification (c) for patients with cancer identified before treatment and/or in the pathologic classification (p) for patients for whom surgery is the first definitive therapy:
-
•
cM0 : no evidence of metastases
-
•
cM1 : distant metastasis
-
•
pM1 : distant metastasis, microscopically confirmed
-
•
-
-
Clinical nodal status (cN)
-
Clinical criteria apply for patients treated nonsurgically, without cervical lymph node dissection. Clinical evaluation synthesizes information from such sources as physical examination, imaging, and fine-needle aspiration.
-
•
NX : nodes cannot be assessed
-
•
N0 : no regional node metastases
-
•
N1 : metastasis in single ipsilateral node, ≤3 cm, and no extranodal extension (ENE(−))
-
•
N2
-
○
N2a : metastasis in single ipsilateral node, >3 cm and ≤6 cm, and ENE(−)
-
○
N2b : metastasis in multiple ipsilateral nodes, all ≤6 cm, and ENE(−)
-
○
N2c : metastasis in bilateral or contralateral nodes, all ≤6 cm, and ENE(−)
-
○
-
•
N3
-
○
N3a : metastasis in a node, >6 cm, and ENE(−)
-
○
N3b : metastasis in a node with clinically overt ENE(+) (ENE c )
-
○
-
•
-
-
Pathologic nodal status (pN)
-
Pathologic criteria apply for patients treated surgically, with cervical lymph node dissection, for whom multiple whole lymph nodes are available for microscopic evaluation.
-
•
NX : nodes cannot be assessed
-
•
N0 : no regional node metastases
-
•
N1 : metastasis in single ipsilateral node, ≤3 cm, and no extranodal extension (ENE(−))
-
•
N2
-
○
N2a : metastasis in single ipsilateral node, >3 cm and ≤6 cm, and ENE(−); or metastasis in single ipsilateral node, ≤3 cm, and ENE(+)
-
○
N2b : metastasis in multiple ipsilateral nodes, all ≤6 cm, and ENE(−)
-
○
N2c : metastasis in bilateral or contralateral nodes, all ≤6 cm, and ENE(−)
-
○
-
•
N3
-
○
N3a : metastasis in a node, >6 cm, and ENE(−)
-
○
N3b : metastasis in single ipsilateral node, >3 cm, and ENE(+); or multiple ipsilateral, contralateral, or bilateral nodes any with ENE(+); or single contralateral node of any size and ENE(+)
-
○
-
•
-
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


