Cancer is a leading cause of death and disability in children and adolescents with an estimated worldwide annual incidence of 400,000 new cases each year. Pediatric cancers in the head and neck include tumors that arise in tissue specific to the region such as retinoblastoma, salivary gland neoplasms, and thyroid carcinoma along with cancers that can occur elsewhere in the body. Imaging plays an essential role and modalities routinely employed depend on tumor type and location. These include postcontrast computed tomography (CT), precontrast and postcontrast MR imaging and PET-CT. PET-MR may also be utilized when available.
Key points
-
•
Pediatric neck masses are often benign. Nonetheless, a persistent or enlarging mass should be evaluated with imaging to assess for possible malignancy.
-
•
Computed tomography (CT), MR, and PET-CT are utilized in pediatric tumors of the head and neck for evaluation of tumor extent, staging, and surveillance.
-
•
Incidentally discovered thyroid nodules in a child have a higher rate of malignancy compared to adults, and these lesions should be evaluated with ultrasound.
-
•
Horner’s syndrome, persistent sinus symptoms, and new cranial nerve deficit should be worked up to rule out cervical neuroblastoma, paraspinal neuroblastoma, or parameningeal rhabdomyosarcoma.
-
•
MR imaging is the preferred modality for all patients presenting with a palpable salivary gland mass.
Abbreviations
| 3D | 3 dimensional |
| BL | Burkitt lymphoma |
| CT | computed tomography |
| GNB | Ganglioneuroblastoma |
| HL | Hodgkin lymphoma |
| IDRFs | image-defined risk factors |
| LCH | Langerhans cell histiocytosis |
| MIBG | I-123 metaiodobenzylguanidine |
| NB | Neuroblastoma |
| NHL | non-Hodgkin lymphoma |
| RMS | Rhabdomyosarcoma |
| US | ultrasound |
Introduction
Cancer is a leading cause of death and disability in children and adolescents with an estimated worldwide annual incidence of 400,000 new cases. It is estimated that up to 12% of pediatric cancers involve the head and neck. , Pediatric cancers in the head and neck include tumors that arise in tissue specific to a region such as retinoblastoma, salivary gland neoplasms, and thyroid carcinoma along with cancers that can occur elsewhere in the body to include sarcomas and lymphomas. Nasopharyngeal carcinoma, which can occur in the second decade of life, has similar features to nasopharyngeal carcinoma in adults, discussed in the article “Update on Nasopharyngeal Cancer” by Dr. Nancy Fischbein. Imaging plays an essential role and modalities routinely employed depend on tumor type and location. These include postcontrast computed tomography (CT), precontrast and postcontrast MR imaging and PET-CT. PET-MR may also be utilized when available.
Spectrum of pediatric head and neck malignancies
Lymphoma
In the pediatric population, lymphoma is the most common malignant tumor in the head and neck. Lymphomas are divided into Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL), each having unique presentations. Treatment advances during the last 3 decades have led to improved survival with cure rates exceeding 90%.
For both cancer subtypes, imaging playing a crucial role in cancer diagnosis, staging, and treatment surveillance. Contrast-enhanced CT is a main imaging modality for defining extent of disease in pediatric lymphomas. MR imaging is preferred if there is central nervous system or skull base involvement. Imaging of all areas with disease is imperative for staging and is accomplished with CT, MR imaging, and PET. Surveillance also utilizes both PET-CT and cross-sectional imaging (CT or MR imaging).
HL is the most common pediatric malignancy in children aged 15 to 19 years. Clinical features at presentation include lymphadenopathy and/or mediastinal mass with or without B symptoms (fatigue, weight loss, and fevers). Children frequently present with painless adenopathy involving cervical and axillary nodal groups. HL arises from B lymphocytes and at histopathology is divided into classic (90%) and lymphocyte predominant subtypes. Epstein- Barr virus (EBV) is implicated in up to 50% of the classic subtype in developed countries and a higher percentage in developing countries.
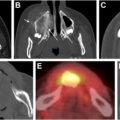
Cross-sectional imaging can strongly suggest the diagnosis, which is subsequently confirmed by histopathological analysis of tissue. Imaging can help guide surgeons in planning lymph node excision, which is the preferred method for diagnosis if percutaneous image-guidance biopsy is not definitive. Imaging findings in the neck are dominated by the presence of moderate to markedly enlarged cervical lymph nodes ( Fig. 1 A–C). Although there is no exact size measurement to discriminate these from reactive nodes, they are often very large, persistent, and have a predilection for the lower neck. In pediatric patients, bulky disease is defined as lymph nodal conglomerates 6 cm or greater, which places the patient into higher risk disease categories.
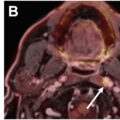
Hodgkin lymphoma. ( A ) Coronal CECT neck of a 16 year old girl shows large round homogeneous lymph nodes in the inferior right neck involving level III and IV as well as the left mediastinum ( arrows ) ( B ) Axial and coronal CECT neck of a 9 year old boy show nodal conglomerate ( asterisk ) measuring 8 cm (caliper), consistent with bulk disease in the left neck. Coronal PET-CT demonstrates increased fluorodeoxyglucose (FDG) uptake ( arrow ). ( C ) Axial CECT neck and coronal PET-CT of a 17 year old girl show adenopathy ( arrows ) in mediastinum and bilateral lower neck (levels III, IV, and VB) with increased FDG uptake. Coronal PET-CT surveillance at 2 years (far right image) shows no evidence of FDG-avid tumor residual or recurrence.
These nodes are often bland and low in attenuation but can be heterogeneous. HL typically involves contiguous nodal groups and may be unilateral or bilateral. It has a high propensity for internal jugular nodes (levels II–IV) and nodes in the lower neck (levels IV and VB) with or without contiguous involvement of mediastinal nodal groups. PET-CT is routinely utilized for staging.
Treatment of HL is now based on the paradigm of response-based treatment adaptation in order to decrease or eliminate radiotherapy and reduce chemotherapy, while preserving high cure rates. , Assessment of treatment response is established with PET-CT.
NHL is a diverse group of malignancies arising from T, B, and natural killer cell lineage with the majority having B cell origin in the head and neck. Unlike adults, who can develop low-grade disease, most cases in children are higher grade with aggressive clinical behavior. In contrast to HL, NHL can result in noncontiguous enlargement of cervical lymph nodes and can arise in nonnodal tissue.
Burkitt lymphoma (BL) is the most common pediatric NHL. These are B-cell lymphoma, which are highly proliferative with a short doubling time, most often presenting with a rapidly growing mass. These tumors harbor the MYC gene rearrangement. Traditionally they have been divided into endemic, sporadic, and immunodeficiency-associated BL; however, recent evidence suggests the presence of EBV might have better correlation with BL molecular features. BL can present in the abdomen. Sites of involvement in the head and neck include the jaw, other facial bones, lymph nodes, and Waldeyer’s ring. Other major NHL subtypes encountered in pediatric patients include diffuse large B-cell lymphoma, along with B-cell and T-cell lymphoblastic lymphomas. ,
NHL has a more varied presentation compared to HL, and MR imaging is often performed to characterize the lesions and suggest the diagnosis. These lesions, which can be nodal or extranodal in the head and neck, have intermediate T2, contrast enhancement, and low apparent diffusion coefficient (ADC) values ( Fig. 2 A, B).
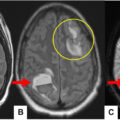
Burkitt lymphoma. ( A ) Axial CECT neck of a 10 year old boy with large tumor involving nasopharynx, oropharynx, and left masticator space ( asterisk ). There was erosion of the pterygoid plates and left basiocciput ( arrows ). Follow-up CT on day 11 demonstrates a rapid response to chemotherapy. The mass is decreased in size and attenuation ( arrowhead ). ( B ) Axial T2WI, postcontrast fat-suppressed coronal T1WI and axial ADC MR of the orbit in a 16 year old boy with multifocal disease at presentation. There is intraconal orbital disease ( arrows ) along the optic nerve sheath on the right. The tumor has mild contrast enhancement and low ADC ( arrows ).
Rhabdomyosarcoma
Rhabdomyosarcoma (RMS) is the most common pediatric soft tissue sarcoma accounting for 4.5% of all malignancies. The majority (72%–81%) of the children are less than 10 years old at the time of presentation. Approximately 35% involve the head and neck, making it the most common sarcoma to affect the head and neck. ,
RMS is a high-grade malignancy composed of small round blue cells at histopathology. There are 2 major subtypes. The more common embryonal subtype (70%) occurs in younger patients and has a better prognosis. RMS in the head and neck is most often the embryonal subtype and rarely involves regional lymph nodes. The less common alveolar subtype can further be categorized as fusion positive (fusion of the PAX3 or PAX7 gene with FOXO1 ), which accounts for 60% to 80% of cases and portends a worse prognosis. The fusion-negative tumors have a favorable outcome. ,
Additionally, tumor staging, management, and prognosis depend on whether the site of tumor is orbital, parameningeal (which include the nasopharynx/nasal cavity, paranasal sinuses, infratemporal and pterygopalatine fossae, as well as the middle ear), or all other head and neck locations. , Orbital and nonparameningeal sites have a favorable prognosis. Clinical presentation varies with location but often is related to a rapidly growing soft tissue mass. Orbital RMS often presents with a palpable lesion resulting in earlier diagnosis and favorable treatment response. Orbital RMS may mimic more benign pathologies at cross-sectional imaging, as it may demonstrate bone remodeling rather than resorption/destruction. Parameningeal RMS can result in nonspecific symptoms that make early diagnosis difficult. A new cranial nerve deficit or persistent sinus symptoms in a child warrants immediate evaluation as this can be the initial manifestation of a parameningeal RMS tumor. ,,
Imaging plays an important role for tumor diagnosis, establishing lesion extent and in detecting metastatic disease. MR imaging provides higher soft tissue resolution. T2 weighted imaging (T2WI), and diffusion weighted imaging (DWI)/ADC maps are helpful in evaluating lesion cellularity. RMS typically presents as a solid enhancing mass with hypercellularity evident by decreased diffusivity and low ADC ( Fig. 3 A–C). Intermediate or high ADC may be also encountered especially in lesions of the orbit. MR imaging is superior for detecting dural invasion, perineural spread, and bone marrow involvement, while CT provides greater detail of osseous changes or erosion. PET-CT plays an important role in initial staging with improved detection of metastatic disease. , Standardized image acquisition and interpretation with awareness of staging guidelines among pediatric oncologists, radiologists, and nuclear medicine physicians is important for optimal care.
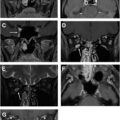
Rhabdomyosarcoma. ( A ). Orbital RMS, fusion negative in a 4 year old patient. There is a well-circumscribed nodule in the left upper eyelid demonstrating peripheral enhancement at postcontrast CT ( arrow ). The lesion has intermediate signal on fat-supressed axial T2WI along with low ADC ( arrows ). Postcontrast axial and coronal fat-suppressed T1WI show solid enhancement ( arrows ). ( B ) Orbital embryonal RMS. There is an intraconal and extraconal mass in the inferolateral right orbit. CT demonstrates benign appearing bone remodeling ( arrow ). Fat suppressed axial T2WI shows lesion hyperintensity ( arrow top right ). Mild enhancement is noted on postcontrast fat-suppressed axial T1WI ( arrow ). There is marked decrease ADC ( arrow ). ( C ) Parameningeal RMS, FOX01 fusion negative in a 7 year old patient. Large mass centered on left pterygopalatine fossa with extension into pharyngeal mucosal space, masticator space, skull base, and orbit. Intracranial disease and V3 involvement are also noted on fat-suppressed coronal T2WI and postcontrast fat-suppressed coronal T1WI ( arrows ). There is associated lytic bone destruction of the sphenoid skull base ( asterisk ) and left mandibular ramus ( arrowhead ). Orbit extension is visualized on the postcontrast coronal T1WI ( arrow bottom right ).
Treatment includes chemotherapy and local control in the form of surgery and/or radiation. Surgical feasibility is determined by site of lesion. Known poor prognostic markers include large tumor size and invasiveness, incomplete surgical removal of primary tumor, metastatic disease, and the presence of FOX01 fusion. At surveillance, precontrast and postcontrast MR imaging is utilized for evaluation of the primary site. PET-CT plays a role in determining residual masses that would benefit from second look surgery as well as determining the presence of new disease.
Neuroblastoma
Neuroblastic tumors arise from the sympathetic nervous system and include neuroblastoma (NB), ganglioneuroblastoma (GNB), and ganglioneuroma. Of these, NB is the most immature and aggressive tumor. GNB occurs in older children and has intermediate malignant potential and is composed of both mature gangliocytes and immature neuroblasts. NB is the most common extracranial tumor in the first 2 years of life. NB is a malignancy composed of small round blue cells of neural crest origin. Schwannian stromal cells are also noted at histopathology. The MYCN oncogene is a major molecular feature of NB. Congenital or antenatal NB can occur rarely, and these tumors tend to have a good prognosis. , In the head and neck, cervical NB presents clinically with palpable neck mass, Horner’s syndrome, difficulty swallowing, or stridor. ,
Treatment depends on stage and tumor risk category and often includes surgery and chemotherapy. Autologous hematopoietic stem-cell transplant is a treatment option for high-risk tumors.
Image-defined risk factors (IDRFs) are features that are associated with a high risk of surgical complications and form an integral part of the International Neuroblastoma Risk Group Staging System, which was established in 2009. IDRFs for primary cervical NBs include encasement of vessels (carotid arteries, vertebral artery, or internal jugular vein), compression of the trachea, or extension to the skull base. In the lower neck, cervicothoracic NBs arise from the stellate ganglion and are located above the subclavian artery. IDRFs at this location include compression of the trachea along with encasement of the subclavian vessels, common carotid artery, vertebral artery, the internal jugular vein, and/or the brachial plexus nerve roots. The extent of metastatic disease at presentation is the most important factor for determining patient outcome. Other high-risk features include MYCN amplification and age older than 18 months.
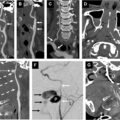
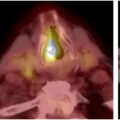
At imaging, NB has intermediate T2 signal, decreased diffusivity/low ADC, and avid enhancement on MR imaging. Calcifications are common, and hemorrhage and necrosis can also be seen. Location is an important clue to the diagnosis, as cervical NBs arise from the cervical sympathetic chain, which lies posteromedial to the carotid space. , This results in anterolateral displacement of carotid space vessels ( Fig. 4 A–C). Intense uptake on I-123 metaiodobenzylguanidine (MIBG) scan may be seen and plays an important role in detecting metastatic disease. A normal result does not exclude the diagnosis, as approximately 30% of NBs are MIBG negative. When imaging patients that present with Horner’s syndrome, it is important to look carefully along the posterior carotid space. Metastases are relatively common, particularly to the orbit, skull base, mandible, and calvarium. Metastatic osteolytic lesions often show aggressive “hair on end” periosteal reaction on CT.
Related posts:
 18-FDG-PET Imaging in Head and Neck Cancer: Current Application
18-FDG-PET Imaging in Head and Neck Cancer: Current Application
 Update on Imaging of Nasopharyngeal Carcinoma
Update on Imaging of Nasopharyngeal Carcinoma
 Immunotherapy and Targeted Therapy Considerations in Head and Neck Oncology
Immunotherapy and Targeted Therapy Considerations in Head and Neck Oncology
 Imaging Insights into Perineural Tumor Spread
Imaging Insights into Perineural Tumor Spread
 Imaging of Jaw Lesions
Imaging of Jaw Lesions
 Imaging of Laryngeal and Hypopharyngeal Squamous Cell Cancers
Imaging of Laryngeal and Hypopharyngeal Squamous Cell Cancers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


