Neoplasms in the temporal bone range from frequently encountered lesions such as vestibular schwannomas, to rare carcinomas. Knowledge of the intricate imaging anatomy of the temporal bone as well as key imaging features of each lesion aids in diagnosis and forming an appropriate differential diagnosis. Advances in imaging and treatment options continue to improve our understanding of these lesions and diagnostic capabilities.
Key points
-
•
Temporal bone neoplasms tend to arise in characteristic locations, aiding in their diagnosis.
-
•
Many neoplasms have typical imaging characteristics that can help narrow a differential diagnosis.
-
•
Imaging advances such as dynamic contrast-enhanced MR imaging can help diagnose lesions when distinguishing lesion features are absent or overlap.
-
•
Mapping of lesion extent remains a key function of the radiologist and aids in treatment planning and prognostication.
Abbreviations
| CN | cranial nerve |
| CPA | cerebellopontine angle |
| DCE-MRI | dynamic contrast-enhanced Magnetic Resonance imaging |
| EAC | external auditory canal |
| ELST | endolymphatic sac tumor |
| FOV | field of view |
| IAC | internal auditory canal |
| SRS | stereotactic radiosurgery |
| SSTR2 | somatostatin-2 receptor |
| VHL | Von-Hippel Lindau |
| VS | vestibular schwannoma |
| WI | weighted images |
Introduction
Neoplasms in the temporal bone range from frequently encountered lesions such as vestibular schwannomas (VSs), to rare carcinomas. Knowledge of the intricate imaging anatomy of the temporal bone and key lesion characteristics aids in diagnosis and formation of an appropriate differential diagnosis. Accurate lesion mapping is also crucial for treatment and surgical planning, and patient counseling, particularly with respect to facial nerve function and hearing preservation.
Imaging techniques
Temporal bone computed tomography (CT) and contrast-enhanced magnetic resonance imaging (MRI) remain the 2 primary modalities for imaging temporal bone neoplasms; however, functional imaging with molecular radiotracers such as 68 Ga-Dotatate positron emission tomography (PET), dynamic contrast-enhanced MRI (DCE-MRI), and photon counting detector CTs have made rapid advances in our ability to visualize and diagnose temporal bone neoplasms.
MRI is often preferred for imaging of neoplasms due to its superior soft tissue contrast, visualization of cranial nerves (CNs), meninges, and the brain parenchyma; however, the intricate anatomy of the temporal bone makes high resolution CT imaging particularly useful to identify the precise location of a lesion and its relationship to nearby critical structures.
The internal auditory canal (IAC) contrast-enhanced MR imaging protocol at our institution includes 5-mm slice thickness axial whole brain DWI/ADC, T2, FLAIR, and DCE GRASP sequences, as well as 3-mm small field of view (FOV) axial precontrast and axial postcontrast T1-weighted images (WI) with fat saturation, and coronal postcontrast T1-WI without fat saturation through the temporal bone. A 3-dimensional high-resolution heavily T2-weighted sequence (constructive interference in steady state [CISS] or other “cisternographic” sequence) with 0.6 to 0.8 mm axial, coronal, and sagittal reformats is obtained for visualization of the CNs and vestibulocochlear complexes. A small FOV axial and coronal multishot echoplanar DWI sequence is included if there is concern for cholesteatoma.
Since becoming available at our institution, photon counting CT has rapidly become the preferred imaging technique for temporal bone CT over conventional energy-integrating detector scanners due to its superior spatial resolution, radiation dose and noise reduction, and ability to clearly demonstrate minute anatomic structures. , When available, our protocol includes 2-mm slice thickness bone kernel images of the right and left temporal bone in the axial, coronal, and Pöschl planes, and large FOV images in a soft tissue kernel.
The choice of initial imaging study is not always straightforward. Symptomatology including hearing loss, facial nerve dysfunction, dizziness, vertigo, otalgia, otorrhea, and pulsatile tinnitus can be present across a range of benign, malignant, and non-neoplastic processes. Contrast enhanced MR imaging is usually an appropriate initial imaging strategy for unilateral facial nerve dysfunction, sensorineural hearing loss, or vertigo; whereas temporal bone CT is usually more appropriate as an initial study for conductive hearing loss. ,
Important imaging findings in the description of temporal neoplasms include the relationship of the lesion to the CNs, in particular CN VII and VIII; vascular structures including the petrous internal carotid artery, sigmoid sinus, and jugular bulb; inner, middle, and outer ear structures; and intracranial compartment including the dura and brain parenchyma.
Schwannomas
Schwannomas are benign neoplasms of Schwann cells lining peripheral nerves. They can be encountered in several locations in and around the temporal bone depending on the CN involved, the most common being VSs arising from the vestibular nerve. Schwannomas typically follow the expected course of a CN. CT may demonstrate smooth osseous expansion and remodeling of a CN canal or foramen due to the slow growth of schwannomas. Common imaging features on MR imaging include well-circumscribed margins, intermediate to high T2 signal, and postcontrast enhancement; however, intralesional hemorrhage and cystic components can lead to a more complex appearance with intrinsic T1 hyperintensity, low T2 signal, and heterogenous enhancement. Internal flow voids or matrix mineralization should suggest an alternative diagnosis. The presence of more than one schwannoma should prompt evaluation for neurofibromatosis type 2 or schwannomatosis.
Vestibular Schwannomas
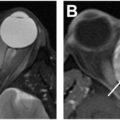
VSs are most commonly encountered within the IAC when small, and extend medially into the cerebellopontine angle (CPA) cistern when larger, resulting in a classic ice cream cone-type appearance ( Fig. 1 ). VSs may be found incidentally on imaging, or can present with symptoms including unilateral hearing loss, dizziness or imbalance, and tinnitus. IAC protocol MR imaging is the study of choice for a suspected VS.
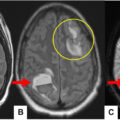
Vestibular schwannomas. Axial postcontrast T1-WI ( A ), axial T2-WI ( B ), and axial FLAIR ( C ) demonstrate a solidly enhancing mass in the left IAC extending into the CPA cistern with mass effect on the left brachium pontis and adjacent parenchymal edema ( arrow in C). Preserved CSF fluid signal is noted at the fundus of the IAC ( arrow in B). Axial postcontrast T1-WI ( D ) demonstrates a VS with a partially cystic component ( arrow ). Axial postcontrast T1-WI pretreatment ( E ) and post-SRS ( F ) demonstrate more heterogeneous enhancement and new areas of nonenhancement ( arrow ) following radiosurgery. Axial CISS ( G ), axial postcontrast T1-WI ( H ) and FLAIR ( I ) demonstrate a large VS with heterogeneous signal and enhancement on initial imaging ( G and H ), absence of fluid signal at the fundus of the IAC ( arrow in G), and asymmetric increased signal within the ipsilateral cochlear. The patient had advanced hearing loss at presentation and underwent resection of the lesion.
Description of the lesion should include the presence or absence of extension into the CPA cistern, and if present, the degree of mass effect on the brain parenchyma and any adjacent parenchymal signal abnormality.
Other relevant imaging features can include the presence of preserved cerebrospinal fluid (CSF) signal at the fundus of the IAC. This was shown to be associated with improved rates of hearing preservation following surgical resection by some authors, , but not others ; however, the presence of a fundal fluid “cap” may still have prognostic implications as it can allow for decreased radiation dose to the inner ear in patients treated with stereotactic radiosurgery (SRS).
The presence of intralesional cystic components was described in some series to be associated with worse post-treatment outcomes ,, ; however, this has not been uniformly demonstrated. ,,
Ipsilateral signal change in the cochlea should also be noted when present. Decreased T2 signal, and hyperintense FLAIR or postcontrast FLAIR signal have been associated with pretreatment and post-treatment hearing impairment, possibly related to increased inflammatory protein content in the cochlear perilymph ( Fig. 1 ). ,,,
Treatment options for VSs include surgical resection, SRS, and surveillance with serial imaging for small and incidentally found lesions.
Radiosurgery is now widely used for treatment of VSs. Increase in tumor size, intratumoral hemorrhage, cystic change, and decreased enhancement can be expected findings following SRS. , Tumor enlargement can occur up to 3 years post-SRS; however, continued growth beyond that likely represents true tumor progression. Some authors advocate for follow-up imaging only 12 months after SRS.
Surveillance imaging without intravenous contrast using a high-resolution T2-weighted sequence has been shown to be equivalent to traditional precontrast and postcontrast imaging by several authors. ,, This abbreviated protocol should be considered to reduce unnecessary gadolinium contrast exposure and decrease imaging time and cost.
Imaging pitfalls for the diagnosis of small VSs can include focal enhancement of the vestibular ganglion, or Scarpa’s ganglion, in the IAC fundus, typically encountered on high-resolution postcontrast sequences. No corresponding filling defect should be seen on high-resolution T2-WI. , Other much less common lesions described in the IAC including cavernous malformations, meningiomas, and non-vestibular schwannoma, are typically difficult to distinguish from VSs. ,, The presence of a dural tail, adjacent hyperostosis, or secondary involvement of the IAC can help differentiate meningiomas from larger VSs in the CPA cistern.
Facial Nerve Schwannomas
Facial nerve schwannomas are far less common than VS, and may cause some diagnostic uncertainty if the radiologist is unfamiliar with atypical appearances ( Fig. 2 ). Contrary to smooth bone remodeling seen along most schwannoma, facial nerve schwannomas involving the mastoid segment may appear to have irregular, aggressive osseous margins due to fracture of adjacent mastoid septa. The most common segment of involvement is the geniculate ganglion. Patients may present with facial nerve dysfunction, conductive or sensorineural hearing loss, vertigo, and tinnitus depending on the size and location of the lesion. Surveillance with serial imaging is the most common strategy for patients with none to moderate facial nerve dysfunction (House-Brackman score 1–3). Other options include SRS, surgical decompression, subtotal resection, or complete resection with nerve grafting.
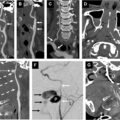
Facial nerve schwannoma. Axial ( A ), coronal ( B ), and axial ( C ) noncontrast CT through the temporal bones demonstrate smooth gradual expansion of the tympanic facial nerve canal ( arrow in A). The expanded facial nerve extends partially over the oval window and directly abuts the stapes ( arrow in B) resulting in conductive hearing loss. More significant expansion is seen at the level of the mastoid segment with irregular appearing osseous margins as the lesion interrupts adjacent mastoid septa ( arrow in C). Extension into the EAC ( dashed arrow in C) and jugular foramen ( double arrow in C) is noted. Coronal T2 ( D ), axial T2 ( E ), and coronal postcontrast T1-WI ( F ) of the same lesion demonstrate relative T2 hyperintensity with lobular margins and solid postcontrast enhancement extending through the stylomastoid foramen (faintly visible on the left for comparison— arrows in F). The patient underwent surgical resection of the lesion and facial nerve reanimation following progressive growth after SRS.
Low-flow venous vascular malformations of the facial nerve can be difficult to distinguish from facial nerve schwannomas clinically and on imaging, particularly if small. These lesions also commonly involve the geniculate ganglion due to the density of the perineural vascular plexus at this location; however, lesions do not typically extend along the course of the facial nerve. A honeycomb or spiculated appearance on CT is a key imaging feature of this lesion, similar to other osseous “hemangiomas,” and can help distinguish it from a facial schwannoma ( Fig. 3 ).
Slow flow venous vascular malformation of the facial nerve. Axial postcontrast T1-WI ( A ), axial ( B ), and coronal ( C ) noncontrast CT demonstrate an enhancing lesion ( A ) in the temporal bone. CT demonstrates a lobular lesion centered at the geniculum of the facial nerve canal without longitudinal extension along the course of the facial nerve canal. Internal spicules of bone with a “honeycomb” appearance ( arrow in B) are a distinguishing imaging feature. The lesion immediately abuts the cochlea ( arrow in C), possibly contributing to the symptoms of asymmetric sensorineural hearing loss. Mild left facial synkinesis was noted on physical examination. The lesion has remained stable on short-term surveillance imaging.
Intralabyrinthine Schwannomas
Intralabyrinthine schwannomas grow along the most distal branches of the vestibulocochlear nerve and can be found within the cochlea, vestibular, or semicircular canals ( Fig. 4 ). Salzman and colleagues described a classification scheme to accurately document the location of the lesion. Lesions may be difficult to distinguish from enhancement secondary to labyrinthitis; however, correlation with clinical presentation and evolution of symptoms and imaging features may help distinguish the 2.
Intralabyrinthine schwannoma. Axial postcontrast T1-WI ( A ) and axial CISS ( B ) through the IACs demonstrate enhancement within the cochlea and vestibule ( arrows in A), with corresponding filling defects on the heavily T2-weighted sequence ( solid arrows in B) compared with the contralateral side ( dashed arrow in B), compatible with an intralabyrinthine schwannoma. The patient presented with dizziness and vertigo.
Paragangliomas
Paragangliomas are hypervascular neuroendocrine tumors of paraganglia associated with the autonomic nervous system. They represent the second most common neoplasm of the temporal bone and are named for their characteristic locations—the cochlear promontory of the middle ear cavity (tympanic), the jugular bulb (jugular), or contiguously spanning both areas (jugulotympanic paraganglioma).
Tympanic Paragangliomas
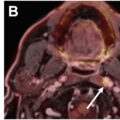
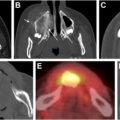
Tympanic paragangliomas, seen as a red retrotympanic mass on otoscopic examination, present as an avidly enhancing mass on the cochlear promontory ( Fig. 5 ). The cochlear promontory is difficult to visualize on MR imaging, however, is located just posterior to the petrous internal carotid artery on axial images. Focal enhancement in this location should prompt further evaluation for a tympanic paraganglioma. The commonly described “salt and pepper” appearance due to T1 hyperintense blood products and hypointense flow voids is often not present in smaller lesions. The lesions typically arise from the inferior tympanic branch of the glossopharyngeal nerve (Jacobson’s nerve), which travels to the cochlear promontory via the inferior tympanic canaliculus. Alternatively, tympanic paragangliomas can arise from the auricular branch of the vagus nerve (Arnold’s nerve).
Tympanic paraganglioma. Axial and coronal noncontrast CT ( A and B ) and postcontrast T1-WI ( C ) demonstrate a lesion centered on the cochlear promontory ( arrow A and B). Postcontrast T1 MR imaging demonstrates abnormal enhancement just posterior to the petrous internal carotid artery ( arrow in C) at the expected location of the middle ear cavity and cochlear promontory. A characteristic red retrotympanic mass was noted on otoscopic examination.
Jugular and Jugulotympanic Paragangliomas
Jugular paragangliomas arise from paraganglia associated with the jugular bulb and can extend superolaterally to involve the middle ear cavity, termed jugulotympanic paragangliomas, and inferiorly can involve the internal jugular vein below the skull base ( Fig. 6 ).
Jugular and jugulotympanic paragangliomas. Axial ( A ) and coronal ( B ) noncontrast CT images demonstrate a lesion centered at the jugular foramen with irregular osseous margins ( arrow in A) and erosion of the jugular tubercle ( arrow in B). Precontrast T1-WI ( C ) demonstrates a characteristic “salt and pepper” appearance due to T1 hyperintense blood products and hypointense flow voids. Postcontrast T1-WI ( D ) demonstrates avid contrast enhancement. Coronal noncontrast CT ( E ) and postcontrast T1-WI ( F ) demonstrate erosive osseous changes and avid enhancement extending from the jugular foramen superolaterally to the middle ear cavity compatible with a jugulotympanic paraganglioma. Time intensity curves from DCE-MR imaging ( G ) demonstrate characteristic lesional rapid wash-in and wash-out of contrast (green curve) similar to the blood pool (white curve from region of interest placed in the contralateral sigmoid sinus).
Paragangliomas of the Facial Nerve Canal
Primary paragangliomas of the facial nerve are extremely rare, but are thought to arise from the branch of Arnold’s nerve traveling in the facial nerve canal ( Fig. 7 ). , Clues to the diagnosis include expansion of the facial nerve canal, particularly the mastoid segment, irregular osseous margins on CT, and avid enhancement with rapid wash-in and wash-out on DCE-MR imaging. ,