This article highlights the diverse upper extremity injuries in Olympic athletes, emphasizing the importance of accurate imaging for diagnosis and management. MR imaging is vital for soft tissue and occult bony injuries, with computed tomography, ultrasound, and radiographs providing complementary rapid assessments. Understanding sport-specific injury patterns and mechanisms enables radiologists to offer targeted insights, enhancing multidisciplinary care. As imaging and sports evolve, these approaches ensure athletes receive optimal care, supporting safe return to competition and peak performance.
Key points
-
•
Upper extremity injuries account for a significant portion of sports-related trauma during the Summer Olympics, particularly affecting athletes in contact and overhead sports such as judo, gymnastics, and swimming.
-
•
Frequent injuries include rotator cuff tears, labral lesions, impingement syndromes, elbow ligament injuries, wrist fractures, and triangular fibrocartilage complex and tendon pathologies.
-
•
Repetitive overhead activity, acute trauma, and high-impact contact are key mechanisms contributing to shoulder, elbow, and wrist injuries in the elite athletes.
-
•
MR imaging is the primary modality for assessing soft tissue and subtle osseous injuries, with aditional roles for ultrasound, computerized tomography, and radiographs in specific scenarios.
-
•
This article highlights characteristic imaging findings, mechanisms, and management considerations across multiple joints injuries, and the radiologists’ key roles for accurate elite athlete assessment.
Abbreviations
| ALPSA | anterior labroligamentous periosteal sleeve avulsion |
| BMX | bicycle motocross |
| DRUJ | distal radioulnar joint |
| ECU | extensor carpi ulnaris |
| MCP | metacarpophalangeal |
| SLAP | superior labrum anteroposterior tear |
| UCL | ulnar collateral ligament |
| US | ultrasound |
| XR | radiographs |
Introduction
Olympic athletes train for their entire lives, especially during the 4-year cycle of the Summer Olympics, preparing for what could be the most important moment of their careers, with events lasting a few seconds to a couple of days. However, despite all the physical and mental training and preparation, injuries can happen during competitions.
Athletic injuries and illnesses at the Olympics have been reported in detail since the 1990s, and based on the Tokyo 2020, Rio de Janeiro 2016 and London 2012 summer Olympics data, approximately 8% to 11% of the Olympics athletes suffered at least 1 injury of bone, ligament, tendon, and/or muscle. The incidence of injury is higher in bicycle motocross (BMX), boxing, taekwondo, rugby, and soccer. ,,
The most common lesions in the upper extremities during the Olympics include fractures, rotator cuff injuries, ligament sprains, and tendinopathies about the elbow and wrist. Muscle strains also seen predominantly affecting the shoulder girdle, however, are less common than in the lower extremities’
Since cross-sectional images have become an important tool in diagnosis, guiding management, and determining prognosis of the injuries, understanding how the most common injuries present and their mechanism, can help athletes and coaches improve their performance and optimize safety in their sports.
The purpose of this article is to review the most common types and mechanisms of musculoskeletal injuries during the summer Olympics games involving the upper extremities and the utility of MR imaging, ultrasound (US), computerized tomography (CT) and radiographs. The central role of the radiologist in team care of the athletes will be emphasized.
Epidemiology
With respect to the last 3 summer Olympics, approximately 11,000 athletes from 200 countries participated in each edition of the Games. In London 2012, a total of 1190 of the athletes sustained at least 1 injury; in Rio de Janeiro 2016, 931 of the athletes suffered at least 1 injury; and in Tokyo 2020, 567 athletes suffered an injury. ,
Shoulder injuries represent a small number of all cases during the Olympics, with most of these injuries related to overuse, instability, and impingement; thus, the throwing athletes are more susceptible to such injuries. For example, in Rio 2016, from 1101 injuries, including both acute and chronic, only 55 were related to shoulder. Patients were from different disciplines such as swimming, judo, boxing, gymnastics, volleyball, and athletics; and the injuries were mostly shoulder dislocations, rotator cuff tendinopathies and tears, and labrum tears.
Elbow injuries during the Olympics are seen mainly in the throwing and power sport athletes. During London 2012, 36 diagnostic studies were performed on elbows, across all imaging modalities. These cases were related to judo, weightlifting, boxing, wrestling, and javelin throw. The ulnar collateral ligament (UCL) was the most commonly seen ligament tear, with additional tendon injuries and muscle strains.
Injuries of the wrist and hand comprised approximately 9% of all sports injuries, including overuse and traumatic lesions. , During Rio 2016, only 25 athletes (2%) underwent an MR imaging for wrist injuries, from sports such as aquatics, tennis, boxing, gymnastics, hockey, and judo. The extensor carpi ulnaris (ECU) tendon was the most injured structure, followed by the triangular fibrocartilage complex (TFCC) and scapholunate ligament. Interestingly, fractures were seen in approximately 32% of the athletes during that Summer Olympics.
Shoulder
The most common sports activities related to shoulder injuries are swimming, tennis, volleyball, gymnastics, and athletics. Most of these injuries occur to repetitive overhead motion and overuse of the joint, leading to microdamage to the muscles, tendons, capsule and labrum, resulting in instability and impingement. Other sports such as rugby, judo, wrestling have similar outcomes; however, in these cases they are usually related to acute trauma. ( Box 1 ).
Box 1
Shoulder injuries in sports
-
Most Common Shoulder Injuries in Sports
-
•
Shoulder impingement
-
•
Rotator cuff tendinopathy and tears
-
•
Subacromial/subdeltoid bursitis
-
•
Labral injuries
-
•
Acromioclavicular dislocation
-
•
Glenohumeral instability
-
•
Shoulder Impingement
Shoulder impingement is a common etiology for athletic injury and is comprised of 2 types.
-
•
External impingement. External impingement happens when the supraspinatus tendon, long head of the biceps and the subacromial bursa are compressed between the humeral head and the coracoacromial arch. Acromial shape and spurs, acromioclavicular joint degenerative changes, fractures or malunion commonly contribute to external impingement. Secondary causes related to capsular and ligamentous laxity may be the result of recurrent stretching of these structures during activity and is most commonly seen in basketball, tennis, and swimming.
-
•
Internal impingement. Internal impingement occurs when the articular surface of the posterior supraspinatus and the anterior infraspinatus tendon fibers are compressed between the humeral head and posterior glenoid, especially on abduction and external rotation during overhead movements.
Rotator Cuff Injuries
The rotator cuff is a complex formed by 4 tendons and their respective muscles, namely the subscapularis, which inserts in the lesser tuberosity, and supraspinatus, infraspinatus and teres minor, which insert in the greater tuberosity.
Partial tears of the rotator cuff can be divided depending on their location in attachment (or footplate), critical zone or myotendinous junction, and additionally in their location with respect to the joint: if the tear is affecting articular sided fibers, bursal sided fibers or interstitial (or intrasubstance). Articular sided partial tears are the most frequent and the prevalence can be up to 60% in patients with rotator cuff injury. On the other hand, bursal-sided partial tears, although less common, reach up to 20% of cases. ,,,, Intrasubstance partial tears are located within the tendon’s substance and are sometimes called concealed lesions , since they cannot be seen during arthroscopy. ,
Full thickness tears of the rotator cuff can be divided into partial width or full width, depending on anteroposterior involvement. Additionally, if there is a full thickness tear involving its full width, it is also known as complete tear. It is important to assess the retraction either seen at the level of the humeral head or glenoid, and such information along with condition of the muscle bellies can help guide surgical management.
In addition, myotendinous injuries can also involve the rotator cuff, presenting usually in the acute setting during sports activities, where the tear occurs proximal to the tendon attachment or critical zone. Such type of injuries can range from strain to partial or complete tears of the myotendinous junction ( Fig. 1 ).
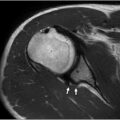
20-year-old female wrestler presenting with sudden shoulder and arm pain during competition. Sagittal T2W fs ( A ), axials T2W fs ( B ). Acute complete avulsion of teres minor tendon from the humeral attachment ( arrow in B ), with associated partial tear of myotendinous junction ( arrows in A ).
Subacromial/Subdeltoid Bursitis
The subacromial/subdeltoid bursa is one of the largest of the human the body and acts to decrease friction between the rotator cuff and overlying bony structures such as acromion, and musculature such as deltoid. Bursal distention can occur due to multiple causes; in the case of the athletes during the Olympics, the most common causes are overuse and in many cases associated with impingement syndrome and rotator cuff tear. The first imaging finding is thickening and mildly increased signal in the bursa on fluid-sensitive MR sequences. Some authors suggest that a bursal thickness of 2 mm or greater can been used as a cutoff to indicate abnormality, though symptomatic bursitis can also be related to edema, fluid distention, and synovial proliferation regardless of the bursal thickness.
Labral Injuries
The glenoid labrum is a fibrocartilaginous structure that attaches as a rim to the articular cartilage of the glenoid fossa and serves to deepen and increase the articulating surface area of the glenoid. MR imaging diagnosis of labral tears is based on abnormalities in the signal intensity, morphology, and location of the labrum. Main imaging findings are surface irregularity, increased signal intensity within the substance of the labrum, fluid or contrast (as seen with MR or CT arthrography) into the substance of the labrum and avulsions.
One of the mechanisms that can lead to a superior labrum anteroposterior tear, also known as SLAP tear, is the one that occurs during the late cocking phase of the throwing. It has been recognized that athletes who engage in repetitive overhead activities, especially swimming, tennis, and volleyball players, develop asymmetries in the ranges of internal and external rotation. Increase in external rotation can be associated with anterior capsule laxity, bony changes in glenoid, and humeral retroversion. As the arm is brought into abduction and external rotation, the biceps take a more vertical and posterior position. This shift in angle produces a posterior vector change as well as a twist at the base of the biceps, which results in increases in torsional force to the labrum, leading to type II SLAP lesions. Of the 4 main types of SLAP tears, type II is the most common and consists of a superior labral tear with possible anterior or posterior extension without tear of adjacent biceps-labral anchor ( Fig. 2 ).
Swimmer with constant shoulder pain during training. Coronal MR arthrogram ( A and B ). Superior labral tear-anterior to posterior ( arrow in A ), extending into the biceps-labral anchor ( arrow in B , SLAP type II). Contrast material is seen extending into the long head of the bicep tendon recess ( arrowhead ).
On the other hand, in contact sports, like wrestling, rugby, judo or BMX, different mechanisms of shoulder injury, especially direct trauma, can lead to anterior shoulder instability (dislocation), acromioclavicular sprain or fracture, muscle/tendon strain or severe fractures or dislocations such as those involving the sternoclavicular joint ( Fig. 3 ) and ribs.
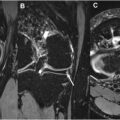
Chest CT with contrast ( A ) with 3-D volume rendered reconstruction ( B ). Sternoclavicular posterior dislocation in a rugby player due to direct trauma during match. The head of the left clavicle is displaced posteriorly ( arrow ), compressing the innominate vein ( arrowhead ).
Acromioclavicular Joint
Acromioclavicular fracture or dislocation is one of the most common injuries in contact sports, and occur from a direct blow to the top of the shoulder or via indirect injury such as a fall on an outstretched arm. This results in stretching and failure of the acromioclavicular ligaments, coracoclavicular ligament, and trapezius muscle insertion, in addition to bone injury at the margins of the joint. Rockwood has classified the acromioclavicular separation into 5 types.
-
•
Type I: sprain of the acromioclavicular ligaments, but the coracoclavicular ligaments are not involved.
-
•
Type II: rupture of the acromioclavicular ligaments. The coracoclavicular ligament is sprained, resulting in edema. Continuity of the coracoclavicular ligament fibers is maintained.
-
•
Type III: complete acromioclavicular joint dislocation, with acromioclavicular and coracoclavicular ligaments completely torn. The deltoid and/or trapezius muscles may present some degree of detachment from the distal clavicle.
-
•
Type IV: the distal end of the clavicle is posteriorly dislocated as the scapula is driven anterior inferiorly.
-
•
Type V: is an exaggeration of the type III injury. The trapezius and deltoid muscle attachments on the clavicle and acromion are completely detached.
-
•
Type VI: is a rare injury caused by a different mechanism. The injury is thought to be due to a severe direct force on the superior surface of the distal clavicle with abduction of the humerus and retraction of the scapular at the same time. As a result, the lateral end of the clavicle rests inferiorly to the acromion or coracoid process.
Less frequently, the acromion and scapula can present stress-related injuries due to overuse or osteochondrosis, such as in golfers or swimmers.
Glenohumeral Joint
Most shoulder dislocations occur anteriorly (95% of the cases) and can lead to chronic instability due to capsule-labral compromise during forced abduction, external rotation, and extension movements. This can occur especially if one of the main shoulder stabilizers, the inferior glenohumeral ligament is injured, triggering chronic instability.
Bankart lesions are the most common labral injury in such events. The classic Bankart lesions are characterized by anteroinferior labral injuries or detachment (soft tissue-Bankart), and can be associated with glenoid rim fracture (bony-Bankart). They are commonly seen in association with Hill-Sachs lesions, the classic posterolateral superior humeral head impaction fracture. Perthes lesion is a variant of the Bankart, in which the anterior inferior labrum is torn and lifted from the edge of the glenoid but still attached to the intact sleeve of periosteum lifted from the anterior aspect of the glenoid ( Fig. 4 ).
Perthes lesion in a gymnast. MR arthrogram in the axial plane, showing a torn anteroinferior labrum ( arrow ), attached to the intact lifted periosteum ( arrowhead ).
Anterior labroligamentous periosteal sleeve avulsion (ALPSA) refers to when the labrum is avulsed from the glenoid and the periosteum remains intact but is displaced medially. Another variant includes the glenolabral articular disruption lesion (GLAD), which involves a tear of the anterior inferior labrum with an associated glenoid chondral defect ( Fig. 5 ).
GLAD lesion in a handball player. MR arthrogram in axial T- weighted fat suppressed (T1W fs), shows a large cartilage defect ( arrow ) in the anterior labrum with associated tear of the anteroinferior labrum ( arrowhead ). A displaced cartilage fragment is seen in the anterior joint recess (star).
Another important injury to be aware of is the inferior capsuloligamentous complex injury with humeral avulsion of the inferior glenohumeral ligament. The most common variant involves avulsion of the anterior band of the inferior glenohumeral ligament from the humeral attachment ( Fig. 6 ).
Track and field athlete with severe shoulder pain after a fall during competition. Coronal MR arthrogram shows complete avulsion of the inferior glenohumeral ligament from the humeral attachment ( arrow ), known as J sign, with associated large joint effusion and extensive pericapsular contrast material in the axillary recess ( arrowhead ).
Approximately 2% to 5% of reported glenohumeral dislocations are posterior. Multiple mechanisms have been described in posterior shoulder dislocation; however, the most common is the axial loading of the arm while adducted, flexed, and internally rotated. Conversely, traumatic posterior dislocations are commonly associated with a characteristic compression deformity of the anteromedial humeral head, known as reverse Hill-Sachs lesion. Other associated lesions include reverse Bankart lesions or posterior labrocapsular periosteal sleeve avulsion, analogous to soft-tissue Bankart and ALPSA lesions seen in anterior dislocations, respectively. ,
Elbow
The most common elbow injuries in sports-related activities, particularly during the Summer Olympics, are UCL injuries, flexor-pronator tendon injuries, lateral and medial epicondylitis, and less frequently, osseous injuries such as stress fractures and dislocations ( Box 2 ).
Box 2
Elbow injuries in sports
-
Most Common Elbow Injuries in Sports
-
•
Stress and traumatic fractures
-
•
Elbow dislocations and complex ligamentous tears
-
•
Ulnar collateral ligament injuries
-
•
Medial and lateral epicondylitis
-
•
Osseous Injuries and Elbow Dislocations
Osseous injuries include stress reactions and fractures of the distal humerus, olecranon, and radial head, particularly in athletes exposed to repetitive loading, such as gymnasts and throwers. These are best visualized on MR imaging as bone marrow edema, cortical irregularity, or fracture lines, and on radiographs as cortical disruption or periosteal reaction in more advanced cases.
Acute traumatic injuries such as elbow dislocations and associated ligamentous or capsular injuries are also encountered, with MR imaging providing detailed assessment of soft tissue disruption and radiographs identifying joint incongruity or associated fractures. The American College of Radiology recommends MR imaging as the preferred modality for evaluating suspected ligamentous, tendinous, or occult osseous injuries when radiographs are normal or indeterminate.
Overall, MR imaging is the primary imaging tool for detailed assessment of soft tissue and subtle bony injuries in elbow dislocations, facilitating accurate diagnosis and management. , The most affected structures are the UCL, often accompanied by radial collateral ligament and lateral ulnar collateral ligament ( Fig. 7 ).
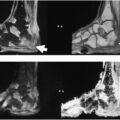
Postreduction MR imaging assessment of posterior elbow dislocation in a volleyball player. Coronal ( A and B ) and sagittal ( C ) T2W fs images. Complete tear of the lateral collateral ligamentous complex ( arrow in A ) and adjacent common extensor tendon ( arrowhead in A ), ulnar collateral ligament ( arrow in B ) with partial tear of the common flexor tendon ( arrowhead in B ). Sagittal sequences show bone bruises of the anterior aspect of the radial head and posterior capitellum (stars in C ). In addition, extensive pericapsular and muscle edema, with joint effusion is also seen.
Ulnar Collateral Ligament
UCL injuries are especially prevalent in sports involving overhead throwing or valgus stress, such as javelin, baseball, and gymnastics, but also occur in weightlifting and judo. On MR imaging, UCL injuries typically present as increased signal intensity, partial or complete discontinuity, and periligamentous edema.
Baseball pitchers, cricket bowlers, and javelin throwers should be aware that the most common pattern of UCL injury involves partial tears of the anterior bundle, the primary restraint to valgus stress during throwing. These tears are often located proximally at the humeral attachment. , The most common MR imaging findings are high T2 signal and fiber disruption in the anterior bundle, edema, and fluid tracking along the ligament, also known as T-sign ( Fig. 8 ), and bone marrow edema or stress reaction in the medial epicondyle in chronic cases.
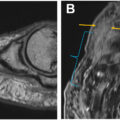
MR arthrogram in Coronal T1Wfs. Figure ( A ) shows normal contrast filling the medial recess of sublime tubercle, contained by the ulnar collateral ligament ( arrow in A ). Figure ( B ) shows contrast extending distally between the UCL and the sublime tubercle ( arrowhead in B , T-sign ), indicating partial tear of the distal UCL.
Flexor-Pronator Tendon Injuries and Overuse Syndromes
Repetitive stress can lead to elbow injuries. Conditions such as medial epicondylitis ( golfer’s elbow ) or lateral epicondylitis ( tennis elbow ) are common. Lateral epicondylitis or common extensor tendinopathy and medial epicondylitis or common flexor tendinopathy are characterized by tendinosis and partial tearing at their respective epicondylar origins, with MR imaging showing increased T2 signal and tendon thickening ( Fig. 9 ). ,,
Lateral epicondylitis in a tennis player. Coronal T2W fs ( A ) and axial T2W fs ( B ) show tendinopathy and a high-grade partial tear at the attachment of the common extensor tendon ( arrows ).
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 High-Resolution Imaging of Knee Meniscus Anatomy and Tears
High-Resolution Imaging of Knee Meniscus Anatomy and Tears
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


