Enhancing masses within SB mesentery and bowel wall
Bull’s-eye or “target” lesions; intussusception
• Lung and breast carcinoma metastases
Are scirrhous tumors
Likely to cause luminal obstruction
• Intraperitoneal metastatic spread (e.g., from ovarian and GI primary tumors)
Serosal metastases cause clustered adhesion and fixation of SB loops and functional obstruction
• Direct invasion (e.g., from pancreatic or GYN tumor)
Lumen of affected SB is often narrowed or obstructed
• Intestinal lymphoma
• Circumferential type: Sausage-shaped mass(es)
Rarely obstructs; may cause aneurysmal dilation
• Polypoid form: Bull’s-eye or “target” lesions
• Mesenteric form: SB masses and nodes
• CT enterography is best protocol, with multiplanar reformation
TOP DIFFERENTIAL DIAGNOSES
• Primary small bowel carcinoma
Solitary mass causing luminal obstruction
• Infectious and inflammatory etiologies
Mucosal hyperenhancement and submucosal edema
CLINICAL ISSUES
• Metastases: Most common with melanoma > lung, breast, others
SB and mesentery are common sites of metastases from melanoma
May arise many years after primary tumor removal
• Lymphoma accounts for 1/2 of all malignant SB tumors
Patients with immune suppression (e.g., transplant recipients, AIDS); celiac disease
• Treatment
Surgical resection of lesions that bleed, perforate, obstruct, or have aneurysmal dilation
(Left) Axial CECT in a 58-year-old man who presented with a known history of malignant melanoma demonstrates 1 of several soft tissue masses in the mesentery. The metastases subsequently resulted in an intussusception.
(Right) Axial CECT in the same patient 5 months later reveals the resultant long-segment intussusception . One of the bowel wall metastases served as the lead point of the intussusception.
(Left) Axial CECT in a 46-year-old man who presented with a known history of non-Hodgkin lymphoma demonstrates extensive, multifocal, bowel wall thickening and aneurysmal dilatation of the lumen of the ileum .
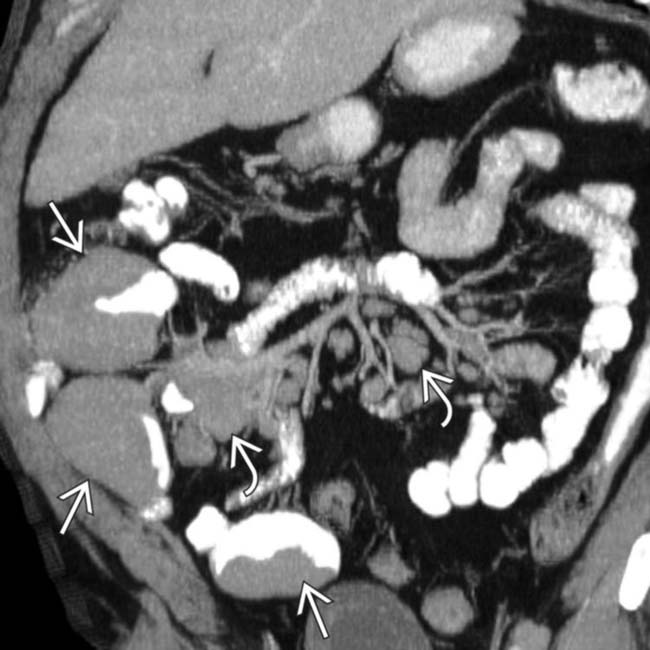
(Right) Coronal CECT reconstruction in the same patient illustrates extensive mesenteric lymphadenopathy and encasement of the mesenteric vessels, but no bowel or vascular obstruction. Multifocal masses of lymphoma are also seen.
TERMINOLOGY
Definitions
• Intestinal metastases from extraintestinal primary cancer
• Lymphoma: Malignant tumor of B lymphocytes
Primary small bowel (SB) lymphoma: Limited to bowel ± mesenteric nodes
Secondary or generalized lymphoma: Involvement of spleen, liver, or thoracic nodes















 in the mesentery. The metastases subsequently resulted in an intussusception.
in the mesentery. The metastases subsequently resulted in an intussusception.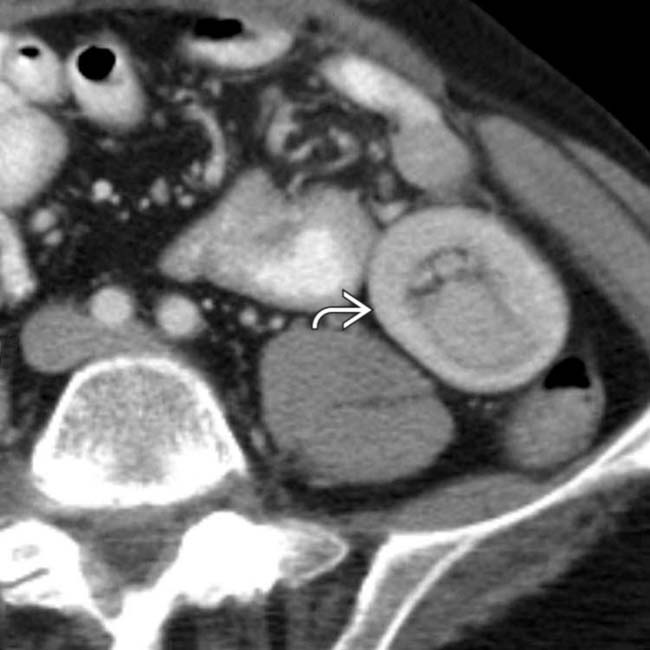
 . One of the bowel wall metastases served as the lead point of the intussusception.
. One of the bowel wall metastases served as the lead point of the intussusception.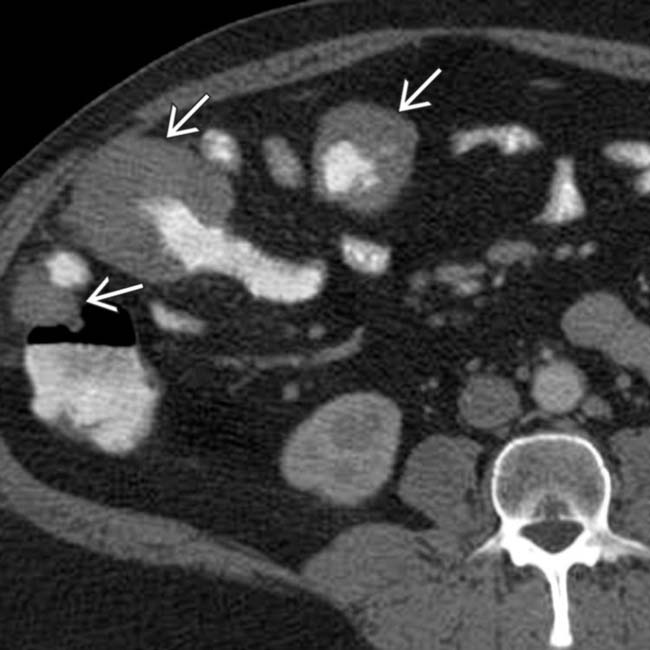
 .
.
 and encasement of the mesenteric vessels, but no bowel or vascular obstruction. Multifocal masses of lymphoma
and encasement of the mesenteric vessels, but no bowel or vascular obstruction. Multifocal masses of lymphoma  are also seen.
are also seen.



 Most detailed study of SB is enteroclysis (tube administration of barium into SB with distention of lumen)
Most detailed study of SB is enteroclysis (tube administration of barium into SB with distention of lumen)











 Endoexoenteric (cavitary form): Localized perforation into extraluminal tissue
Endoexoenteric (cavitary form): Localized perforation into extraluminal tissue












