Intracranial Vascular Malformations and Aneurysms
Nicholas A. Telischak
Huy M. Do
Since the last edition of this chapter, magnetic resonance imaging (MRI) has firmly established itself in depiction of lesions of the cerebral vasculature. In addition to now routine standard techniques, many new sequences are pushing the envelope such that physiologic information such as cerebral blood flow is easily acquired noninvasively. It is well established that MRI is the most specific and sensitive noninvasive modality for the detection of intracranial vascular malformations of all types, whether angiographically demonstrable or angiographically occult. Even the detection of subarachnoid hemorrhage (SAH), for which computed tomography (CT) was previously felt to be superior (1), has been shown to be equally or better depicted by MRI (2,3). MR is widely held to be more sensitive to the documentation of the sequelae of vascular lesions and complications of their treatment than CT. As a general rule, MR has replaced CT as the screening modality of choice for intracranial vascular malformations and their complications in all clinical settings, although CT will still prove useful when artifact plagues MRI or when a patient has a contraindication to MRI.
In certain clinical settings and pathologies, it has even become apparent that the complete preoperative assessment of some types of vascular malformations (generally those without arterial or high-flow components), as well as all secondarily related intracerebral pathology, can be made with MR alone. The continued refinement and development of high-field (3 Tesla [T] and beyond) MR scanners, newer pulse sequences, such as diffusion tensor imaging (DTI) and arterial spin labeling (ASL), and improvements to MR angiography (MRA) promise even more sensitive and sophisticated methods for detecting and specifically defining these lesions based on anatomic and pathophysiologic criteria and temporal evolution. Functional MR (fMRI) (see Chapter 33) techniques are no longer nascent and are well suited to the regional mapping of brain functions in the presence of vascular malformations that occupy “eloquent” cortex (4). The role of fMRI in the study of vascular malformations, for both preoperative mapping and more detailed investigations of anomalous development of cortical representations in the presence of congenital space-occupying lesions like arteriovenous malformations (AVMs), has been better elucidated as the techniques have matured.
Although MR has become part of the standard workup of patients suspected (or known) to harbor vascular lesions, catheter angiography continues to be the definitive imaging modality and is still the mainstay of diagnosis in the preoperative and postoperative evaluations of AVMs and aneurysms. Multidetector CT angiography (CTA) has had a significant effect on the imaging of aneurysms, but for vascular malformations, especially AVMs, CTA lacks the temporal resolution accurately to depict these lesions (5). Concurrent with the improvements in MR have been dramatic improvements in CTA, such that both modalities are now complimentary. It should be emphasized that despite all of the improvements in these techniques, intracranial aneurysms in particular still cannot be definitively excluded by any noninvasive modality, including CTA, leaving conventional intra-arterial catheter angiography as the gold standard for aneurysm diagnosis. Three-dimensional (3D) rotational angiography has improved the diagnostic quality and safety of intracranial diagnostic and endovascular treatment procedures for both AVM and aneurysm diagnosis and therapy. The 3D rotational angiography images are obtained by reconstruction of a series of images that are acquired while the C-arm rotates in a continuous movement around the region of interest. Computer-automated reconstruction algorithms then enable the physician to view vascular morphology in any direction, including cut-planes and “flythrough” modes (6,7,8,9,10). The 3D digital subtraction angiography (DSA) and rotational C-arm CT images are now obtainable in nearly all rotational angiography units and are indispensable in the neurovascular setting (11,12).
Vascular Malformations
Vascular malformations of the brain have been classified by McCormick (13) and Russell and Rubinstein (14) into four major pathologic types: AVM, cavernous malformation, capillary telangiectasia, and developmental venous anomaly (DVA). The basis for these classifications is that each entity has its distinct pathologic abnormalities. In addition, each has its unique clinical presentation, treatment, and, in most cases, MR characteristics. Although not typical, clinical imaging studies and necropsy specimens have demonstrated that mixed vascular malformations having pathologic characteristics of two or more of the major types may also occur (15,16,17,18,19).
Aside from these congenital (developmental) lesions, a distinct entity is the dural arteriovenous fistula (DAVF). The DAVF represents an acquired vascular lesion, characterized by arteriovenous (AV) shunting involving vessels within the dural venous sinuses and coverings of the brain. Estimates of the overall incidence of vascular malformations involving the brain range from 0.1% to 4%.
Arteriovenous Malformations
The most common clinically symptomatic cerebrovascular malformation is the AVM. AVMs have an estimated incidence of
about one-seventh that of intracranial aneurysms (20), which corresponds to approximately 0.14% of the population. AVMs represent congenital anomalies of blood vessel development and result from preservation of direct communication between arterial and venous channels without an intervening capillary network (21).
about one-seventh that of intracranial aneurysms (20), which corresponds to approximately 0.14% of the population. AVMs represent congenital anomalies of blood vessel development and result from preservation of direct communication between arterial and venous channels without an intervening capillary network (21).
 FIGURE 11.1 Arteriovenous malformation, artist’s depiction. Tangle of vascular nidus receives supply from multiple enlarged tortuous arteries. Markedly enlarged proximal draining veins carry arterialized blood. |
The focus of all therapy involving any surgical or catheter treatment in the management of a patient harboring an AVM is the tangle of abnormal vessels representing the site of this primitive communication—the nidus—which replaces the normal arterioles and capillaries with a low-resistance, high-flow vascular bed (Fig. 11.1). The nidus permits increased flow through the arterial feeding vessels to the AVM and delivers increased blood volume under relatively high pressure into the cerebral venous system. Therefore, it is of paramount importance in pretherapy imaging to delineate this vascular nidus in those patients for whom intervention is planned.
Clinical Features
Although they are congenital, AVMs most commonly are not clinically apparent until the second through the fourth decades of life, with most having become symptomatic by the time the patient reaches age 40 years (22). In adults, the most common initial symptom is related to acute intracranial hemorrhage, although larger AVMs are more likely to present with seizures rather than acute hemorrhage (23). Seizures and progressive neurologic deficits follow hemorrhage in frequency, and other, less common clinical manifestations may also occur. In those cases in which the AVM becomes apparent in the pediatric age group, hemorrhage is more likely than seizures to be the initial clinical event (24).
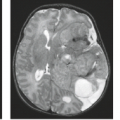
From historical literature, intracranial hemorrhage heralds the existence of the AVM in 30% to 55% of patients and most often occurs during the second or third decade (25,26,27,28). More than 70% of patients who become symptomatic due to acute intracranial hemorrhage do so before age 40 years. Intracranial hemorrhage associated with AVMs is most often intraparenchymal, with the presumed site of bleeding being the nidus or proximal arterialized venous drainage. Intraventricular hemorrhage and SAH may also occur, although AVMs represent the etiology of only some nontraumatic SAHs. On the other hand, the occurrence of nontraumatic isolated intraventricular hemorrhage (i.e., without SAH) in an adult should always suggest the presence of an underlying AVM (Fig. 11.2).
The rate of bleeding from AVMs has received much attention in the clinical literature for decades, and the appropriate management of unruptured AVMs has now become newly controversial. It was generally believed that the incidence of bleeding from cerebral AVMs was much lower than that of intracranial (saccular) aneurysms. Over the past couple of decades, data, however, had suggested a high rate of hemorrhage, in the range of 2% to 4% per year. It had become conventional wisdom that the rate of hemorrhage from an AVM is at least as high as (28) and probably exceeds that of aneurysmal hemorrhage from long-term follow-up studies (26,27). Data suggest that AVMs in deep gray matter have a higher bleed rate than those in other cerebral locations (29). Estimates of annual bleed rates have ranged from 0.9% per year for patients without hemorrhagic AVM presentation, deep location, or deep venous drainage to 34.4% per year in patients having all three risk factors (30).
In 2014, a randomized study (the ARUBA trial) of adults with nonruptured AVMs was published comparing medical
management to interventional plus medical management in 223 patients from 39 sites in 9 countries (31). The ARUBA trial showed that medical management alone is superior to medical management with interventional therapy for the prevention of death or stroke in patients with unruptured brain AVMs followed up for 33 months. The randomized study was halted due to the superior outcome in the medical management alone group. The trial specifically showed a more than threefold increased risk of stroke and death after the initiation of interventional therapy compared with medical management alone in these patients. At the time of this writing, the continued funding of a longer-term study was denied, partly based on the disparity in outcome events between the two treatment arms in the trial. Statisticians calculated a range of 12 to 30 years might be needed for events in the medical arm to reach that of the intervention group, assuming no further events occur in the intervention group. As J.P. Mohr wrote in May 2015, “the current status of the data from ARUBA leaves unsettled both the long-term rate of hemorrhage and hemorrhage severity for those in the medical arm,” but concluded “In adult patients (>18 years) with an unruptured AVM, addition of interventional therapy (ie, neurosurgery, embolization, or stereotactic radiotherapy, alone or in combination) to medical management alone (ie, pharmacologic therapy for neurologic symptoms as needed) is probably harmful” (32).
management to interventional plus medical management in 223 patients from 39 sites in 9 countries (31). The ARUBA trial showed that medical management alone is superior to medical management with interventional therapy for the prevention of death or stroke in patients with unruptured brain AVMs followed up for 33 months. The randomized study was halted due to the superior outcome in the medical management alone group. The trial specifically showed a more than threefold increased risk of stroke and death after the initiation of interventional therapy compared with medical management alone in these patients. At the time of this writing, the continued funding of a longer-term study was denied, partly based on the disparity in outcome events between the two treatment arms in the trial. Statisticians calculated a range of 12 to 30 years might be needed for events in the medical arm to reach that of the intervention group, assuming no further events occur in the intervention group. As J.P. Mohr wrote in May 2015, “the current status of the data from ARUBA leaves unsettled both the long-term rate of hemorrhage and hemorrhage severity for those in the medical arm,” but concluded “In adult patients (>18 years) with an unruptured AVM, addition of interventional therapy (ie, neurosurgery, embolization, or stereotactic radiotherapy, alone or in combination) to medical management alone (ie, pharmacologic therapy for neurologic symptoms as needed) is probably harmful” (32).
 FIGURE 11.2 Isolated intraventricular hemorrhage on sagittal (A) and axial images (B–D) was due to proven arteriovenous malformation. |
From the literature prior to the ARUBA study, each occurrence of hemorrhage from an AVM is associated with a mortality of 10% to 15%, with an overall annual mortality rate in the range of 1%. In addition, permanent neurologic deficit associated with hemorrhage has been estimated to be approximately twice the risk of death, that is, 20% to 30% per episode of hemorrhage, for an annual incidence in the vicinity of 2%. The risk of rebleeding after the initial hemorrhage from cerebral AVM has been estimated to be 6% during the first year (33). After the first year, the rebleeding rate decreases to that of the rate of initial hemorrhage in patients with symptomatic AVMs who had no clinical history of bleeding, estimated to be 2% to 4% per year (20,25). In the analysis of the ARUBA study for patients followed up without interventional therapy, the data demonstrated a low spontaneous rupture rate of 2.2% per year (95% CI, 0.9% to 4.5%). In the past, no significant increase in the risk of AVM hemorrhage was considered to be associated with hypertension or specific situations, such as physical activity, pain, or trauma (20,25,34). However, others have found that hypertension is positively associated with hemorrhage in patients harboring intracranial AVMs (35).
The dominant single predictor of future AVM hemorrhage is initial hemorrhagic presentation; that is, if a patient originally presents with hemorrhage, they are at higher risk of repeat hemorrhage than a patient with an identical-appearing, unruptured AVM. Several anatomic and physiologic factors are associated with increased hemorrhage from an AVM: exclusively deep venous drainage, periventricular/intraventricular or basal ganglia location of the AVM, arterial supply from perforating vessels or from the vertebrobasilar system, intranidal aneurysm(s), and high intranidal pressure, which is reflected by high pressures in the feeding arteries or restriction of venous outflow (36,37,38,39). In a recent large, individual patient data meta-analysis of three large AVM databases, identified risk factors for hemorrhage included hemorrhagic presentation (hazard ratio 3.86), increasing age (hazard ratio 1.34 per decade), female sex (hazard ratio 1.49), and exclusively deep venous drainage (hazard ratio 1.60) (40). The ARUBA study secondary analyses argue against a predictive spontaneous hemorrhage effect from the Spetzler–Martin AVM grade, however. Although investigators have reported that smaller AVMs (less than 2.5 cm) present more frequently with hemorrhage than larger ones, the absolute effects of small size may be overestimated. Smaller malformations may be less likely to cause other symptoms such as seizures, headaches, and steal phenomena than are larger AVMs and therefore are more likely to present with bleeding (41). A high incidence of underlying AVM has been reported by many investigators in patients presenting with intracranial hemorrhage after cocaine abuse (42,43), and so the diagnosis must be aggressively pursued in that specific clinical setting.
Seizures are also a common clinical manifestation of intracranial AVMs, reported as an initial symptom in 20% to 60% of cases in several large series (20,23,33,44). More often associated with AVMs situated in the temporal and frontal regions, seizures affect more than half of AVM patients younger than 30 years.
Acute or progressive neurologic deficits may result from the presence of an intracranial AVM. Although acute neurologic deficits have been reported to accompany 90% of AVM-associated intraparenchymal hemorrhages, neurologic deficits may arise in the absence of bleeding. In fact, the risk of significant morbidity and mortality is high in AVMs, whether or not the lesion has ruptured. Crawford et al. (26) followed 217 patients who had conservative management of their AVMs for a mean period of more than 10 years. They estimated that aside from the risk of hemorrhage, the risk of seizure disorder was 18% and the risk of neurologic dysfunction was 27% during the 20-year follow-up in conservatively treated patients. In the study by Anderson et al. (45), there was a 25% risk of a patient becoming disabled because of intellectual impairment, even without hemorrhage.
Progressive and transient deficits have been ascribed to a number of potential pathophysiologic mechanisms. Among those proposed is “steal” of blood flow from adjacent normal regions of brain into the low-resistance, high-flow vessels feeding the AVM. Dilation of arterial supply to the AVM or enlarged draining veins may result in mass effect with resultant compression and neurologic dysfunction. Hydrocephalus may develop, either as a result of prior hemorrhage or by compression of adjacent cerebrospinal fluid (CSF) pathways. Venous hypertension represents an additional cause of neurologic dysfunction that may affect brain adjacent to or at a distance from the AVM nidus.
Headache is another frequently described clinical manifestation of intracranial AVMs; it affects more than half of patients at some time during their clinical course (46). Although no characteristic headache pattern is consistently observed in AVM patients, a number of authors have reported atypical migraine-like pain with associated visual complaints. The incidence of true migraine, however, appears no higher in patients with AVMs than in the general population. AVMs with arterial supply from dural arteries may cause headache as a result of involvement of the pain-sensitive dura. Other mechanisms of pain include increased intracranial pressure, hemorrhage, hydrocephalus, and mass effect.
Additional clinical associations of AVMs include subjective bruit, which was noted in nearly 30% of patients in one series (25). Objective cranial bruit is an infrequent finding in adult patients with AVMs. Compression of cranial nerves is a rare symptom, most often reflected by atypical facial pain from involvement of cranial nerve V. Hemifacial spasm and glossopharyngeal neuralgia due to involvement of the seventh and ninth nerves have also been described (46).
Pathologic Findings
Although AVMs can be found throughout the central nervous system, intracranial AVMs are located in the supratentorial compartment in approximately 80% to 93% of cases. Supratentorial AVMs usually arise over the convexities and involve the distribution of the middle cerebral artery (MCA), typically visible over the surface of the cerebral hemisphere. However, deep-seated lesions are not uncommon. When AVMs are situated within deep structures, their venous drainage typically
enlarges the deep venous system; in children, this may result in a massive enlargement of the vein of Galen (“vein of Galen aneurysm”), which should not be confused with a vein of Galen malformation, a misnomer that describes an AV fistula occurring in infants and children resulting in an enlarged draining median vein of the prosencephalon. AVMs are most often solitary lesions, but they can be multiple when part of certain syndromes (47), including hereditary hemorrhagic telangiectasia (Rendu–Osler–Weber disease) and mesencephalon-oculor facial angiomatosis (Wyburn–Mason syndrome).
enlarges the deep venous system; in children, this may result in a massive enlargement of the vein of Galen (“vein of Galen aneurysm”), which should not be confused with a vein of Galen malformation, a misnomer that describes an AV fistula occurring in infants and children resulting in an enlarged draining median vein of the prosencephalon. AVMs are most often solitary lesions, but they can be multiple when part of certain syndromes (47), including hereditary hemorrhagic telangiectasia (Rendu–Osler–Weber disease) and mesencephalon-oculor facial angiomatosis (Wyburn–Mason syndrome).
 FIGURE 11.3 Arteriovenous malformation, intraoperative photograph. Note the well-circumscribed arteriovenous malformation with vessels of varying caliber and states of thrombosis. (Courtesy of Dr. E. Flamm, Philadelphia, PA.) |
On direct inspection, the gross pathologic appearance of an AVM is a tangled cluster of irregularly dilated vessels with varying wall thicknesses and luminal sizes (Fig. 11.3). Classically, AVMs appear as wedge-shaped clusters of vessels, with the apex of the wedge directed toward the ventricular surface and the base located at the cortical margin. Intervening brain parenchyma is not found within the vascular nidus itself, but feeding and draining vessels are separated by parenchyma when examining the malformation in its entirety (48).
Typically, neither displacement nor mass effect on adjacent structures is present unless hemorrhage has occurred or there has been development of large venous varices involved in the drainage of the lesion. With time, feeding arteries of the AVM gradually enlarge with increased flow, and venous drainage pathways undergo progressive dilation and tortuosity. Approximately 10% of AVMs have associated arterial aneurysms, most of which occur on arteries hemodynamically related to the lesion (49,50). In one recent series, more than 98% of aneurysms originated from arteries hemodynamically or anatomically related to the AVM (50).
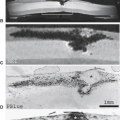
On histopathologic examination, arterial channels in AVMs usually show well-defined elastic laminae, a feature absent in the venous channels. Wall thickening of both arterial and venous channels is often present with hyperplasia of smooth muscle cells, fibroblasts, and connective tissue. In many cases, focal areas of wall thinning may be found, representing sites of possible hemorrhage. Regions of thrombosis and recanalization are often present. Intervening and adjacent brain parenchyma frequently exhibit degenerative changes, seen as mild or extensive gliosis and demyelination (Fig. 11.4), often with concomitant parenchymal atrophy (48,51). Evidence of prior hemorrhage is also frequently present, as evidenced by ferritin, hemosiderin, and other iron-storage forms (Fig. 11.5). Calcification may involve not only vessel walls, but also adjacent brain parenchyma due to chronic ischemia or old hemorrhage (Fig. 11.4).
Pretreatment Grading of Arteriovenous Malformations
Grading systems have been developed in an effort to rank individual AVMs into groups predictive of the difficulty associated with a specific treatment and the probable response to that treatment. Ideally, such a system should be sufficiently simple for easy application yet comprehensive enough to permit grading of all AVMs. It should, therefore, encompass all features of the lesion that influence risks of the specific treatment modality and accurately predict the degree of risk associated with the treatment. Although such an ideal grading system does not exist, a number of systems have been proposed.
Surgical grading scales are based on clinical, anatomic, and/or physiologic characteristics of the AVM and the patient. Features studied have included the age and sex of the patient, the presence of neurologic deficits, and the occurrence of prior hemorrhage. The number and location of feeding arteries, site and size of the AVM nidus, and pattern of venous drainage have also been included in various grading systems (52,53,54,55,56).
A relatively simple and widely used AVM grading system (although not widely used in diagnostic neuroradiology reports) is that proposed by Spetzler and Martin (55). This system assigns a numerical grade to the AVM, with higher grades indicating lesions that are more surgically difficult. It requires
evaluation of three features: the size of the nidus, the location of the nidus, and the venous drainage pattern. The nidus size is scored as small (less than 3 cm), medium (3 to 6 cm), or large (greater than 6 cm), with 1, 2, or 3 points given, respectively. Venous drainage is categorized as either superficial (score of 0) if drainage is entirely into the cortical venous system or deep (score of 1) if any or all drainage enters the deep system. The location of the nidus is determined to be within either “eloquent” (score of 1) or “noneloquent” (score of 0) regions of brain, where eloquent areas are those with readily identifiable neurologic function and resultant disabling neurologic deficit when injured (Table 11.1). By this definition, eloquent areas include sensorimotor, visual, or language cortex; internal capsule; thalamus; hypothalamus; brainstem; cerebellar peduncles; and deep cerebellar nuclei (Table 11.2).
evaluation of three features: the size of the nidus, the location of the nidus, and the venous drainage pattern. The nidus size is scored as small (less than 3 cm), medium (3 to 6 cm), or large (greater than 6 cm), with 1, 2, or 3 points given, respectively. Venous drainage is categorized as either superficial (score of 0) if drainage is entirely into the cortical venous system or deep (score of 1) if any or all drainage enters the deep system. The location of the nidus is determined to be within either “eloquent” (score of 1) or “noneloquent” (score of 0) regions of brain, where eloquent areas are those with readily identifiable neurologic function and resultant disabling neurologic deficit when injured (Table 11.1). By this definition, eloquent areas include sensorimotor, visual, or language cortex; internal capsule; thalamus; hypothalamus; brainstem; cerebellar peduncles; and deep cerebellar nuclei (Table 11.2).
 FIGURE 11.4 Right hemispheric arteriovenous malformation, computed tomography (CT) versus magnetic resonance (MR) versus digital subtraction angiography (DSA). A: CT before contrast administration. B,C: CT after contrast administration. D: T1-weighted postcontrast MR. E,F: T2-weighted MR. G–I: Three-dimensional time-of-flight MR angiography. J,K: Anteroposterior (AP) and lateral DSA arterial phase. L,M: AP and lateral DSA venous phase. CT before contrast (A) shows a relative hyperdense mass with punctate and curvilinear calcifications with surrounding edema and mass effect. There is dense enhancement of the anterior round tubular component representing the draining venous aneurysm and mottled spongiform enhancement of the posteriorly located nidus after contrast administration (B,C). On MR, prominent flow void (E,F) and pulsation artifact along the phase-encoding axis (D, arrows) denote the arteriovenous malformation and venous varix. Note the surrounding high signal intensity on T2-weighted images (E,F) representing gliosis in adjacent brain. Three-dimensional time-of-flight MR angiography (G–I) demonstrates right middle cerebral arterial feeders, nidus, and large tortuous draining vein of Trolard (arrows) but fails to demonstrate the huge proximal draining venous aneurysm confirmed on angiography (L,M, curved arrows) due to slow flow and intravoxel phase dispersion. |
 FIGURE 11.5 Arteriovenous malformation (AVM), evidence of prior hemorrhage by magnetic resonance. Axial T2-weighted (A) and gradient-recalled echo (GRE) (B) images show a region of mixed signal on T2 that appears to be hemorrhagic on GRE in the left basal ganglia. The abnormality was confirmed to be an AVM with deep venous drainage at angiography (C). |
TABLE 11.1 Spetzler–Martin Determination of Arteriovenous Malformation (AVM) Grade | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The numerical score from these features is added to give the overall grade of the AVM. For instance, a grade I lesion would be small, located in noneloquent cortex, and have only superficial venous drainage. A grade V AVM would be large, involve eloquent cortex, and have deep drainage. In this system, large or diffuse AVMs encompassing the entirety of critical structures are classified as grade VI because surgical resection of such lesions would be associated with unavoidable disabling neurologic deficit or death.
Therapy
Because AVMs have been thought to hold a grim prognosis if left untreated, the goal of management (in the appropriate clinical setting) has been complete obliteration of the nidus for cure.
Various therapeutic arms are available for patients with intracranial AVMs, including surgery, intravascular embolotherapy, and radiotherapy, often used in some combined approach. Traditional treatment for AVMs has been surgical excision of the nidus. Complete surgical excision can be achieved in approximately 80% of AVMs with mortality and morbidity better than that arising from the natural history of the lesion if left untreated. Combined operative morbidity and mortality rates equal approximately 10% when taking into account all AVMs, regardless of grade (28). With the ARUBA study, however, the treatment of unruptured AVMs is now newly controversial.
Various therapeutic arms are available for patients with intracranial AVMs, including surgery, intravascular embolotherapy, and radiotherapy, often used in some combined approach. Traditional treatment for AVMs has been surgical excision of the nidus. Complete surgical excision can be achieved in approximately 80% of AVMs with mortality and morbidity better than that arising from the natural history of the lesion if left untreated. Combined operative morbidity and mortality rates equal approximately 10% when taking into account all AVMs, regardless of grade (28). With the ARUBA study, however, the treatment of unruptured AVMs is now newly controversial.
TABLE 11.2 “Eloquent” Areas of Braina | ||||||
|---|---|---|---|---|---|---|
|
Most postoperative morbidity in the series by Heros and Korosue (28) occurred in very large AVMs, AVMs that were immediately adjacent to critical anatomy, and AVMs with deep venous drainage (i.e., those that would be classified as Spetzler grade V). If one only considered AVMs of grades I through IV, morbidity and mortality were only 4.5% in the series by Heros and Korosue. To evaluate the proposed Spetzler–Martin grading system, Hamilton and Spetzler (57) prospectively studied 120 patients with brain AVMs who underwent surgery and showed no permanent deficits in grade I, II, and III patients. For grade IV and V patients, permanent neurologic deficits were found in 21.9% and 16.7%, respectively. This AVM grading system accurately correlated with both new temporary (p < 0.0001) and new permanent (p = 0.008) neurologic deficits. Thus, this evaluation confirms the accuracy and utility of this grading system for assisting with management decision-making. Because the rates of immediate rebleeding and mortality and morbidity associated with hemorrhage from AVMs are lower than those associated with aneurysmal hemorrhage, acute or emergent surgical intervention is limited to patients with life-threatening intracranial hemorrhage. Timing of surgery is determined by the characteristics of the lesion and the judgment of the surgeon. Depending on the risk associated with surgical treatment alone, adjunctive or alternative forms of therapy may be used.
Radiosurgery or stereotactic external beam radiation therapy uses focused irradiation directed at the AVM nidus. Radiosurgery is usually pursued in those cases considered unsuitable for resection because of either location of the AVM nidus or overall operative risk. Generally, the size of the nidus must be less than 3.5 cm for the AVM to be considered suitable for treatment by these methods. Radiotherapy techniques cause obliteration of the nidus secondary to radiation damage to vessel endothelium (58), with minimal radiation exposure of the surrounding brain parenchyma. A single dose is used that is larger than the typical fractionated doses used to treat brain tumors. Obliteration rates in the range of 75% to 90% have been reported with permanent neurologic complications (due to radiation necrosis) in the range of 3% to 10% (59,60,61,62). Significant controversy over the role of radiotherapy for AVMs continues, however, as some studies have questioned the efficacy of any form of radiotherapy based on worse reported outcomes from radiotherapy than from microsurgery in some hands (63). Among the advantages of radiotherapy are its relatively noninvasive nature (for some radiosurgical systems stereotactic frames need to be placed on the patient’s skull while others utilize a thermoplastic mask) and its absence of visible effects on the head. Unlike microneurosurgical resection, the effect of radiosurgery takes months to years. Therefore, the risk of hemorrhage is still present until the lesion entirely disappears (64).
Endovascular treatment is usually an adjunctive measure to either surgery or radiation. Complete endovascular obliteration of brain AVMs occurs in only approximately 5% of cases and in general occurs in AVMs that are small and with one or two arterial feeders (65,66,67). Embolization usually precedes surgery or radiosurgery. Surgery most frequently benefits from embolization when deep feeding vessels are eliminated. Reduction in the AVM nidus size decreases venous outflow, which can be helpful, especially when the venous drainage is deep. The goal of preradiosurgical embolization is to reduce the size of the radiosurgical target (AVM nidus) to 3.0 cm or less in all dimensions. The efficiency of AVM obliteration is low when the AVM nidus exceeds 3.0 cm when treated with γ radiation (“gamma knife”) or x-ray photon radiation (“LINAC radiosurgery”). Large AVMs greater than 3.0 cm may benefit from stereotactic heavy–charged-particle Bragg peak radiation (68). Aneurysms associated with AVMs are at risk for rupture before, during, and immediately after the treatment of the AVMs. New aneurysms may arise in patients with high-flow AVMs. The risk of intracranial hemorrhage from either source is higher in female patients. To reduce the complications of intracranial hemorrhage in these patients, these aneurysms should be treated by either surgical or endovascular means before administering definitive therapy for the AVMs (69).
Magnetic Resonance Imaging
Complete imaging evaluation of an AVM requires the acquisition of sufficient information on which to select, plan, and carry out therapy. Features of the lesion to be evaluated include (a) the number, location, and specific identification of arterial supplies to the AVM (including collateral circulation to the AVM and vascular steal from adjacent normal brain); (b) associated vascular lesions (e.g., aneurysms); (c) the presence of hemorrhage (acute or chronic); (d) the location, size, and flow characteristics of the nidus; (e) venous drainage of both the AVM and the normal brain, including the presence of venous thrombosis, outflow restriction, or mass effect; and (f) follow-up of any prior therapy (55,70).
Although cerebral angiography clearly remains the definitive method of fully characterizing the vascular supply and venous drainage of intracranial AVMs, recent advances with MR allow specific diagnosis of these lesions in most cases. It has been recognized that improved anatomic delineation of the AVM nidus, its relationship to vital cerebral structures, and improved definition of the lesion in 3D space with the use of MR (Fig. 11.6) has contributed significantly to optimizing surgical approach (71) and has allowed treatment of some lesions that previously would have been believed to be inoperable (28).
Associated hemorrhage and other parenchymal changes and posttherapy follow-up are best evaluated with the use of MR in conjunction with supplemental MRA. MR information derived from these types of studies is complementary to the angiographic evaluation and clearly contributes significantly to accurate diagnosis and optimal therapeutic decisions (Figs. 11.5 and 11.6).
The typical AVM on conventional fast spin-echo or spin-echo (SE) MR is depicted as a cluster of focal round, linear, or serpentine areas of signal void (Figs. 11.4–11.7), representing dilated vascular channels containing relatively rapidly flowing blood (72). Although large high-flow AVMs are usually obvious diagnoses on MRI, subtle enlargement of deep veins occasionally may be the only clue to the diagnosis of these high-flow lesions. Note that certain MR sequences can result in high intensity in areas of flowing blood (Fig. 11.6) because of either flow-related enhancement or even echo rephasing (73) or because of the now routine incorporation of gradient moment nulling into SE imaging. High intensity from these phenomena is generally a reflection of slower flow. Gadolinium enhancement of the enlarged vessels also occurs in those vessels with relatively slow flow, that is, mainly the venous side of the lesion. AVM nidi can partially enhance after gadolinium (Figs. 11.8–11.10), but the rapidly flowing blood within arterial feeding vessels generally does not enhance. Despite the traditional teaching stating that intraparenchymal AVMs demonstrate little or no mass effect on imaging studies unless hemorrhage has occurred, enlargement of draining veins can result in fairly significant mass effect (Fig. 11.10), even in the absence of hemorrhage, in up to one-third of cases (25).
 FIGURE 11.6 Arteriovenous malformation (AVM), complete anatomic delineation by magnetic resonance. Right internal carotid angiogram in anteroposterior (A) and lateral (B) projections demonstrate two AVMs in the right thalamic region fed by hypertrophied lenticulostriate arteries and a smaller AVM in the right orbit fed by small branches from the ophthalmic artery. The precise location of the thalamic AVM is well depicted by axial T1-weighted (C,D), T2-weighted (E), and three-dimensional time-of-flight magnetic resonance angiography (F,G). The enlarged deep draining basal vein of Rosenthal is well seen. Both AVMs are also well depicted on multidetector computed tomography angiography with coronal (H,I) and sagittal (J) reformations. |
 FIGURE 11.7 Extensive holohemispheric racemose arteriovenous malformation with dilated feeding arteries and enlarged cortical venous drainage (A,B) is associated with chronic parenchymal changes, including atrophy of the corpus callosum. Note the enlarged leptomeningeal vessels well seen after gadolinium (C), as well as markedly feeding arteries outlined on magnetic resonance angiography (D). |
 FIGURE 11.8 Spetzler–Martin grade III arteriovenous malformation (AVM) in a 14-year-old girl with severe headache and altered mental status. Sagittal T1-weighted image demonstrates frontotemporal acute hemorrhage with mass effect (A). Coronal T2-weighted image shows dark acute blood products in the left temporal lobe. MIP image of the MRA does not show clear vascularity, obscured by blood products (C). Ferraheme blood pool T1-weighted image shows clear abnormal vascularity along the medial border of the hemorrhage (D). 3D reconstructions of the Ferraheme contrast-enhanced T1 images show the venous drainage patter into the basal vein of Rosenthal and straight sinus (E,F). AP and lateral views of the catheter angiogram in the early arterial (G,H) and late arterial phase (I,J) show the supply to the AVM from branches of the left anterior choroidal artery and from a lateral lenticulostriate artery with venous drainage into the left basal vein of Rosenthal. |
 FIGURE 11.9 Deep thalamic arteriovenous malformation with deep venous drainage (A,B) shows heterogeneous enhancement limited to slower-flowing components (C); magnetic resonance angiography shows vascular relationships to the lesion (D). |
 FIGURE 11.10 A 17-year-old female with headache, found to have a Spetzler–Martin grade IV arteriovenous malformation with mass effect in the absence of hemorrhage. T1-weighted sagittal (A) and T2-weighted axial (B) MRI show flow voids from a right parieto-occipital AVM. T1-weighted postcontrast image shows minimal enhancement (C). There is evidence of blood products on the axial GRE sequence (D). ASL demonstrates arteriovenous shunting into an enlarged cortical vein. MIP image from the MRA shows the arterial supply. Note the presence of mass effect on the occipital horn of the right lateral ventricle in the absence of hemorrhage. In a 21-year-old female with a left parietal Spetzler–Martin grade IV arteriovenous malformation as identified on sagittal T1-weighted (A), axial T2-weighted (B), sagittal FLAIR image (C), axial GRE images (D). ASL image shows increased cerebral blood flow and early venous shunting. Axial and sagittal postcontrast BRAVO images (L,H), and MRA (G) delineate the arterial supply and draining veins. |
Aside from the features of the intracranial AVM itself, associated findings on MR may provide further insight into the natural history of these lesions and aid in predicting the development of secondary clinical deficits in individual patients. The presence and age of any associated intraparenchymal hemorrhage (Figs. 11.8 and 11.11) and its resultant mass effects are clearly seen on MR. Associated intraparenchymal hemorrhage can be aged on the basis of signal intensity patterns (see Chapter 13). Staining of adjacent brain by iron-storage products can suggest prior subclinical hemorrhage from a clinically asymptomatic AVM. Intraventricular or superficial cortical hemosiderosis from prior (or recurrent) SAHs is a frequent accompaniment to vascular malformations. This entity, not usually seen on CT, is often an incidental MR finding, but patients can develop cranial nerve palsies, most commonly sensorineural hearing loss, or extraventricular obstructive hydrocephalus. Long–repetition
time/echo time (TR/TE) (T2-weighted) SE and gradient-recalled echo (GRE) images demonstrate marked hypointensity along the surface of the brain parenchyma or along the ependymal surface of the ventricle in this entity (Fig. 11.12) (74). Venous occlusive disease, probably an important pathophysiologic feature of many AVMs, should be sought on MR. This can be suggested by massively dilated vessels (nearly always representing veins) of either the deep or superficial venous system. Enlargement of the medullary veins, even in the contralateral hemisphere from the site of the AVM, is an important clue to venous occlusive disease (particularly in dural AV fistulas; see Dural Arteriovenous Fistulas). Signal intensity alterations representing gliosis
and/or secondary demyelination in the vicinity of the AVM are easily demonstrated and imply chronic vascular ischemia, perhaps because of steal from adjacent brain.
time/echo time (TR/TE) (T2-weighted) SE and gradient-recalled echo (GRE) images demonstrate marked hypointensity along the surface of the brain parenchyma or along the ependymal surface of the ventricle in this entity (Fig. 11.12) (74). Venous occlusive disease, probably an important pathophysiologic feature of many AVMs, should be sought on MR. This can be suggested by massively dilated vessels (nearly always representing veins) of either the deep or superficial venous system. Enlargement of the medullary veins, even in the contralateral hemisphere from the site of the AVM, is an important clue to venous occlusive disease (particularly in dural AV fistulas; see Dural Arteriovenous Fistulas). Signal intensity alterations representing gliosis
and/or secondary demyelination in the vicinity of the AVM are easily demonstrated and imply chronic vascular ischemia, perhaps because of steal from adjacent brain.
 FIGURE 11.11 A 23-year-old male with acute left temporal lobe hemorrhage from a Spetzler–Martin grade I AVM as shown on T1-weighted (A) and T2-weighted (B) images. Sagittal contrast-enhanced T1-weighted BRAVO image shows abnormal vascularity along the base of the hematoma (C), and there is increased CBF with shunting on the ASL image (D). MRA fails to show abnormal vascularity adjacent to the hematoma (E), which was evident on the lateral projection of the catheter angiogram with arterial supply from temporal branches of the left MCA and venous drainage to an infratemporal vein to the left lateral sinus (F). |
 FIGURE 11.12 Intraventricular arteriovenous malformation with intraventricular siderosis. A: T1-weighted magnetic resonance (MR) (600/20). B: T2-weighted MR (2,800/80). C: Gradient-echo MR (150/15/50 degrees). Right ganglionic and intraventricular arteriovenous malformation is unambiguously depicted as round and serpentine regions of signal void on spin-echo images (A,B) and as high intensity on gradient-echo image (C). Note the marked hypointensity lining the right lateral ventricle (C, arrows), more obvious on the gradient-echo image (C), indicating prior intraventricular hemorrhage. (From Atlas SW, Fram EK, Mark AS, et al. Vascular intracranial lesions: applications of fast scanning. Radiology 1988;169:455–461, with permission.) |
To determine the precise role of MR in the diagnostic workup of intracerebral AVMs, several investigators have studied patients with these lesions and compared MR findings with those of other imaging modalities (71,75,76). MR has been shown to be competitive with both CT and catheter angiography for demonstrating the neuroanatomic location of the nidus and the relationship of its supplying and draining vessels to deep ganglionic structures, the ventricular system (Figs. 11.6 and 11.13), and the corpus callosum (Fig. 11.14 and 11.15).
This information is critical to treatment planning, whether surgical, endovascular, or radiosurgical (72).
This information is critical to treatment planning, whether surgical, endovascular, or radiosurgical (72).
 FIGURE 11.13 Arteriovenous malformation adjacent to hemorrhage in the left lateral ventricle. Axial T2-weighted image shows hemorrhage in the left lateral ventricle (white arrow) with flow voids (white arrow) from the adjacent Spetzler–Martin grade IV arteriovenous malformation (A,B). Blood products in the ventricle and AVM show blooming artifact on axial GRE images (black arrow) (C,D). Axial T1-weighted image before (E) and after (F) gadolinium contrast demonstrates intense hematoma (white arrow) and mild enhancement of the nidus. MRA shows the left frontal AVM with supply from left anterior cerebral artery, middle cerebral artery, and lateral lenticulostriate branches (G,H). Closer inspection of the MRA (A) and T2-weighted axial images identifies a perinidal aneurysm as the cause of hemorrhage (arrows), confirmed on the AP view of the catheter angiogram (arrow, K) and on a selective injection of the lateral lenticulostriate artery (arrow, L). This was treated with targeted embolization with n-BCA (native image, M), with exclusion of the aneurysm on the postembolization angiogram (N). |
 FIGURE 11.14 Arteriovenous malformation involving the corpus callosum. T1-weighted sagittal (A) and T2-weighted axial (B) images demonstrate serpentine signal voids within the genu and anterior body of the corpus callosum, which adjacent to the nidus shows thinning. After administration of gadolinium, partial enhancement of the nidus occurs (C). MRA in the lateral projection demonstrates the callosal AVM with supply from numerous small branches of the paricallosal artery. Early drainage into the deep venous system is into the inferior sagittal sinus and an ectatic ependymal vein draining to the vein of galen. AP and lateral projections of the catheter angiogram better define the arterial supply, nidus, and draining veins (E,F). |
 FIGURE 11.15 A 36-year-old man with a corpus callosum arteriovenous malformation that extends into the left lateral ventricle. A: Axial T2-weighted (2,900/87.5/2) image through the level of the nidus with setup acquisition block for lateral projection magnetic resonance (MR) digital subtraction angiography (DSA). B: T2-weighted image shows the nidus extending into the left lateral ventricle. C: Left carotid selective conventional catheter angiogram shows the arteriovenous malformation. D–F: Several stages of MR DSA during passage of a contrast bolus in a lateral projection. Early arterial phase (D), late arterial phase (E), and early venous phase (F). (From Griffiths PD, Hoggard N, Warren DJ, et al. Brain arteriovenous malformations: assessment with dynamic MR digital subtraction angiography. AJNR Am J Neuroradiol 2000;21:1892–1899, with permission.) |
MR and CT allow for accurate representations of lesion volumes, and are often used as an adjunctive study to both MR and angiography for treatment planning purposes, although the gold standard that we use for radiosurgical planning is that of fused 3D rotational angiograms (Figs. 11.16 and 11.17). The size of the AVM nidus is important for many reasons, including an overall increase in operative grade (and risk) with increasing nidus size and the potential for normal perfusion pressure breakthrough after a large nidus is resected (77). The potential for hemorrhage is also related to AVM size: smaller AVMs tend to present more often with hemorrhage than larger AVMs, perhaps because by definition they are less likely to cause symptoms related to mass effect (78). MR is also superior to CT for demonstrating the degree of nidus obliteration after intra-arterial embolization. In such cases, MR often allows clear depiction of the thrombosed portion of the lesion and accurate differentiation of patent from thrombosed vessels, a distinction that even conventional arteriography may not make with certainty because of the many physiologic changes in flow after endovascular therapy (71). MR is more sensitive than either CT or angiography at delineating hemorrhagic complications of AVMs, especially those that are subacute or chronic (Figs. 11.5 and 11.8).
Conventional catheter angiography remains superior to MR in depicting the specific arterial supply and venous drainage of the AVM. Even thin-section, high-resolution MR can only implicate abnormal veins or arteries in an AVM on the basis of enlargement, a feature that may not be present in all involved vessels. Similarly, 3D time-of-flight (TOF) MRA is a nonselective technique that cannot define with certainty the specific feeding arteries and draining veins, although approaches to selective time-resolved MRA or MR DSA techniques have been developed (Fig. 11.16) (see Chapter 28). These time-resolved techniques include both noncontrast ASL sequences (79), and bolus tracking sequences with gadolinium. Even newer contrast agents such as ultrasmall superparamagnetic iron oxide particles (USPIO) (e.g., Ferraheme) may further improve what MR can show (80). Currently, the spatial and temporal resolution of these sequences still cannot match a catheter directed DSA. Moreover, one must detect and characterize aneurysms that are associated with the AVM because certain types are reported to have an extremely high risk of rupture (81). Obliteration of symptomatic intranidal or perinidal aneurysms is now considered a part of the surgical or endovascular management of AVMs (50,69), and so these lesions must be defined on imaging studies (Figs. 11.13, 11.17–11.19). If MRA is performed in these patients, then the region of interest is not limited to the AVM itself and must include the circle of Willis and feeding arteries into the nidus.
Differential Diagnosis
Because AVMs are frequently associated with intracranial hemorrhage, the question of the diagnosis is often raised when the patient presents after an episode of intracranial hemorrhage. In the presence of any intracerebral hematoma, the radiologist must search for evidence of large vessels to suggest AVM, which can be detected with either CT or MR (Fig. 11.20). It is important to realize that the failure to identify large vessels on MR in the presence of an acute hematoma does not entirely exclude an AVM as the cause of the hemorrhage (Fig. 11.21). Small AVMs
occasionally can be angiographically occult because of a variety of factors, including compression of the lesion by adjacent hematoma, vasospasm, extremely slow flow, and thrombosis. These lesions are often referred to as “cryptic” AVMs.
occasionally can be angiographically occult because of a variety of factors, including compression of the lesion by adjacent hematoma, vasospasm, extremely slow flow, and thrombosis. These lesions are often referred to as “cryptic” AVMs.
 FIGURE 11.16 Right frontal AVM in a 22-year-old man. Main arterial feeder from the anterior cerebral artery (arrows), medium nidus (arrowheads), and superficial drainage. (A) Time-resolved SL MR angiographic images over two cardiac cycles in axial (top), sagittal (middle), and coronal (bottom) planes: two short early-draining veins are located on the superior portion of the nidus, posteromedial (white arrows) and anterolateral (black arrows), and then converge into a single vein toward the superior sagittal sinus; there was no artifact, although the anterior cerebral artery is close to the nasal fossa and ethmoid sinus. (B) TOF MR angiography in axial (top) and sagittal (bottom) planes does not allow venous drainage analysis. (C) Time-resolved CE MR angiography in axial (top) and sagittal (bottom) planes. Nidus delineation is less accurate than at time-resolved SL MR angiography over two cardiac cycles; complete venous drainage is better detected, with an anastomotic vein toward the right lateral sinus (gray arrows), but the two short early-filling draining veins are not distinguished. (D) Reference DSA in sagittal (top) planes and in comparison with time-resolved SL MR angiography over two cardiac cycle (bottom) planes. The two short early-filling draining veins are distinguishable with DSA. (From Raoult H, Bannier E, Robert B, et al. Time-resolved spin-labeled MR angiography for the depiction of cerebral arteriovenous malformations: a comparison of techniques. Radiology 2014;271(2):524–533.) |
 FIGURE 11.17 Radiosurgical planning for residual AVM. AP native image (A) demonstrates a large Onyx cast within the patient’s left cerebellar AVM, with a lateral DSA image (B) showing residual arteriovenous shunting through remnant AVM nidus. Images from the 3D rotation angiogram show the embolization material cast and the residual nidus, which were subsequently used to create a radiosurgical treatment volume (C,D). |
 FIGURE 11.18 Flow-related aneurysms. Sagittal T1-weighted image (A), axial GRE (B), postcontrast axial T1-weighted (C), and axial T2-weighted images show a large Spetzler–Martin grade IV right frontoparietal arteriovenous malformation with increased cerebral blood flow on the ASL image (E) and rapid T-max on bolus perfusion imaging (F). MRA identifies multiply dysplastic aneurysms of the feeding anterior cerebral arteries and anterior communicating artery, confirmed on the lateral projection catheter angiogram (I) and reformatted 3D rotational angiogram (J). |
 FIGURE 11.19 Acute arteriovenous malformation (AVM) hemorrhage from an intranidal aneurysm in a 38-year-old woman with sudden severe headache and mental status change. Noncontrast computed tomography (A) and T1-weighted (B) and gradient-recalled echo (C) images demonstrate casting of the lateral and third ventricle by blood products. Sagittal reformatted image (D) from computed tomography angiography shows a vascular lesion in the quadrigeminal plate region suspicious for a small AVM with a possible nidal aneurysm, which was confirmed at angiography (E,F) from lateral left vertebral injection. This small AVM was supplied by a branch of the medial posterior choroidal artery, which was superselectively embolized, resulting in cure (G,H). |
 FIGURE 11.20 Ruptured intranidal aneurysm. A,B: Sagittal and coronal T1-weighted magnetic resonance (MR). C–E: Axial T2-weighted MR. F,G: Computed tomography angiogram (CTA). H,I: Anteroposterior and lateral right internal carotid artery angiogram. Subacute parenchymal hematoma (arrows) is seen inferior and anterior to the arteriovenous malformation nidus (A–E). Note the prominent flow voids in the enlarged central draining veins on T2-weighted sequence (C,D). Sagittal maximum intensity projection image from CTA (F) is suspicious for an aneurysm arising from a feeding right middle cerebral artery branch in the same location as the hematoma (white arrow). Variceal draining cortical and galenic system veins are well depicted on three-dimensional reformatted CTA (G, black arrows). At angiography (H,I), which was done for confirmation and stereotactic presurgical localization, the aneurysm is again demonstrated (arrows). The aneurysm was surgically clipped and was found to be the cause of the bleed. |
 FIGURE 11.21 Hyperacute hematoma with cryptic arteriovenous malformation (AVM). A: Sagittal T1-weighted magnetic resonance (MR) (600/11). B: Axial T2-weighted MR (3,000/80). C: Lateral view, arterial phase, angiogram. D: Anteroposterior view, arterial phase, angiogram. Parietal mass (A,B,1) represents hyperacute hematoma (see Chapter 9), with no definite evidence of AVM on MR. Arteriogram shows posterior parietal AVM with small nidus (C,D, closed arrows) and draining vein (D, open arrows). |
A major part of the role of the radiologist once the identification of an intracerebral hemorrhage has been made on MR is the search for any associated enlarged vessels because the diagnosis of an underlying AVM is of paramount importance in these cases. A point of confusion may arise when a cavernous hemangioma is identified but vascular channels are noted in contiguity with the lesion (Fig. 11.22). The keys to the diagnosis of the “mixed malformation,” composed of cavernous hemangioma plus venous angioma (discussed later in this chapter), are the recognition of two features of the associated vessels: the characteristic “spoke-wheel” morphology of the enlarged vessels and the very slow flow through these vessels (shown by either SE intensities or with gadolinium enhancement) (Figs. 11.23 and 11.24).
Occasionally, a hypervascular neoplasm with markedly enlarged vessels manifests as an acute hematoma. The only potential source of confusion with AVM might be a hemangioblastoma, which can certainly be associated with markedly enlarged vascular channels and intraparenchymal hematoma. The typical macrocystic component and the identification of the enhancing mural nodule of hemangioblastoma separate this entity from AVM in most cases. Moreover, hemangioblastomas do not generally bleed.
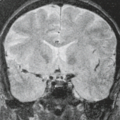
Although the diagnosis of AVM is usually unambiguous on MR, one other lesion can superficially masquerade as an AVM because it too is depicted as abnormally dilated vascular channels. Moyamoya disease is characterized by the occurrence of progressive symmetric occlusion involving the bifurcations of the internal carotid arteries (ICAs) and the proximal anterior and middle cerebral arteries. The occlusive process stimulates the development of an extensive network of enlarged basal, transcortical, and transdural collateral vessels. The angiographic appearance of the innumerable tiny collateral vessels, termed “puff of smoke” or “moyamoya” in Japanese, gives the condition its name.
Moyamoya disease has a bimodal age presentation, with the first peak occurring in the first decade of life, associated with cerebral infarction as progressive carotid occlusion develops. Adult patients most often present in the fourth decade with intracranial hemorrhage arising from the rupture of the delicate network of collateral vessels. Hemorrhage from moyamoya is intraparenchymal in 60% of cases, with intraventricular hemorrhage accounting for nearly all the rest (82,83). Occasionally, isolated SAH is the initial manifestation of the disease.
 FIGURE 11.22 Hemorrhage involving dorsal medulla cannot be dismissed as cavernous malformation due to subtle vessels in adjacent subarachnoid space, later proven as arteriovenous malformation. |
 FIGURE 11.23 Incidentally discovered developmental venous anomaly with arteriovenous shunting. Axial T2-weighted (A) and gradient-recalled echo (GRE) images (B) show numerous linear small channels oriented perpendicularly to the cortical surface which show minimal intrinsic hyperintensity on the axial T1-weighted image likely secondary to slow flow (C) and enhance on the postcontrast T1-weighted axial image (D). An unusual finding in this case is the presence of arteriovenous shunting on the arterial spin labeling (ASL) image which signifies a transitional type of developmental venous anomaly. In a second patient with a left occipital developmental venous anomaly shown on an axial T1-weighted contrast-enhanced image (F), there is ASL signal abnormality with early shunting into the superior sagittal sinus (G). |
Characteristically, flow voids representing large collaterals and the markedly enlarged striate vessels are seen on MR amid the deep ganglionic structures (84,85). Absence of the expected flow void within the cavernous and supraclinoid portions of the ICAs is a consequence of narrowing and ultimately occlusion of these vessels. Changes resulting from ischemia or rupture of the fragile, enlarged network of collateral vessels, including regions of infarction or hemorrhage, may also be seen (Fig. 11.25). This diagnosis is clearly defined by MR when evidence of the occlusive disease of the distal ICAs is apparent in conjunction with the flow voids representing the enlarged striate vessels. Associated enhancing leptomeningeal collaterals after gadolinium and hyperintensity within these surface collaterals and small arterial branches on FLAIR images should suggest this diagnosis.
 FIGURE 11.24 Hemorrhagic mixed malformation in a middle-aged woman who presented with mild headache. Noncontrast computed tomography (CT) (A) shows no acute findings, only a region of calcification in the right cerebellum. She presented several months later with sudden acute loss of consciousness. Repeat head CT (B) and T1-weighted (C), T2-weighted (D,E), gradient-recalled echo (F,G), and T1 postcontrast (H) magnetic resonance (MR) studies show a large acute left cerebellar hematoma with upward transtentorial herniation. MRI demonstrates multiple smaller chronic-appearing bleeds consistent with multiple cavernous malformations. Enhanced MR sequence suggests a linear enhancement in the right cerebellum, which was confirmed to be a developmental venous anomaly at angiography (I). |
 FIGURE 11.25 Young woman with bilateral moyamoya disease. Hyperintense slow-flow leptomeningeal collaterals with right hemispheric deep chronic infarctions on fluid-attenuated inversion recovery (A) were verified as patent collaterals after gadolinium (B). Arterial spin labeling (ASL) images performed before (C), and after the administration of diamox (D) show worse cerebral perfusion to the left hemisphere at baseline. Poor perfusion to the right frontal lobe at baseline shows augmentation of cerebral blood flow following diamox administration. Right internal carotid artery (ICA) catheter angiogram shows classic findings of moyamoya disease, including occlusion of the supraclinoid segment of the ICA and innumerable leptomeningeal collateral vessels (E,F). |
 FIGURE 11.26 Computed tomography (A) shows subtle hyperdensity in the right parietal region without mass effect. Fluid-attenuated inversion recovery (FLAIR) (B) and T2 (C) demonstrate abnormal right parietal white matter; especially note the hyperintense subarachnoid space on FLAIR. After gadolinium, characteristic leptomeningeal enhancement and enhancing intrachoroidal vascular malformation (D) prove a diagnosis of Sturge–Weber syndrome. |
Most often, the underlying occlusive process is idiopathic and is more commonly seen in Asian patients. An identical picture may result from progressive distal internal carotid occlusion arising from any other etiology that is accompanied by collateral development, termed moyamoya syndrome. Such causes include neurofibromatosis and sickle cell disease and as a delayed effect of radiation therapy to the suprasellar region. An increased incidence of moyamoya changes may also be present in patients with Down syndrome. Another entity associated with marked enhancement of surface vessels that should not be confusing is Sturge–Weber syndrome (Figs. 11.26 and 11.27). On close inspection, the MR changes associated with moyamoya are usually quite characteristic and should not be confused with the findings of an AVM or any other entity.
Posttherapy MR
In addition to the initial pretreatment evaluation of the patient harboring an intracranial AVM, MR has gained increasing importance in the assessment of these patients after treatment has been completed. Several investigators have studied the effects of radiosurgery on intraparenchymal AVMs based on imaging (86,87,88). Expected pathologic changes after therapy include deposition of collagen within the subendothelial space of the nidus, resulting in gradual narrowing and thrombosis of the lesion. A significant reduction in nidus size after therapy is usually clearly recognized on MR, even without MRA. This is depicted as a decrease in previously recognizable flow void with increased signal intensity on T2-weighted images and persistent contrast enhancement in the area of the nidus. Significant evidence of reductions in AVM flow generally does not occur until at least 12 months after the initial treatment (Fig. 11.28) (89). It should be noted that CT is inaccurate in evaluating residual AVM nidus size after radiosurgery because persistent contrast enhancement is demonstrated even after complete obliteration.
Complications of this treatment may also be monitored by MR. Changes in the surrounding parenchyma have been noted as early as 3 months after treatment and include transient vasogenic edema and radiation necrosis. Most often, asymptomatic vasogenic edema is a frequent finding in these patients and is characterized by hyperintensity on T2-weighted images in white matter surrounding the nidus. Symptomatic radiation necrosis occurs in an estimated 3% to 4% of patients and is seen as high intensity with mass effect and irregular enhancement (Fig. 11.29). Hemorrhage can be concomitant with radiation necrosis.
In an in vitro study, liquid cyanoacrylate mixtures used for superselective endovascular embolization of AVMs demonstrated signal characteristics similar to fat secondary to the iophendylate component that is added to make the mixture more radiopaque. After the addition of blood to simulate in vivo postembolization and polymerization conditions, the signal characteristics of clotted blood predominated (90). MRI of patients after staged transarterial flow-directed embolization with N-butyl cyanoacrylate demonstrated the region of the “glue” cast as mixed regions of alternating high and low signals on conventional images (Figs. 11.30–11.32).
 FIGURE 11.27 Atrophy in the right parietal lobe, calvarial thickening, and right lateral ventricle choroid plexus mass on T2 and fluid-attenuated inversion recovery (A,B) are accompanied by parenchymal hypointensity on T2* gradient-echo images (C), making the diagnosis of unsuspected Sturge–Weber syndrome obvious. Confirmation was achieved on gadolinium-enhanced sagittal and axial images (D). |
 FIGURE 11.28 Arteriovenous malformation (AVM) pre- and postcyberknife radiosurgery in a 7-year-old girl who presented with right-sided weakness. Anteroposterior left internal carotid artery angiogram (A) shows a large but compact AVM nidus in the right thalamus fed by multiple lateral lenticulostriate arteries. Pretreatment fluid-attenuated inversion recovery (B) and three-dimensional time-of-flight magnetic resonance angiography (C) show a discrete nidus in the thalamus. Repeat magnetic resonance (D,E) done 1 year after radiosurgery demonstrates obliteration of previously seen prominent flow voids and flow-related enhancement consistent with a favorable response to treatment. |
 FIGURE 11.29 Arteriovenous malformation with extensive radiation necrosis after treatment. A: Pretherapy magnetic resonance (MR). A supraventricular arteriovenous malformation is clearly seen as signal voids in this patient without neurologic deficit. B,C: Posttherapy MR. Severe edema (B) with marked contrast enhancement (C) indicates extensive radiation necrosis in the patient, who developed hemiparesis. |
 FIGURE 11.30 Postembolization magnetic resonance (MR). The N-butyl cyanoacrylate “glue” cast is hyperdense on computed tomography (A), predominantly isointense on T1-weighted MR (B), and of mixed signal intensity on T2-weighted MR (C, arrows). |
 FIGURE 11.31 Vein of Galen malformation. Infant with pulmonary hypertension and enlarging head circumference. Sagittal T1-weighted (A), axial T2-weighted (B,D), and arterial spin-labeled (C) (ASL) MR images show numerous small choroidal branches supplying a choroidal type vein of Galen malformation draining into an enlarged median vein of the prosencephalon (black arrow, A), with clear evidence of rapid arteriovenous shunting on the ASL image (white arrow, C). Following multiple sessions of n-BCA embolization, a glue cast can be clearly seen in the venous pouch on sagittal T1-weighted (A), coronal T2-weighted (B), axial T2-weighted (C), and axial gradient-recalled echo (GRE) MR images. |
 FIGURE 11.32 Arteriovenous malformation with adjacent hematoma, magnetic resonance (MR) versus time-of-flight MR angiography. Sagittal T1-weighted (700/12) (A) and axial T2-weighted (2,300/80) (B) images demonstrate intraparenchymal hemorrhage with adjacent areas of signal void. Three-dimensional time-of-flight MR angiography (C) shows feeding vessels originating from the left posterior cerebral artery and their relationship to the area of high-signal hematoma. Lateral (D) and anteroposterior (E) vertebral artery injections show the arterial supply, nidus, and superficially draining vein. |
Specialized MR Techniques in Arteriovenous Malformations
MR Angiography
Since the initial publication by Wedeen et al. (91) showing intravascular flow as high signal intensity on in vivo MR images, intense scientific and clinical interest has focused on imaging the cerebral vasculature and its pathology with MR. The various methods of imaging vascular flow and displaying it in multiple projections have been termed “MR angiography” because of the similar appearance of these images to conventional catheter angiography using iodinated contrast agents and x-rays. MRA for the brain and spine consists of three principal techniques of data acquisition: TOF, phase contrast (PC), and contrast-enhanced TOF (92,93,94,95,96,97,98).
The major impetus for the development of MRA as a potential replacement for catheter angiography in the diagnosis of neurologic diseases is the morbidity and mortality of cerebral catheter angiography. The historical literature reports that aside from local complications due at the puncture site itself, there is approximately a 4% incidence of neurologic event, a 1% fixed neurologic deficit incidence, and a small but definable (less than 0.1%) incidence of death from these procedures (99). It should be recognized, however, that in competent and well-trained hands, cerebral angiography is well documented to be a safe procedure and has become much safer with the improvement in equipment, contrast agents, and techniques (100,101). In fact, in a meta-analysis of the risk of angiography in patients with SAH, cerebral aneurysm, and AVMs, Cloft et al. (102) found that the risk of permanent neurologic complication is only 0.07%, much lower than that found in patients presenting with transient ischemic attacks or ischemic stroke (0.7%; p = 0.004). The second motivation for developing MRA for the workup of neurologic disease, particularly in the United States in the current healthcare climate, is the hospital cost of catheter angiography, a factor that varies widely and is too complex a subject for this review.
More specific characterization of regions of signal void on (fast) SE images as regions of blood flow rather than from dense calcification or hemorrhage can be obtained by using gradient-refocused limited flip-angle techniques (94,103). These techniques form the basis of TOF and PC MRA (see Chapter 16). On these sequences, regions of flowing blood are most often demonstrated as high signal intensity. These techniques can be relatively rapid methods of clarifying ambiguous regions of signal intensity on SE images as flowing blood (such as subependymal vessels or vessels near cortical margins). The presence of major venous sinus occlusion accompanying the AVM can also
be clarified with MRA techniques. It is clear that at least some familiarity of the physics of flow is essential to the appropriate design and implementation of these techniques (104) (see Chapter 32). While not generally thought of as an MRA sequence, blood pool imaging with 3D postcontrast acquisitions (e.g., BRAVO) is excellent at delineating the venous side of the cerebral circulation and can be performed either following gadolinium contrast or USPIO which has a strong T1 shortening effect and yields exquisite images of the blood pool (Fig. 11.8).
be clarified with MRA techniques. It is clear that at least some familiarity of the physics of flow is essential to the appropriate design and implementation of these techniques (104) (see Chapter 32). While not generally thought of as an MRA sequence, blood pool imaging with 3D postcontrast acquisitions (e.g., BRAVO) is excellent at delineating the venous side of the cerebral circulation and can be performed either following gadolinium contrast or USPIO which has a strong T1 shortening effect and yields exquisite images of the blood pool (Fig. 11.8).
The fundamental role for such flow imaging techniques as MRA in the diagnostic workup of the patient with an AVM is controversial at this point in the evolution of these techniques (105). Interesting early results have been reported on the utility of 3D volume-rendered surface anatomy displays of 3D TOF MRA for staging of AVMs (106,107,108). This display technique has been used together with catheter cerebral angiography for the treatment planning and targeting of AVMs for radiosurgery.
Although no one doubts that MRA can demonstrate the vascular nature of a high-flow AVM, the importance of simply showing the tangle of vessels on an image is arguable because the mere identification of the lesion is usually accomplished even with conventional MR. In fact, the AVM can sometimes be even more clearly separated from adjacent hematoma by MR rather than by MRA (Figs. 11.11 and 11.31). MRA in those AVMs that are fed by enlarged dural vessels is a valuable tool because dural feeding arteries are often not seen well on conventional SE MR because of their intrinsic signal void superimposed against the background of signal void of skull base and calvarium. The search for dural vessels involved in AVMs is a clear indication for supplemental MRA rather than MR alone (see Dural Arteriovenous Fistulas).
One could make a strong argument that the assessment of AVM nidus size might be an appropriate indication for MRA of these lesions, whether pretreatment or posttreatment, for several reasons. First, in terms of prognosis, many neurosurgeons classify AVMs at least in part based on nidus size (55,78). Second, it is common practice to evaluate these patients after radiotherapy and/or embolization to determine the residual nidus, particularly if one desires to avoid exposing these patients to invasive catheter angiograms multiple times. Third, most institutions that treat some AVMs with a form of radiotherapy triage these lesions based on the size of the nidus, among other factors, where lesions less than 3.5 cm are more difficult to treat with such therapy (59,60,61,62). MRA does represent a potentially effective way to demonstrate a quantifiable nidus size in 3D space (Fig. 11.32). Reports of the utility of time-resolved projectional MRA and dynamic MR DSA for depiction of intracranial AVM and dural AVM have been encouraging (109,110,111). Recently, a comparative study demonstrated that 3D TOF MRA at 3 T is superior to the same technique at 1.5 T in terms of image quality, detection rates of feeding arteries, and draining veins (112). More important, however, the same study found that both MRA techniques are equal in nidal size evaluation and both are inferior to DSA in all assessment criteria.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


