INTRODUCTION TO WOMEN’S IMAGING (FEMALE PELVIS IMAGING)
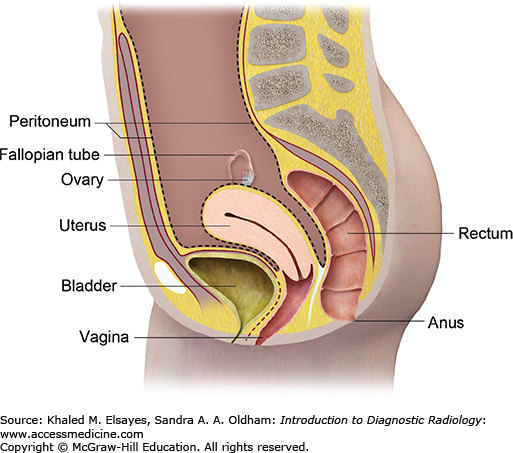
The uterus is a pear-shaped organ located in the female pelvis between the urinary bladder anteriorly and the rectum posteriorly (Figs. 10.1 and 10.2). The average dimensions are approximately 8 cm long, 5 cm across, and 4 cm thick, with an average volume between 80 and 200 mL. The uterus is divided into 3 main parts: the fundus, body, and cervix.
Blood is provided to the uterus by the ovarian and uterine arteries, the latter of which arise from the anterior division of the internal iliac artery. The uterine artery occasionally gives off the vaginal artery (although this is usually a separate branch of the internal iliac artery), which supplies the upper vagina, and the arcuate arteries, which surround the uterus. It then further branches into the radial arteries, which penetrate the myometrium to provide blood to all layers, including the endometrium.
Once these vessels reach the endometrial level, they branch into the basal arteries and spiral arteries, which support the specialized functions of each layer. The basal arteries are not responsive to hormones; they support the basal endometrial layer, which provides the proliferative cells for endometrial growth. The spiral arteries supply the functionalis layer and are uniquely sensitive to steroid hormones. In ovulatory cycles in which pregnancy does not occur, menses results following constriction of these terminal arteries, causing endometrial breakdown with desquamation of the glands and stroma.
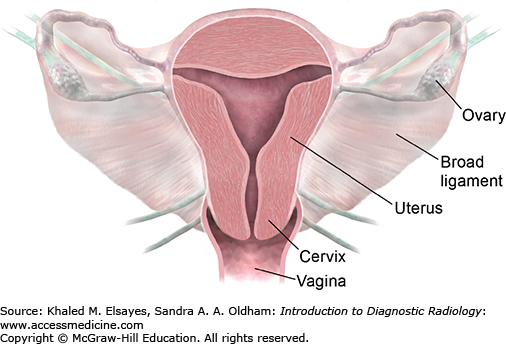
The ovaries are the female pelvic reproductive organs that house the ova and are responsible for the production of sex hormones. They are paired organs located on either side of the uterus within the broad ligament below the uterine (fallopian) tubes. The ovary is within the ovarian fossa, a space that is bound by the external iliac vessels, obliterated umbilical artery, and ureter. The ovaries are responsible for housing and releasing ova, or eggs, necessary for reproduction. At birth, a female has approximately 1 to 2 million ova, but only 300 of these eggs will ever become mature and be released for the purpose of fertilization.
The ovaries are small, oval-shaped, and grayish in color, with an uneven surface. The actual size of an ovary depends on a woman’s age and hormonal status; the ovaries, covered by a modified peritoneum, are approximately 3 to 5 cm in length during childbearing years and become much smaller and then atrophic once menopause occurs. A cross section of the ovary reveals many cystic structures that vary in size. These structures represent ovarian follicles at different stages of development and degeneration.
Ultrasound is the imaging modality of choice for the female pelvis. It is widely available, has broad acceptance by patients as a familiar test, and is relatively inexpensive. High-resolution imaging of transvaginal ultrasound provides high diagnostic accuracy for pelvic pathology. However, there are some shortcomings with this modality, such as the limited field of view, obscuration of pelvic organs by the presence of bowel gas, inherent limitations dependent on patient size, and its dependence on the skill and experience of the operator. The American College of Radiology has provided guidelines for when ultrasound is an appropriate imaging tool for the evaluation of the female pelvis (Table 10.1).
Indications for Pelvic Sonography
| Indications for pelvic sonography include, but are not limited to: |
|---|
|
For a pelvic sonogram performed transabdominally, the patient’s urinary bladder should in general, be distended adequately to displace the small bowel and its contained gas from the field of view. Occasionally, overdistention of the bladder may compromise evaluation. When this occurs, imaging may be repeated after the patient partially empties the bladder.
For a transvaginal sonogram, the urinary bladder is preferably empty. The sonographer or the physician may introduce the vaginal transducer, preferably under real-time monitoring. When possible, a woman member of the physician or hospital’s staff should be present as a chaperone in the examining room if a man is performing the examination.
Ultrasound has high diagnostic accuracy rates for uterine and ovarian abnormalities. MRI should be considered for the evaluation of adnexal pathology when sonographic characteristics are not definitive to determine whether an adnexal mass is ovarian in origin and to determine the likelihood of malignancy. MRI has an established role in the preprocedural and postprocedural assessment for uterine artery embolization, diagnosis of adenomyosis, staging of known endometrial and cervical carcinoma, evaluation of suspected Müllerian ductal anomalies, and presurgical workup for pelvic floor prolapse. Other indications include assessment of the pregnant patient with acute pelvic pain and of fetal anatomy. In most cases, fetal anatomy is well evaluated by ultrasound, but MRI can play a role in problem solving. For cases of acute pelvis and if there is a concern for acute appendicitis, the role of MRI has yet to be established. Beyond the period of organogenesis, CT may be considered. Within the period of organogenesis, however, MRI is a safe alternative, and limited studies to date have shown promising results.
J, Bergin
D Imaging the female pelvis: when should MRI be considered. Appl Radiol. 2008;37(1):9-–24.
VL, Lentz
GM, Lobo
RA, Gershenson
DM. Comprehensive Gynecology. 5th ed. Philadelphia: Mosby Elsevier; 2007.
H. Anatomy, Descriptive and Surgical, The Unabridged Gray’s Anatomy. Philadelphia: Running Press; 1999.
KW. Gross Anatomy. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2000.
CASE 1: ECTOPIC PREGNANCY
A 25-year-old woman presents to the ER complaining of pelvic pain and vaginal bleeding. Quantitative urine β-hCG is positive indicating early pregnancy. Patient has history of pelvic inflammatory disease.
Ectopic pregnancy
Transabdominal and transvaginal pelvic ultrasound (TVS) in addition to color Doppler evaluation. Advantages: readily available, low cost, sensitive, no ionizing radiation, and color Doppler evaluation. The overall sensitivity of TVS to diagnose an ectopic pregnancy is 98.3%, with a specificity of 99.9%, a positive predictive value of 97.5%, and a negative predictive value of 100% [7].
Ultrasound findings of tubal ectopic pregnancy (Figs. C1.1 and C1.2):
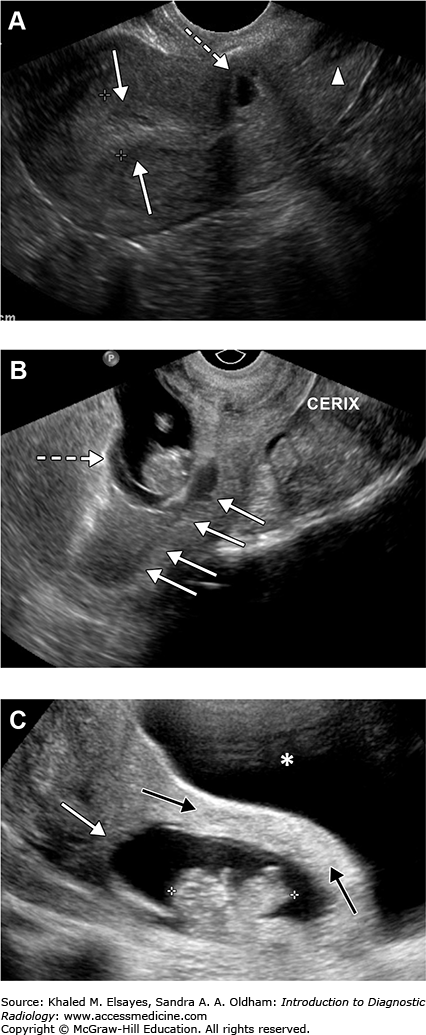
Fig. C1.1
(A) Transverse and longitudinal transvaginal gray-scale ultrasound images of a 26-year-old woman who presented with abdominal pain and positive urine β-hCG show an endometrial cavity full of fluid centrally without evidence of intrauterine pregnancy consistent with pseudosac (calipers). (B) Transverse transvaginal gray-scale ultrasound image of the same patient shows a ringlike mass (arrow) with yolk sac seen outside the uterus in the right adnexa consistent with an ectopic pregnancy.
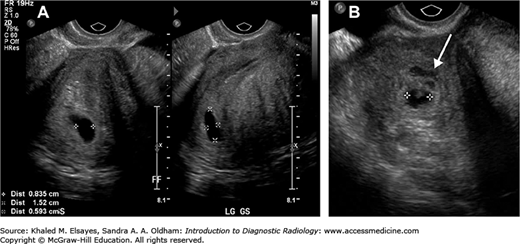
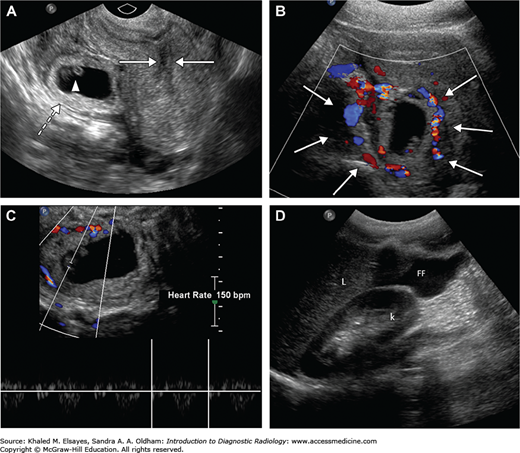
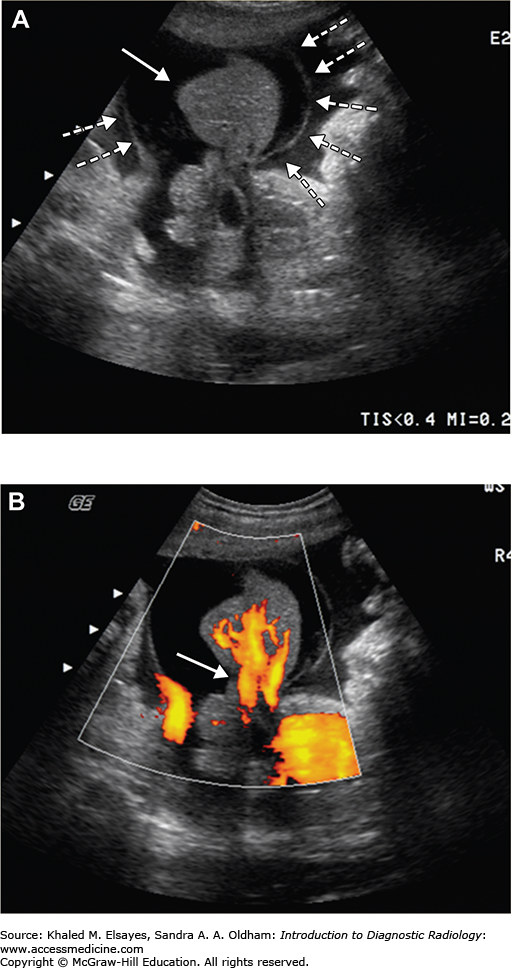
Fig. C1.2
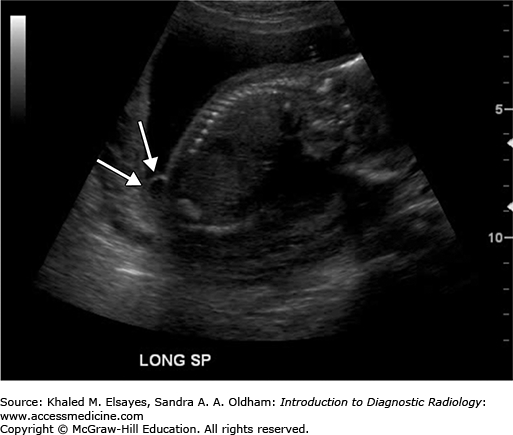
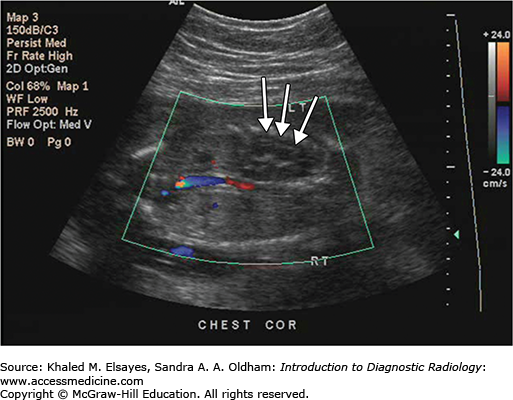
Multiple transabdominal and transvaginal ultrasound images of a different patient with an ectopic pregnancy demonstrating (A) echogenic debris in the endometrial cavity (arrows) and a gestational sac (dashed arrow) with a yolk sac (arrowhead) outside the uterus. (B) “Ring of fire” appearance with prominent blood flow around the echogenic ring of the ectopic pregnancy is also seen (arrows). (C) Cardiac activity is seen in the ectopic pregnancy. (D) Longitudinal view of the right upper quadrant shows free fluid (FF) adjacent to the kidney compatible with a ruptured ectopic pregnancy. Liver (L), kidney (K). Note that “ring of fire” can also be seen with hemorrhagic cysts.
-
Endometrium:
-
No intrauterine pregnancy; no gestational sac, no yolk sac, and no fetal pole in the endometrium.
-
Pseudosac that represents fluid centrally located in endometrial cavity with an absent double decidual reaction. Pseudosac is most often irregular in shape or flat (Fig. C1.1A).
-
-
Fallopian tube or adnexa:
-
Free fluid:
-
The presence of fluid with debris suggesting hemorrhage increases the likelihood of ectopic pregnancy (Fig. C1.2).
-
-
Color Doppler:
-
Ring of color around the echogenic ringlike mass. “Ring of fire” (Fig. C1.2).
-
Ectopic pregnancy accounts for about 2% of all pregnancies and is the most common cause of pregnancy-related mortality in the first trimester. A history of pelvic pain along with bleeding and abnormal β-hCG levels should always trigger an evaluation for an ectopic pregnancy. The fallopian tube is the most common location for an ectopic pregnancy, accounting for about 95% of cases, though there are other rare types of ectopic pregnancies including interstitial, cornual, ovarian, cervical, scar (Fig. C1.3), intra-abdominal, and heterotopic.
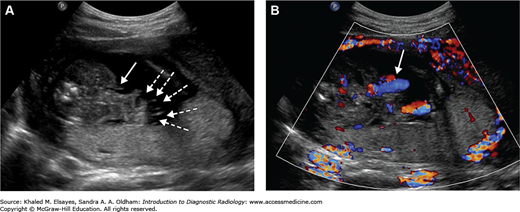
Fig. C1.3
Transabdominal gray-scale ultrasound image of the pelvis in this 32-year-old patient who presented with abdominal pain, positive urine β-hCG, and history of cesarean section 2 years prior to presentation show the rare case of an ectopic pregnancy in a cesarean scar. (A) There is an eccentric gestational sac within anterior myometrium in the lower uterine segment at the site of prior C-section scar (dashed arrow). An empty uterine cavity (arrows) and cervix (arrowhead) are seen. (B) Sagittal transvaginal ultrasound image of the pelvis for the same patient 4 weeks later shows a viable ectopic pregnancy at the site of prior C-section scar (dashed arrow) with an empty uterine cavity filled with blood (arrows). An empty cervix is seen again. (C) Transabdominal ultrasound image shows the eccentric anterior lower uterine gestational sac (white arrow) with thin myometrium (black arrows) between the sac and bladder (asterisk) compatible with scar ectopic pregnancy.
-
Prior ectopic pregnancy
-
History of pelvic inflammatory disease; tubal scarring
-
History of gynecologic surgery
-
Infertility
-
Use of intrauterine device
-
History of placenta previa
-
Use of in vitro fertilization
-
Congenital uterine anomalies
-
History of smoking
-
Endometriosis; increases the risk for tubal scarring from fibrosis
-
Intrauterine exposure to diethylstilbestrol
Ectopic pregnancy in a C-section scar is very rare with an incidence of 1:2,000 pregnancies, and it can lead to life-threatening complications such as uterine rupture and massive hemorrhage. Ultrasound guided methotrexate injection is emerging as the treatment modality of choice in stable patients. Subsequent pregnancies may also be complicated by uterine rupture, hence the uterine scar should be evaluated before as well as during those pregnancies.
-
Intrauterine pregnancy with hemorrhagic corpus luteum cyst: Always check for intrauterine pregnancy, which is diagnosed with intradecidual sign, double decidual sac sign, yolk sac, or embryo.
Adnexal cyst will be in the ovary rather than adjacent to the ovary. Although ovaries can be a rare location for an ectopic pregnancy, the cyst wall will be less echogenic than the wall of an ectopic pregnancy, and an anechoic cyst is unlikely to be an ectopic pregnancy. If diagnosis is unclear, a follow up sonogram and β-hCG will be helpful.
-
Heterotopic pregnancy: Very rare indicating combined intrauterine and extrauterine pregnancy. In such instances pregnancies are typically of similar gestational age.
-
Tubal cyst: Thin-walled anechoic cyst separate from the ovary.
-
Tubo-ovarian abscess: Cervical motion tenderness when performing transvaginal sonography. Elevated white blood cell count
-
Exophytic leiomyoma: Broad base attachment to uterus. Usually multiple with similar echogenicity to other leiomyomas.
Instances where a positive pregnancy test is encountered without evidence of pregnancy could be due to early intrauterine or ectopic pregnancy and miscarriages; follow-up ultrasound and β-hCG should be performed. If it is an early pregnancy, follow-up β-hCG levels should show normal doubling in 2 days, while in ectopic pregnancy or miscarriages β-hCG should not rise normally or should decrease, although normal rise could be seen in 21% of ectopic pregnancy cases. Miscarriages can cause retrograde flow of blood into the tube mimicking ectopic pregnancy.
-
Watchful waiting in stable patient for spontaneous abortion.
-
Methotrexate in reliable patients with ectopic pregnancy less than 5 cm and no fetal cardiac activity.
-
Laparoscopy if patient presents with hemodynamic instability and possible tubal rupture.
EP, Bhatt
S, Dogra
VS. Diagnostic clues to ectopic pregnancy. RadioGraphics. 2008;28(6):1661-–1671.
[PubMed: 18936028]
D. Ectopic pregnancy. Radiology. 2007;245(2): 385-–397.
[PubMed: 17940301]
DA, Poder
L, Goldman
M,
et al. Role of sonography in the recognition, assessment, and treatment of cesarean scar ectopic pregnancies. J Ultrasound Med. 2008;27(5):779-–783.
[PubMed: 18424654]
KM, Huang
LW, Lin
YH,
et al. Cesarean scar pregnancy: issues in management. Ultrasound Obstet Gynecol. 2004;23(3):247-–253. doi:10.1002/uog.974.
[PubMed: 15027012]
MA, Haberman
S, Levgur
M. Cesarean scar ectopic pregnancies: etiology, diagnosis, and management. Obstet Gynecol. 2006;107(6):1373-–1381. doi:10.1097/01. AOG.0000218690.24494.ce.
[PubMed: 16738166]
C, Dickinson
JE. Caesarean scar ectopic pregnancy: a single centre case series. Aust N Z J Obstet Gynaecol. 2009;49(5):451-–455. doi:10.1111/j.1479-828X.2009.01067.x.
[PubMed: 19780724]
E, Papageorghiou
AT, Condous
G,
et al. The diagnostic effectiveness of an initial transvaginal scan in detecting ectopic pregnancy. Hum Reprod. 2007;22:2824-2828.
CASE 2: GESTATIONAL TROPHOBLASTIC DISEASE
A 48-year-old Asian woman who is 12 weeks pregnant presents to the emergency department with painless vaginal bleeding and hyperemesis. The patient has never had any primary workup or ultrasound studies during the first trimester. On clinical examination the patient seems to have a uterus that is larger than the expected gestational age and an elevated blood pressure. Laboratory workup shows β-hCG levels of 198,000.
Complete hydatidiform mole
Transabdominal and transvaginal pelvic ultrasound. Advantages: readily available, low cost, sensitive, no ionizing radiation.
Ultrasound findings for complete hydatidiform mole:
-
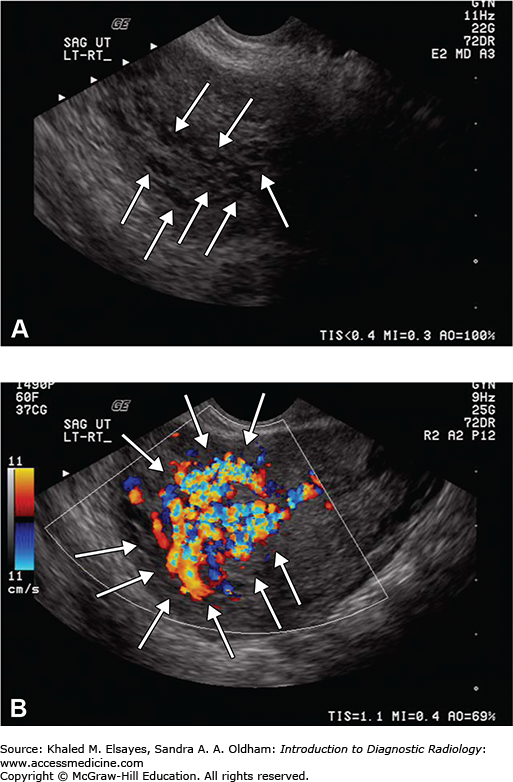
Uterine cavity filled with multiple hypoechoic areas of varying size and shapes (vesicles) resembling a “bunch of grapes” that increase in size with gestational age is the best imaging clue (Fig. C2.1).
-
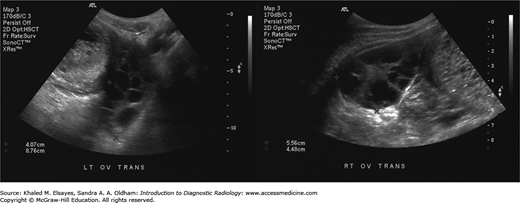
Theca lutein cysts secondary to very high beta human chorionic gonadotropin levels (β-hCG) in up to 50% of cases. “Soap-bubble” or “spoke wheel” appearance (Fig. C2.2).
-
Color Doppler: very vascular with very high velocity blood flow (Fig. C2.1).
-
First trimester moles may have a sonographic appearance simulating that of an incomplete abortion.
Ultrasonography has replaced all other means in early screening and is the examination of choice for initial diagnosis. However, CT typically shows an enlarged uterus with central areas of low attenuation, and MRI typically shows a uterine mass of heterogeneously T2 high signal intensity that distends the endometrial cavity. The T2 high signal intensity is mainly due to numerous cystic spaces, which typically show low T1 signal intensity. Foci of T1 increased signal intensity can also correspond to areas of hemorrhage.
-
Multiple gestations
-
Invasive mole
-
Choriocarcinoma
-
Triploidy
-
Threatened abortion
-
Ectopic pregnancy
-
Placental hydropic degeneration: This represents hydropic changes without proliferation often seen after failed pregnancy due to fetal demise or anembryonic gestation. This can look similar to complete hydatidiform mole, but it is less vascular and clinically associated with low β-hCG levels rather than high levels as seen with complete moles.
-
Placental sonolucencies (pseudomole): This is often a normal finding after 25 weeks of gestation, but it could be associated with preeclampsia and intrauterine growth restriction.
-
Partial mole (also known as triploidy): Similar in appearance to complete mole; however, the presence of fetal tissue is specific to partial moles. Differential diagnosis includes twin gestation, one of which is a complete mole, or placental hemorrhages discussed in Fig. C2.3.
-
Invasive mole or choriocarcinoma: Those are largely indistinguishable on imaging and look similar to complete moles on ultrasonography. MRI has the ability to demonstrate myometrial and parametrial invasion; however, again invasive mole vs choriocarcinoma is an exclusively histological diagnosis even though the presence of metastasis can suggest choriocarcinoma rather than invasive mole.
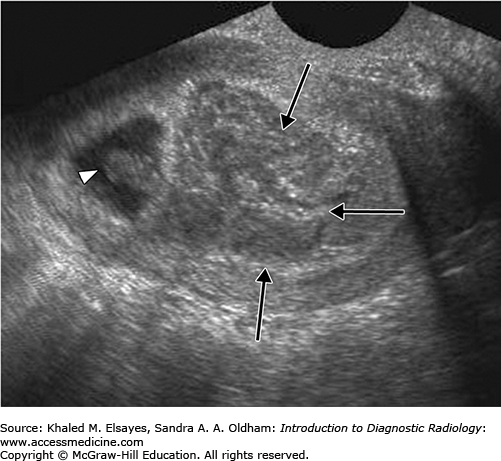
Fig. C2.3
Transvaginal gray-scale ultrasound image shows echogenic material filling the majority of the uterine cavity (arrows). Adjacent to this material is a gestational sac containing an embryo (arrowhead). These findings were due to a pathologically proven partial mole. The differential diagnosis for this appearance includes twin gestation, one of which is a complete mole. Differential also includes a large subchorionic hemorrhage, which can be distinguished on the basis of the β-hCG level and the presence of vascular flow within the molar tissue. No flow would be expected in a hemorrhage. Used with permission from Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-1391.
Complete hydatidiform moles are the most common gestational trophoblastic neoplastic tumors and are considered essentially benign. They are mainly due to proliferative growth of trophoblastic tissue and may become invasive in 12% to 15% of cases or develop into choriocarcinoma in 5% to 8% of the cases.
A complete mole is typically formed by a single (90%) or two (10%) sperm combining with an ovum that has an inactive nucleus leading to a 100% paternal genetic makeup, which most commonly has a karyotype of 46, XX. This chromosomal abnormality results in loss of the embryo and proliferation of trophoblastic tissue.
A partial mole on the contrary is typically formed by a normal ovum that is fertilized by two sperms or one sperm that duplicates itself yielding the karyotype of 69, XXX or 69, XXY (triploidy). Fetal tissue is present with partial moles, but fetal growth is often complicated by severe symmetric growth restriction, multiple structural anomalies, and oligohydramnios. Partial moles look similar to complete mole on ultrasound evaluation; however, the presence of fetal tissue is unique for partial moles (Fig. C2.3).
Complete hydatidiform moles have a higher risk of developing into choriocarcinoma than do partial moles.
The incidence of complete moles in the United States is 0.5:1,000 in comparison to 8:1,000 in Asia.
Prognosis for complete mole is overall good. Malignant degeneration to an invasive form or choriocarcinoma can occur; those usually tend to be generally highly chemosensitive and carry a much better cure rate than other comparable malignancies despite their aggressiveness.
-
Age: < 20 y (2 fold), > 40 y (10 fold), and >50 y (50% chance).
-
Prior molar pregnancy.
-
Contraception: Combined oral contraceptive pills have been proved to double the chances of molar pregnancy.
-
Previous spontaneous abortion: double the incidence.
-
Multiple sexual partners.
-
Suction and curettage followed by metastatic disease workup.
-
Hysterectomy advocated by gynecologists in patients over 35 years old who are not interested in preserving fertility.
-
After evacuation, β-hCG levels should be monitored weekly until it is undetectable followed by monthly monitoring for 6 to 24 months.
-
In women with persistent disease or chemotherapy resistant disease, angiography is useful in workup of myometrial invasion and surgical management.
-
Pregnancy should be postponed if desired to avoid confusing the clinical picture while monitoring β-hCG levels.
C, Atri
M, Arenson
AM,
et al. Sonographic diagnosis of gestational trophoblastic disease and comparison with retained products of conception. J Ultrasound Med. 2006;25 (8):985-–993.
[PubMed: 16870892]
Q, Lei
XY, Xie
Q,
et al. Sonographic and Doppler imaging in the diagnosis and treatment of gestational trophoblastic disease: a 12-year experience. J Ultrasound Med. 2005;24:15-–24.
[PubMed: 15615924]
JR, Gorengaut
V, Brown
JJ. MR imaging of maternal disease of the abdomen and pelvis during pregnancy and the immediate postpartum period. RadioGraphics. 2004;24(5):1301-–1316.
[PubMed: 15371610]
KM, Trout
AT, Friedkin
AM,
et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics 2009;29:1371-–1391.
[PubMed: 19755601]
CASE 3: PLACENTAL PATHOLOGY
A 40-year-old woman who presents at 30 weeks of gestation with vaginal bleeding.
Placenta previa, placental abruption
Transvaginal and transabdominal ultrasound. Advantages: readily available, low cost, sensitive, no ionizing radiation.
Antepartum hemorrhage is defined as vaginal bleeding between 20 weeks of gestation and delivery, and it is considered a major factor of maternal and fetal morbidity and mortality. Placenta previa and placental abruption are by far the most common causes of antepartum hemorrhage.
Placenta previa refers to an abnormally located placenta in which the placenta is near or covers the cervical internal os. Placental abruption represents separation of the placenta from the uterine wall. While both placenta previa and placental abruption usually present with vaginal bleeding, placental abruption seems to be associated with abdominal/pelvic pain that is sudden in onset. Transvaginal and transabdominal ultrasound are essential for diagnosis.
ACR appropriateness criteria in order of preference for second and third trimester bleeding with or without pain:
-
US transabdominally. If cervix and placenta are not visualized transabdominally, further evaluation with transvaginal or transperineal US should be done unless contraindicated as discussed below.
-
US transvaginal. Considered safe in patients with placenta previa or placental abruption, even in those who present with vaginal bleeding [9]. This can be done particularly when transabdominal US is inconclusive. If there is evidence of ruptured membranes or open cervix with bulging amniotic sac at or below the external os, transvaginal US is contraindicated.
-
US transperineal. This is least preferred.
Placenta previa most often presents with painless bleeding, and the diagnosis should never be made before 15 weeks of gestation. There are four types of placenta previa based on position of the placenta in relation to the internal cervical os (Table C3.1). Screening to rule out placenta previa should be done as part of the second trimester anatomic survey examination, and if a complete or central placenta previa is diagnosed, those will not likely resolve with advancing pregnancy, and appropriate action needs to be made such as bed rest, hospitalization, maternal blood transfusion, and delivery will be likely with cesarean section. However, if marginal or low-lying placenta is seen, a repeat ultrasound at 32 weeks should be done to ensure the placental edge has migrated farther away from the internal os [5]. Advance maternal age (≥35) is associated with increased incidence of placenta previa at time of delivery. Prognosis of placenta previa is excellent if picked up early during antenatal care and subsequently appropriately managed.
Subtypes of Placenta Previa
| Placenta Previa Subtype | Description |
|---|---|
| Low-lying placenta (Fig. C3.2) | Lower placental margin is within 2 cm of the internal cervical os. |
| Marginal previa (Fig. C3.3) | Placenta extends to the edge of the internal os but does not cover it. |
| Complete previa (Fig. C3.4) | Placenta covers the internal os. |
| Central previa (Fig. C3.5) | Central placenta is implanted directly over the internal os. |
US will reliably exclude placenta previa if the lower placental edge is shown to lie >2 cm away from the internal cervical os (Fig. C3.1). This is most often accomplished by transabdominal examination of the cervix and lower uterine segment with the bladder moderately full; but the bladder should not be so full as to artificially elongate the cervix [4]. Focal myometrial contraction can cause the uterine walls to come closer together and falsely show placenta previa; however, this will resolve once contractions resolve.
Fig. C3.1
Transvaginal US image obtained at 27 weeks gestation shows a posterior placenta (P) without previa. The most caudal tip of the placenta is nearly 5 cm (cursors) from the internal cervical os. Distances greater than 2 cm are considered normal.
Used with permission from Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-1391.
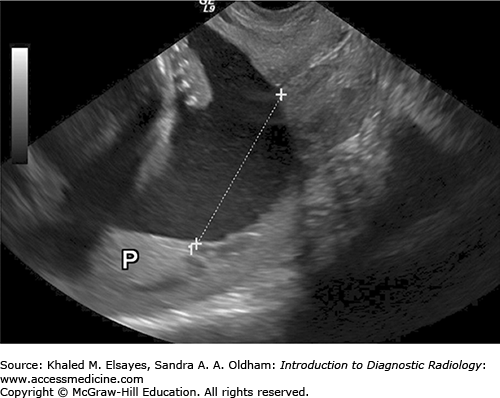
Fig. C3.2
Transvaginal US image obtained at 20 weeks gestation shows a low-lying placenta (P). The placental margin comes to within 0.7 cm of the internal cervical os.
Used with permission from Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-1391.
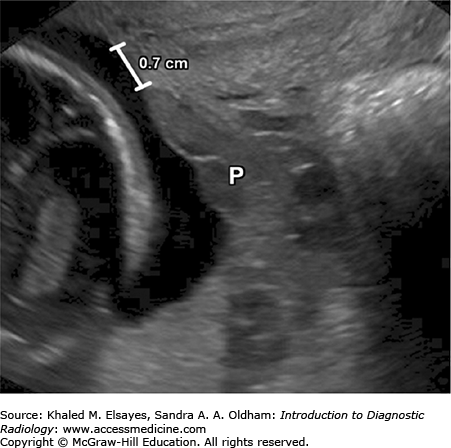
Fig. C3.3
Transvaginal US image obtained at 19 weeks gestation shows marginal placenta previa. The placental tip (T) is located immediately at the internal cervical os (O) but does not cover it. P = body of the placenta.
Used with permission from Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-1391.
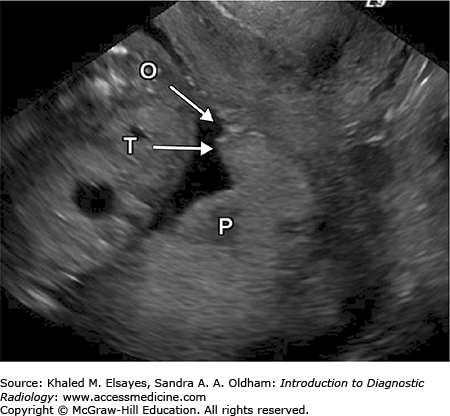
Fig. C3.4
Transvaginal US image obtained at 20 weeks gestation shows complete placenta previa. The placenta (arrow) entirely covers the internal cervical os (arrowhead).
Used with permission from Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-1391.
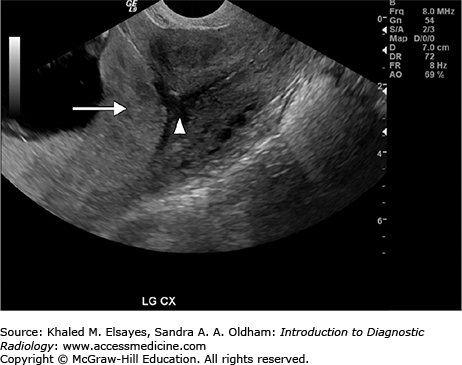
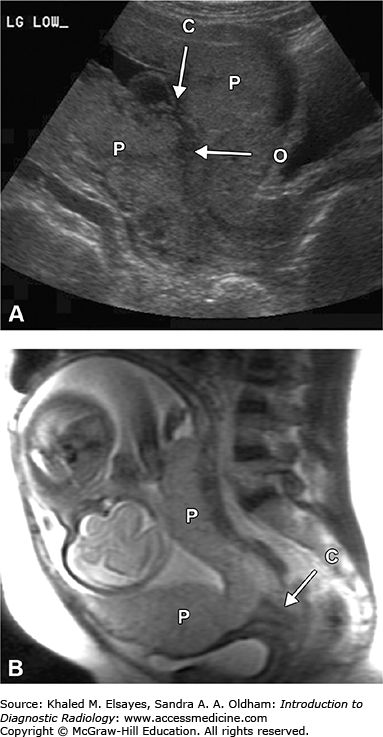
Fig. C3.5
Transabdominal US image obtained at 18 weeks gestation (A) and sagittal SSFSE MR image obtained at 29 weeks gestation (B) show central placenta previa. The placenta (P) entirely covers the internal cervical os (O) in (A). In the case shown in the US image, the umbilical cord (C) in (A) inserts immediately above the os. C in (B) = uterine cervix.
Used with permission from Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-1391.
Placental abruption can be diagnosed by ultrasonography by showing placental detachment with an accompanying clot (Fig. C3.6). If gray-scale sonography is challenging, color Doppler can be helpful sometimes that shows no flow in blood clot.
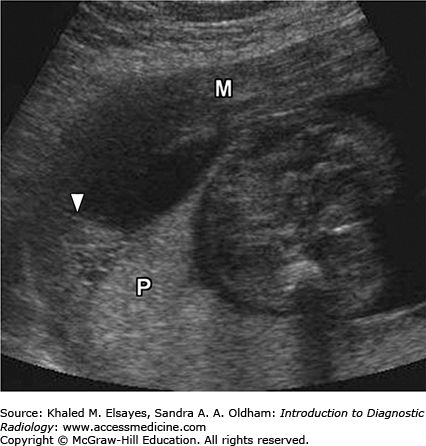
Fig. C3.6
US image shows placental abruption in another patient. A crescenteric collection of predominantly hypoechoic fluid lifts the edge of the placenta (P) away from the underlying myometrium (M). The fluid collection contains layering high-attenuation material (arrowhead), a finding consistent with blood.
Used with permission from Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-1391.
Risk factors for developing placental abruption include smoking, blunt abdominal trauma, cocaine use during pregnancy, advanced maternal age, prior C section, leiomyoma, prior placental abruption, and multiparity.
In cases of placental abruption, close monitoring of the mother and fetus should be performed with serial ultrasound follow-up. If there is any evidence of placental insufficiency including bradycardia and increased systolic/diastolic ratio in the umbilical cord, early delivery and even cesarean section in cases of acute distress should be done rather than expectant management.
KM, Trout
AT, Friedkin
AM,
et al. Imaging of the placenta: a multimodality pictorial review. RadioGraphics. 2009;29:1371-–1391.
[PubMed: 19755601]
A, Thilaganathan
B. Recent advances in the management of placenta previa. Curr Opin Obstet Gynecol. 2004;16(6):447-–451.
[PubMed: 15534438]
J, Ngambu
NF, Corr
P. Imaging techniques to identify morbidly adherent placenta praevia: a prospective study. J Obstet Gynaecol. 2004;24(7):742-–744.
[PubMed: 15763778]
E. Transvaginal and transabdominal ultrasound for the diagnosis of placenta praevia. J Obstet Gynaecol.1999;19(2):152-–154.
[PubMed: 15512257]
BS, Bowie
JD, Carroll
BA, Kliewer
MA, Weber
TM. Diagnosis of placenta previa during the third trimester: role of transperineal sonography. AJR. 1992;159(1):83-–87.
[PubMed: 1609727]
EC, Roberts
CL, Nassar
N, Algert
CS. Test characteristics of placental location screening by transabdominal ultrasound at 18-20 weeks. Ultrasound Obstet Gynecol. 2006;28(7):944-–949.
[PubMed: 17121427]
Y, Nghiem
HV, Nodell
C,
et al. Sonography of obstetric and gynecologic emergencies: part I, obstetric emergencies. AJR. 2000;174(3):641-–649.
[PubMed: 10701602]
G, Brunelli
R, Di
Tola M,
et al. MR imaging in the evaluation of placental abruption: correlation with sonographic findings. Radiology. 2011;259(1):222-–230.
[PubMed: 21330568]
EE, Pham
DH. Placental abruption and subchorionic hemorrhage in the first half of pregnancy: US appearance and clinical outcome. Radiology. 1986;160(1):109-–112.
[PubMed: 3520643]
CASE 4: CLUBFOOT
A 25-year-old woman who presents at 20 weeks for routine second trimester ultrasound. Sonographer notices an abnormally inward oriented foot.
Clubfoot
Transabdominal pelvic ultrasound. Advantages: readily available, low cost, sensitive, no ionizing radiation.
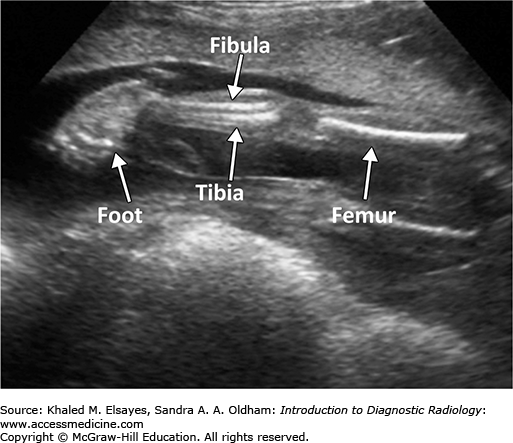
Sonographic findings for clubfoot (Figs. C4.1 and C4.2):
-
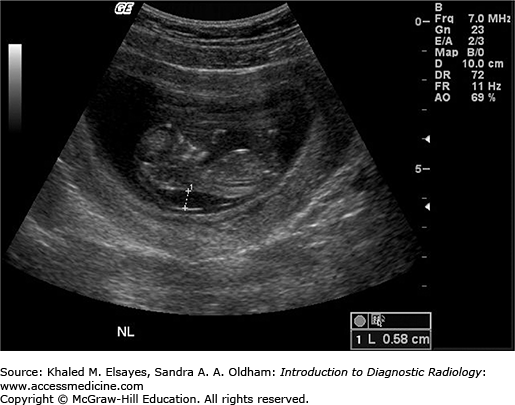
Normally, in the coronal plane, the long axis of the foot should not be seen in the same plane as the long axis of the lower leg; however, in clubfoot the long axis of the foot and lower leg will be seen in the same coronal plane.
-
Clubfoot shows an abnormal orientation of foot and ankle, where the foot is inverted at the ankle and plantar flexed (talipes equinovarus, equino = plantar flexed, varus = inward orientation).
-
3-D ultrasound may be helpful as well.
-
After birth, plain films of neonate with clubfoot will show hind foot deformity with the talus and calcaneus parallel to each other.

Clubfoot has a high association with aneuploidy, particularly with trisomy 18, and other entities such as oligohydramnios, spina bifida, or a result of intrauterine growth restriction. There is a positive familial correlation. Usually manifests as bilateral (Fig. C4.2) but can be an isolated finding. It is usually found during routine second trimester fetal survey.
Rocker bottom foot:
-
Convex foot secondary to a vertical talus orientation, which can also have an associated clubfoot.
-
Strong association with trisomy 18.
Amniotic band syndrome:
-
Abnormal amnion may cause fetal parts to be restricted.
-
May result in missing toes and foot deformity.
Surgically corrected based on severity of deformity. Most result in surgical management; however, conservative management as done for nonsevere minority. Decision for surgery is not made until at least 3 months of age postnatal.
E, Fraracci
L, Farsetti
P,
et al. Validity of the anteroposterior talocalcaneal angle to assess congenital clubfoot correction. AJR. 2004;182(5):1279-–1282.
[PubMed: 15100132]
L, Benson
CB. Outcome of fetuses with clubfeet diagnosed by prenatal sonography. J Ultrasound Med. 2004;23(4):497-–500.
MJ, Cano
S, Palau
J,
et al. Prenatal diagnosis of clubfoot in low-risk population: associated anomalies and long-term outcome. Prenat Diagn. 2008;28(4):343-–346.
[PubMed: 18382991]
K, Jebens
N, Blaas
HG,
et al. Prenatal ultrasound detection of talipes equinovarus in a nonselected population of 49 314 deliveries in Norway. Ultrasound Obstet Gynecol. 2007;30(6):838-–844.
[PubMed: 17787031]
CASE 5: CHIARI II MALFORMATION
A 38-year-old woman who is 16 weeks pregnant presents for fetal ultrasound due to abnormal maternal serum screening test showing elevated maternal serum α-fetoprotein (AFP).
Open neural tube defect (ONTD)
Transabdominal pelvic ultrasound. Advantages: readily available, low cost, sensitive, no ionizing radiation.
Chiari II malformation is a fairly common congenital anomaly of the spine and posterior fossa characterized by spina bifida (meningocele/myelomeningocele) and posterior fossa hypoplasia.
The pathophysiology behind Chiari II malformation is thought to be secondary to CSF leakage through open spinal dysraphism during the fourth week of gestation allowing for CSF to flow through the central canal so it is therefore not maintained in the ventricular system. Ventricular distention is the driving force for development of the calvaria, and given its absence, the posterior fossa never fully develops. Later during gestation, the rhombencephalon rapidly develops, forcing the cerebellum cephalad and caudad along with the brainstem due to hypoplasia of the posterior fossa. Ultimately the flow of CSF through the foramina of Luschka and Magendie becomes blocked or impaired by crowding of structures in the posterior fossa explaining the ventriculomegaly and hydrocephalus in Chiari II patients.
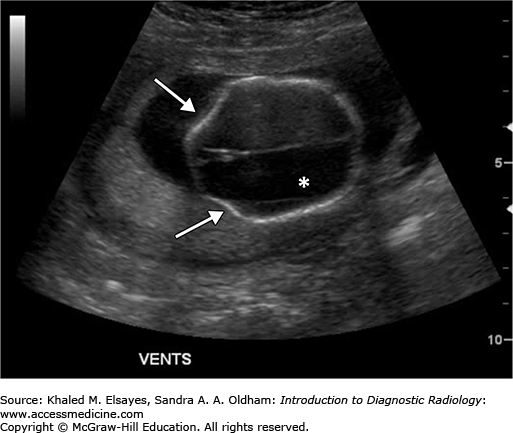
Ultrasound findings for Chiari II malformation:
-
Posterior fossa compression: Small or obliterated cisterna magna. This is the most common finding, which is seen on routine axial posterior fossa view and considered when the cisterna magna measures less than 3 mm. The cerebellum usually is small and compressed; severe compression of the cerebellum leads to banana sign.
-
Ventriculomegaly: Normal unilateral transverse lateral ventricle atrial dimension measured in the posterior horns just above the level of the thalami should not exceed 10 mm. Mild ventriculomegaly (10-12 mm) is seen in 50% of fetal ultrasounds for Chiari II malformation. Usually ventriculomegaly progresses during pregnancy with 90% of Chiari II fetuses having ventriculomegaly at birth (Fig. C5.1).
Triangular shaped ventricle sometimes seen.
-
Frontal bone concavity, also known as “lemon sign”: This sign is nonspecific and can be seen in 1% of all second trimester fetuses. It is usually transient and often seen in the second trimester only (Fig. C5.1).
-
Dorsal vertebral defect: Eight percent of the defects have an overlying sac. If there is skin covering the defect, this will not be Chiari II malformation. The defect could either contain a meningocele (simple anechoic sac) or a myelomeningocele (heterogenous complex sac). Twenty percent have no sac, also known as myeloschisis. The ONTD is lumbar > sacral > thoracic > cervical (Fig. C5.2).
-
Clubfoot is seen in 24% of Chiari II cases.
-
Scoliosis and/or kyphosis are usually seen at the level of the ONTD.
-
Chiari II malformation is associated with high morbidity and mortality with about 35% of live-born babies dying within the first 5 years.
Clinical symptomatology varies in severity depending on the range of anatomical severity. Common clinical presentations include those of brain stem dysfunction, cranial nerve palsies, neurogenic bladder, those related to myelomeningocele, hydrocephalus, musculoskeletal, and kyphoscoliosis.
Chiari II malformation is associated with trisomy 18 and 13, with slight increase in risk with advanced maternal age.
Folate deficiency and teratogenic anticonvulsants have been related to Chiari II malformation as they are known to cause open neural tube defects.
An elevated maternal serum α-fetoprotein can trigger antenatal diagnosis. If any suspicious findings are seen on ultrasound, a fetal MRI should be obtained to better detect and characterize the full constellation of findings associated with Chiari II malformation.
Once the diagnosis is established antenatally, arrangement should be made for cesarean delivery at term to decrease risk of meningomyelocele sac rupture and decrease risk of infection. An immediate postnatal ONTD surgery should be done, and almost 80% need ventriculoperitoneal shunting. In utero interventions are evolving.
Preventive treatment with folic acid at the preconception stage can reduce the risk for developing ONTD and decrease recurrence by about 70%.
Differential diagnosis for ventriculomegaly (hydrocephalus):
-
Aqueductal stenosis: Obstruction of the aqueduct of Sylvius leading to noncommunicating hydrocephalus, which is often severe and progressive. However, in this case, a normal posterior fossa is seen.
-
Dandy-Walker malformation: Partial or complete agenesis of the cerebellar vermis leading to enlargement of the cisterna Magana. The fourth ventricle is communicating with cisterna magna and often ventriculomegaly is seen.
Communicating hydrocephalus secondary to infection or hemorrhage.
Differential diagnosis for calvarial abnormalities:
-
Craniosynostosis: Premature suture fusion leading to abnormal calvarial shape and may cause a small posterior fossa however spine is most often normal.
-
Isolated frontal bone concavity: Seen in 1% of normal fetuses.
T, Mark
EK, Brooks
BS. MR imaging of Chiari II malformation. AJR. 1988;150(1):163-–170.
[PubMed: 3257116]
DM. The Chiari malformations. J Neurol Neurosurg Psychiatr. 2002;72(suppl 2):ii38-–ii40.
[PubMed: 12122202]
TP, Pudlowski
RM, Naidich
JB,
et al. Computed tomographic signs of the Chiari II malformation. Part I: Skull and dural partitions. Radiology. 1980;134(1):65-–71.
[PubMed: 7350637]
JT, Oakes
WJ, Boyko
OB. MR imaging of hindbrain deformity in Chiari II patients with and without symptoms of brainstem compression. AJNR. 1989;10(2):293-–302.
[PubMed: 2494848]
TP, Mclone
DG, Fulling
KH. The Chiari II malformation: Part IV. The hindbrain deformity. Neuroradiology. 1983;25(4):179-–197.
[PubMed: 6605491]
MA, Venes
JL, Rubin
JM. Arnold-Chiari II malformation: intraoperative real-time US. Radiology. 1987;164(3):799-–804.
[PubMed: 3303122]
WJ. Spina Bifida, Management and Outcome. Springer; 2008. ISBN:8847006511.
CASE 6: CONGENITAL PULMONARY AIRWAY MALFORMATION
A 28-year-old woman with abnormal chest findings on anatomical fetal ultrasound at 20 weeks of gestation.
Congenital pulmonary airway malformation (CPAM), also known previously as congenital cystic adenomatoid malformation (CCAM), is a lung hamartoma with proliferation of terminal bronchioles and lack of normal alveoli. The hamartomatous lesion communicates with the tracheobronchial tree and is supplied by the pulmonary artery and drained by the pulmonary vein. Terminology has been changed to better reflect the developmental disorder of airway morphogenesis as such a lesion can be neither cystic nor adenomatoid.
CPAM is rare; however, it is considered the most common respiratory tract congenital malformation and accounts for about 75% of fetal lung masses encountered antenatally. The reported incidence rate of CPAM ranges from 1 in 11,000 to 1 in 35,000 live births with a higher incidence in midtrimester ultrasounds due to spontaneous resolution as will be discussed later.
The pathogenesis of such lesions is poorly understood. There are no genetic causes or recurrence risk described; however there is association with other abnormalities in 3% to 12% of the cases, most commonly other lung malformations, including sequestrations, and renal anomalies.
CPAMs are usually discovered incidentally on antenatal ultrasound seen as cystic or echogenic lung mass and usually show greatest growth at 20 to 26 weeks of gestation. Ninety-five percent of those are unilateral and usually affect one lobe without any definite side of predilection.
Ultrasound findings of CPAM (Fig. C6.1):
-
Variable appearance from solid (microcystic) to complex cystic mass (macrocystic). There are at least three subtypes of (CPAM) classified based on size of cyst. Type I is the most common one (70%) and has one or more large dominant cysts (3-10 cm). Type II represents about 20% of all CPAM cases and consist of smaller cysts measuring less than 2 cm in diameter. Type III represents about 10% of cases and has only microcysts measuring less than 5 mm in diameter. Type III typically involves an entire lung and has a worse prognosis.
-
Color Doppler evaluation shows the mass is supplied by the pulmonary artery and drained by the pulmonary vein; however, this can be difficult to demonstrate.
-
Heart is displaced.
-
Stomach is in normal location.
-
Hydrops, which is the most important predictor factor for outcomes and occurs in < 10% of cases leading to dismal prognosis.
-
Polyhydramnios, which may result from compression of the esophagus and is associated with hydrops.
CPAM has increased risk for developing hydrops fetalis and fetal demise especially if represented by a large dominant cyst or if the CPAM volume ratio (CVR) > 1.6, which can be calculated sonographically (CPAM volume/head circumference).
The majority of CPAM lesion stabilize or regress in utero over the course of pregnancy, and once the diagnosis is suspected antenatally, weekly ultrasound monitoring should be performed until growth stabilizes with special attention to developing hydrops. If CVR > 1.4, betamethasone should be considered, which has been shown to decrease growth. In the case where hydrops is seen, in utero interventions should be considered as almost 100% mortality is seen if untreated. Otherwise excellent prognosis is seen without hydrops even if large at the time of diagnosis.
Postnatally, CPAM patients have increased risk for neonatal complications including air trapping and pneumothorax as well as infection, which can also present later in life. There is a small risk for malignant transformation throughout childhood and adulthood.
Delivery should be done in a tertiary facility capable with dealing with the abovementioned complications, and postnatal workup should be performed for all lesions even if regressed in utero or even in asymptomatic individuals by obtaining CT of the chest with contrast as CXR can fail to identify it. Most authors believe that the risk of infection and malignancy warrants resection, which is usually performed at 1 month of age or later, as early resection can maximize compensatory lung growth.
-
Bronchopulmonary sequestration (BPS): Indistinguishable from microcystic CPAM on gray-scale imaging. Feeding vessel is from aorta, and 90% are left-sided with ipsilateral effusion.
-
Hybrid lesion (CPAM + BPS): Dual pathology has been reported in as many as 50% of echogenic lung mass cases, and such diagnosis should be considered when a systemic vessel supplies a cystic lung mass.
-
Congenital diaphragmatic hernia: Peristalsis on ultrasonography is pathognomonic with small abdominal circumference due to absent normal fluid-filled stomach and small bowel loops.
-
Congenital lobar obstruction: Uniformly echogenic and usually in the upper lobes. This is rarely diagnosed in utero and usually manifests postnatally as lobar emphysema.
-
Teratoma: Solid and cystic components with calcifications, which is the most specific component.
-
Tracheal atresia: Can be confused for bilateral CPAM. Usually associated with inversion of the diaphragm with fluid-filled trachea and bronchi as well as ascites.
-
Other cystic masses: These include bronchogenic cyst, esophageal duplication cyst, and neuroenteric cyst. Such lesions are more often seen in the mediastinum rather than the lungs.
ML, Stocker
JT. Congenital cystic adenomatoid malformation. RadioGraphics. 1991;11(5): 865-–886.
[PubMed: 1947321]
T, Madrid
C, Novo
S,
et al. Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology. RadioGraphics. 2004; 24(1):e17.
[PubMed: 14610245]
GW. Pediatric chest imaging. Curr Opin Radiol. 1992;4(5):36-–43.
[PubMed: 1524979]
J, Stern
EJ. Chest Radiology, the Essentials. Lippincott Williams & Wilkins; 2007. ISBN:0781763142.
MI. Prenatal Diagnosis. McGraw-Hill Professional; 2006. ISBN:0838576826.
EY, Boiselle
PM, Cleveland
RH. Multidetector CT evaluation of congenital lung anomalies. Radiology. 2008;247(3):632-–648.
[PubMed: 18487532]
M, Albig
M, Knoll
U,
et al. Ultrasound Diagnosis of Fetal Anomalies. Thieme; 2003. ISBN:1588902129.
WS, Yeh
GP, Tsai
HD.
et al. Prenatal diagnosis of congenital cystic adenomatoid malformations: evolution and outcome. Taiwan J Obstet Gynecol. 2009;48(3):278-–281.
[PubMed: 19797020]
AM, Ganapathy
R, Crowley
S,
et al. Neonatal outcome of antenatally diagnosed congenital cystic adenomatoid malformations. Ultrasound Obstet Gynecol. 2005;26(2):150-–153.
[PubMed: 16038013]
H, Fink
MA, Crameri
J,
et al. Congenital cystic adenomatoid malformation: monitoring the antenatal and short-term neonatal outcome. Aust N Z J Obstet Gynaecol. 2008;48(5):462-–466.
[PubMed: 19032660]
CASE 7: FIRST TRIMESTER INCREASED NUCHAL TRANSLUCENCY
A 40-year-old woman who is 12 weeks pregnant who was referred for fetal ultrasound by her OB-GYN doctor due to abnormal maternal serum screening test.
Aneuploidy, congenital heart defects, hydrops
Transabdominal ultrasound. Advantages: readily available, low cost, sensitive, no ionizing radiation.
Ultrasound findings for increased nuchal translucency (Fig. C7.1):
-
Nuchal translucency (NT) refers to fluid under the skin in the back of the fetal neck.
-
Measurement performed at 11 to 14 weeks of gestational age.
-
NT ≥ 3 mm always abnormal.
-
Simple fluid without septations.
Pitfalls: Beware of amnion. Gravity dependent fetus may lie on amnion. Wait for fetus to move away and show amnion and skin on same image to avoid the pitfall.
Pregnant patients often are referred by their OB-GYN physician after an abnormal first trimester maternal serum results such as β-human chorionic gonadotropin or pregnancy-associated plasma protein A. However, Nuchal translucency (NT) measurement is now recommended in all 11 to 14 weeks pregnancies. The larger the NT, the worse the prognosis. The normal cutoff is equal to 3 mm or less. If suspected, chorionic villus sampling should be obtained.
Increased NT is found in aneuploidy and congenital heart defect and is associated with hydrops. Trisomies, particularly trisomy 21 (most common), trisomy 18, trisomy 13, and Turners syndrome have increased nuchal translucency. There is approximately 90% detection rate for aneuploidy. Trained ultrasonographers with correct caliper placement are important. Increased maternal age has increased incidence of fetal aneuploidy.
Top differential diagnoses for increased nuchal fold translucency:
-
Chorioamniotic separation: Amnion mistaken for fetal skin. Wait for fetus to move away and show amnion and skin on same image to avoid this pitfall.
-
Cystic hygroma: Large fluid collections with septations behind fetal neck.
-
Poor measurement technique: Calipers not correctly placed. Skilled sonographers are necessary.
Nuchal fold thickness is a different parameter that is measured during second trimester fetal ultrasound survey (16-22 weeks), and it is not to be confused with nuchal translucency (which is measured in the first trimester as discussed above).
The proposed theory for the cause of increased nuchal fold thickness is edema occurring secondary to congenital heart disease and lymphatic obstruction in association with aneuploidy such as Down (trisomy 21), Edwards (trisomy 18), Patau (trisomy 13), and Turner (monosomy 45, X) syndromes.
Nuchal fold thickness is measured on an axial image through the head at the level of the thalami, cavum septum pellucidum, and cerebellar hemispheres with one caliper at the outer limit of the occipital bone and the other one at the outer aspect of the skin edge (Fig. C7.2). An abnormal value is one that is more than 6 mm.
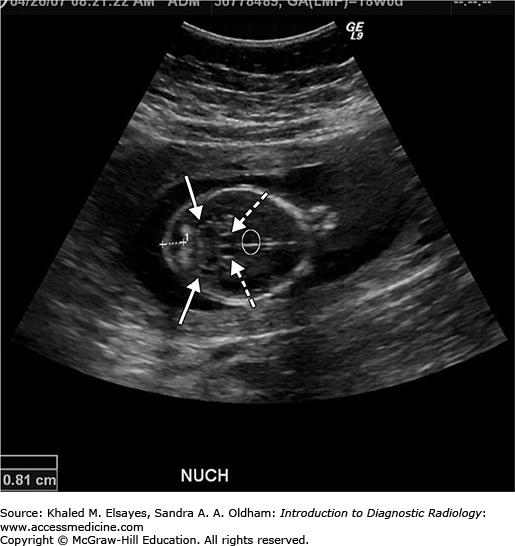
Fig. C7.2
Axial gray-scale ultrasound image of fetal head during the 18th week of gestation, taken at the level of the cavum septum pellucidum (circle), thalami (dashed arrows), and cerebellar hemispheres (arrows) showing thickened nuchal fold measuring 8 mm between the outer aspect of the occipital bone and outer edge of skin as marked by calipers. This fetus was found to have Down syndrome.
Most thickened nuchal folds tend to resolve toward the third trimester. However, this doesn’t reduce the increased risk for aneuploidy. In fact, a thickened nuchal fold is considered the most sensitive and specific second trimester finding of Down syndrome with a false positive rate as low as 1%.
K, Papageorghiou
A, Bindra
R,
et al. Prospective first trimester screening for trisomy 21 in 30,564 pregnancies. Am J Obstet Gynecol. 2005;192(6):1761-–1767.
[PubMed: 15970804]
AP, Von Kaisenberg
CS, Hyett
JA,
et al. Increased nuchal translucency with normal karyotype. Am J Obstet Gynecol. 2005;192(4):1005-–1021.
[PubMed: 15846173]
KH. Nuchal translucency and other first-trimester sonographic markers of chromosomal abnormalities. Am J Obstet Gynecol. 2004;191(1):45-–67.
[PubMed: 15295343]
A, Piccoli
MG, Vergani
P,
et al. Critical appraisal of the use of nuchal fold thickness measurements for the prediction of Down syndrome. Am J Obstet Gynecol. 2000;182(1 Pt 1):192-–197.
[PubMed: 10649178]
CASE 8: OMPHALOCELE
A 20-year-old woman who is 18 weeks pregnant presents for routine screening. The ultrasonographer recognizes abdominal contents herniating within a membranous sac.
Omphalocele
Transabdominal pelvic ultrasound. Advantages: readily available, low cost, sensitive, no ionizing radiation.
Ultrasound findings for omphalocele:
-
Omphalocele: Midline defect in which extruded abdominal contents, mainly liver, persist beyond 12 weeks of gestation (Fig. 8.1).
-
Omphalocele is contained by a sac; small bowel and liver are usually within the herniated sac. Umbilical cord inserts in the center of the sac.
-
Size of abdominal wall defect is important:
-
< 5 cm: Minor or small; chromosomal abnormalities more likely
-
5 cm: Large; usually contains liver; higher rate of cardiac, renal, pulmonary anomalies
-
-
Bowel malrotation is frequent.
Physiologic midgut herniation is a normal phenomenon before 12 weeks of gestation that allows for normal physiologic bowel rotation, so omphalocele should never be diagnosed until the gestational age is more than 12. Physiologic rotation, though, doesn’t include liver, and if liver herniating through a midline defect before 12 weeks of gestation is encountered, wrong dating should be suspected as this is highly specific for omphalocele. Isolated omphalocele survival rate is 75% to 95%, and most cases are sporadic. The high mortality is mainly due to increased association with chromosomal abnormalities, mainly trisomy 13, 18, and 21, which lead to a poor prognosis. Omphaloceles are also associated with intestinal atresia, tracheoesophageal fistula, bowel malrotation, pulmonary hypoplasia, and congenital heart disease. Not infrequently, omphaloceles can be complicated by rupture, which is associated with very poor prognosis. Polyhydramnios is common with omphaloceles, and amniocentesis for karyotyping should always be performed when diagnosis is made.
Treatment for omphalocele:
-
C-section for giant omphalocele, otherwise vaginal delivery
-
Sac should be covered to prevent fluid loss and to prevent rupture
-
Urgent repair is not indicated unless sac ruptures
-
Gastroschisis: Gastroschisis refers to herniation of fetal bowel loops into the amniotic cavity through a right paraumbilical abdominal wall defect. This anomaly doesn’t have a membrane covering the hernia, and the abdominal wall defect is anterior on the right side of the umbilical cord insertion (Fig. C8.2). Extruded contents include only bowel and stomach, but not liver as seen with omphaloceles. Gastroschisis on the contrary to omphalocele is not associated with chromosomal abnormalities and has a better prognosis. The only associated abnormalities with gastroschises are bowel related such as malrotation and intestinal atresia.
-
Umbilical hernia: Small skin-covered midline anterior wall defect. May contain bowel.
-
Bladder exstrophy: Lower anterior wall defect with bladder involvement.
Fig. C8.2
(A) Ultrasound of a midtrimester 18 weeks fetus showing bowel extruded (dashed arrows) to the right of the umbilical cord insertion (arrow). No membrane is covering herniated bowel. Appearance is consistent with gastroschisis. (B) Color Doppler ultrasound image confirms umbilical cord insertion (arrow) with herniated bowel to its right.
S, Zimmer
EZ, Gover
A,
et al. Fetal omphalocele detected early in pregnancy: associated anomalies and outcomes. Radiology. 2004;232(1):191-–195.
[PubMed: 15220502]
PJ, Kousseff
BG. Omphalocele and gastroschisis: an 18-year review study. Genet Med. 2004;6(4):232-–236.
[PubMed: 15266212]
RD, Johnson
MP. Congenital abdominal wall defects: an update. Fetal Diagn Ther. 2004;19(5):385-–398.
[PubMed: 15305094]
CASE 9: COMPLETE SEPTATE UTERUS
A 26-year-old woman presents with recurrent first trimester pregnancy loss.
Uterine anomaly leading to infertility
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


