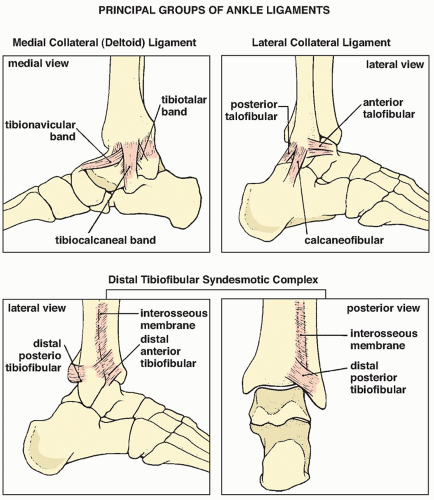
 FIGURE 10.1 Ligaments of the ankle. Three principal sets of ligaments form the ankle joint: the medial collateral (deltoid) ligament, the lateral collateral ligament, and the distal tibiofibular syndesmotic complex, which is important for maintaining ankle integrity and stability. |
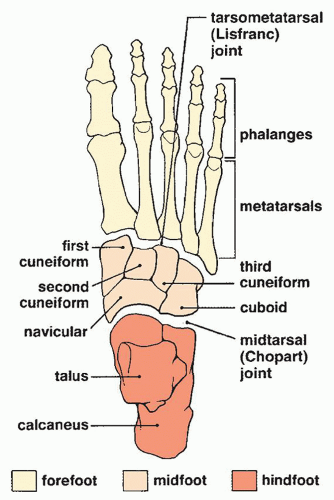 FIGURE 10.2 Anatomic divisions of the foot. The foot can be viewed as comprising three anatomic parts: the hindfoot, midfoot, and forefoot, separated respectively by the midtarsal (Chopart) and tarsometatarsal (Lisfranc) joints. |
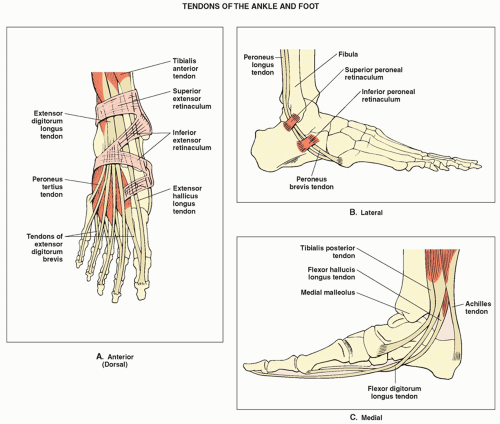 FIGURE 10.3 Tendons of the ankle and foot. The attachment of various tendons of the ankle and foot are depicted, as viewed from the dorsal aspect (A), lateral aspect (B), and medial aspect (C). |
so-called Maisonneuve fracture (see later), indicates rupture of the interosseous membrane up to the level of the fibular fracture.
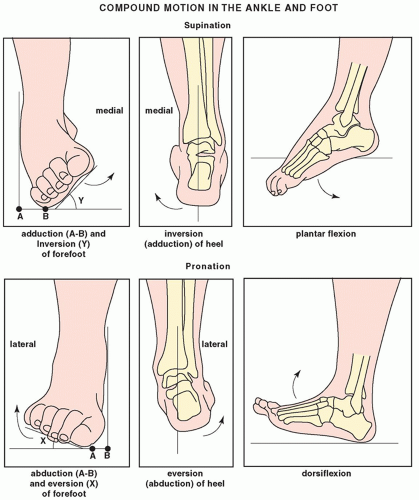 FIGURE 10.4 Motion in the ankle and foot. Supination is a compound motion consisting of adduction and inversion of the forefoot, together with inversion of the heel and slight plantar flexion in the ankle joint. In pronation, the compound motion involves abduction and eversion of the forefoot with eversion of the heel and slight dorsiflexion in the ankle joint. |
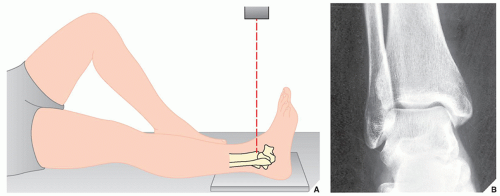 FIGURE 10.5 Anteroposterior view. (A) For the anteroposterior view of the ankle, the patient is supine on the radiographic table with the heel resting on the film cassette. The foot is in neutral position, with the sole perpendicular to the leg and the cassette. The central beam (red broken line) is directed vertically to the ankle joint at the midpoint between both malleoli. (B) The radiograph in this projection demonstrates the distal tibia, particularly the medial malleolus, the body of the talus, and the tibiotalar joint. Note, however, the overlap of the distal fibula and the lateral aspect of the tibia. The tibiofibular syndesmosis is not clearly demonstrated. |
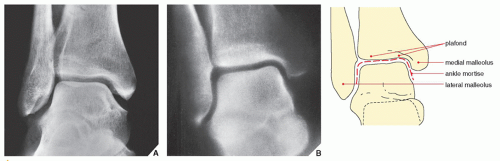 FIGURE 10.6 Mortise view. (A) The mortise view, a variant of the anteroposterior projection obtained with 10-degree internal rotation of the ankle, eliminates the overlap of the medial aspect of the distal fibula and the lateral aspect of the talus, so the space between these bones is well demonstrated. (B) The ankle mortise, shown here on a tomographic cut through the ankle joint, is formed by the medial malleolus, the articular surface of the distal tibia (the ceiling or plafond), and the lateral malleolus; it is shaped like an inverted U. |
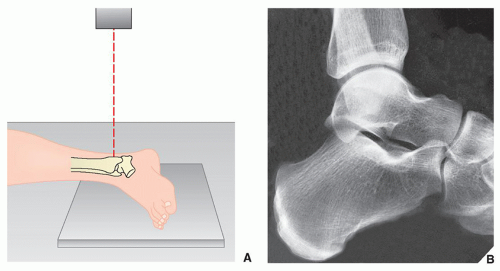 FIGURE 10.7 Lateral view. (A) For the lateral projection of the ankle, the patient is placed on his or her side with the fibula resting on the film cassette and the foot in the neutral position. The central beam is directed vertically to the medial malleolus. (The lateral view can also be obtained by placing the medial side of the ankle against the cassette.) (B) On the radiograph obtained in this projection, the distal tibia, talus, and calcaneus are seen in profile, and the fibula overlaps the posterior aspect of the tibia and the posterior aspect of the talus. The tibiotalar and subtalar joints are well demonstrated. Note the posterior lip of the tibia, also known as the third malleolus. |
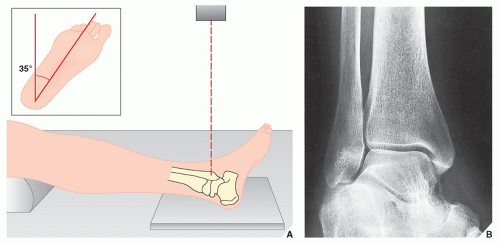 FIGURE 10.8 Internal oblique view. (A) For the internal oblique view of the ankle, the patient is supine, and the leg and foot are rotated medially approximately 35 degrees (inset). The foot is in the neutral position, forming a 90-degree angle with the distal leg. The central beam is directed perpendicular to the lateral malleolus. (B) On the radiograph, the medial and lateral malleoli, the tibial plafond, the dome of the talus, the tibiotalar joint, and the tibiofibular syndesmosis are well demonstrated. |
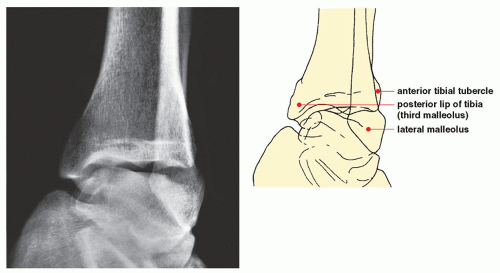 FIGURE 10.9 External oblique view. On the external oblique view, for which the patient is positioned as for the internal oblique view but with the limb rotated laterally approximately 40 to 45 degrees, the lateral malleolus and the anterior tibial tubercle are well demonstrated. |
5 to 15 degrees may be normal or abnormal, 15 to 25 degrees strongly suggests ligament injury, and more than 25 degrees is always abnormal. With forced eversion, talar tilting of more than 10 degrees is probably pathologic.
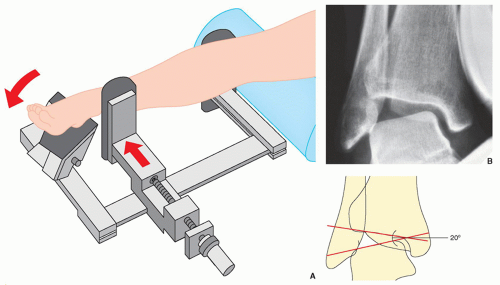 FIGURE 10.10 Inversion stress view. (A) For inversion (adduction)-stress examination of the ankle, the foot is fixed in the device while the patient is supine. The pressure plate, positioned approximately 2 cm above the ankle joint, applies varus stress (red arrows) adducting the heel. (If the examination is painful, 5 to 10 mL of 1% lidocaine or a similar local anesthetic is injected at the site of maximum pain.) (B) On the anteroposterior radiograph, the degree of talar tilt is measured by the angle formed by lines drawn along the tibial plafond and the dome of the talus. The contralateral ankle is subjected to the same procedure for comparison. |
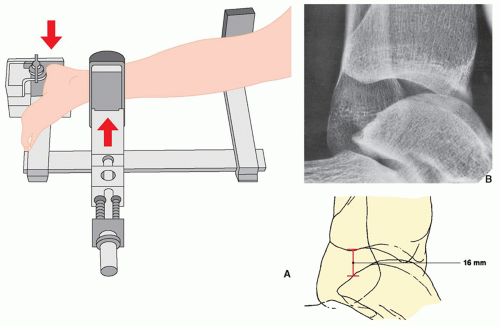 FIGURE 10.11 Anterior-draw stress view. (A) For anterior-draw stress examination, the patient is placed on his or her side, with the foot in the device. The pressure plate, positioned anteriorly approximately 2 cm above the ankle, applies posterior stress (red arrows) on the heel. During the examination, the amount of pressure is monitored on a light-emitting diode digital reader. (B) On the lateral stress film, the amount of transposition of the talus in relation to the distal tibia can be determined. |
of various tendons seen on axial MR image of the ankle by using the mnemonic phrase, “Tom, Dick, and Harry” for the posteromedial aspect, and “TED” for the anterolateral aspect of the ankle (Fig. 10.15). The ankle ligaments, likewise, demonstrate low signal intensity on MR images, with the exception of the posterior talofibular ligaments, which often appears inhomogeneous, similar to the anterior cruciate ligament of the knee. The anterior and posterior talofibular ligaments can be visualized over their entire length on axial scans with the foot in neutral position (Fig. 10.16) because they are approximately in the same plane of section. The calcaneofibular ligament can be similarly visualized when the foot is in 40-degree plantar flexion. The anterior and posterior tibiofibular ligaments can be demonstrated on the axial images in more proximal sections (Fig. 10.17).
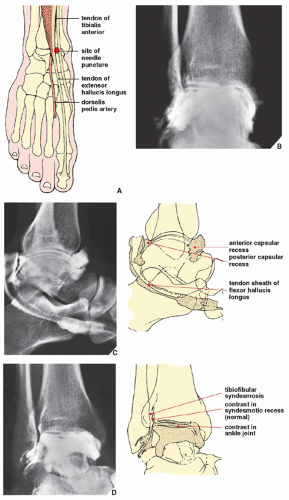 FIGURE 10.12 Arthrography of the ankle joint. (A) For arthrographic examination of the ankle, the patient is supine on the table, with the foot in the neutral position (see Fig. 10.5A). Under fluoroscopic control, the injection site between the tendons of the tibialis anterior and the extensor hallucis longus is marked. Care should be taken to avoid puncturing the dorsalis pedis artery, which should be located by palpation and its site marked on the skin. The needle (preferably 21-gauge) is directed slightly cephalad to avoid the overhanging anterior margin of the tibia. After the joint is entered, approximately 5 to 7 mL of 60% meglumine diatrizoate or a similar contrast agent is injected for a single-contrast arthrogram. For a double-contrast study, 1 to 2 mL of positive contrast agent and 6 to 8 mL of room air are injected. Films are then obtained in the standard anteroposterior, lateral, and oblique projections. (B) The normal anteroposterior radiograph shows contrast agent outlining the ankle joint, coating the articular surface of the talus and extending into the syndesmotic recess, which normally should not exceed 2.5 cm. (C) On the lateral radiograph, the anterior and posterior capsular recesses are outlined. Filling of the posterior facet of the subtalar joint represents a normal variant, occurring in approximately 10% of cases (see Fig. 10.69C). In approximately 20% of cases, the tendon sheaths of the flexor hallucis longus and flexor digitorum longus opacify on the medial aspect of the ankle. When this occurs, the full extension of the flexor hallucis longus should be noted as it passes proximal to the groove in the talar tubercle and into the groove beneath the sustentaculum tali. Under normal conditions, no tendon sheath opacification should occur on the lateral side of the ankle. (D) Oblique radiograph demonstrates the tibiofibular syndesmosis. No contrast agent should be seen in this area except for normal opacification of the syndesmotic recess. |
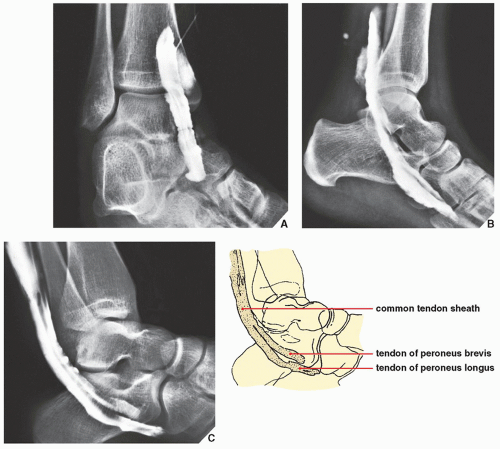 FIGURE 10.13 Ankle tenography. Tenograms in the oblique (A) and lateral (B) projections demonstrate the normal appearance of the tendon of the flexor hallucis longus. On the oblique radiograph, note the distal direction of the needle tip at the beginning of the injection. Normally, the tendon of the flexor hallucis longus does not opacify beyond the limit of the Lisfranc joint. (C) On the normal tenogram of the peroneus longus and brevis, seen here on the lateral radiograph, note the position of these tendons below the flexor hallucis longus. The tendon of the peroneus brevis is seen normally opacified; the tendon of the peroneus longus passes below it, crossing into the plantar aspect of the foot to its insertion at the base of the first metatarsal bone. |
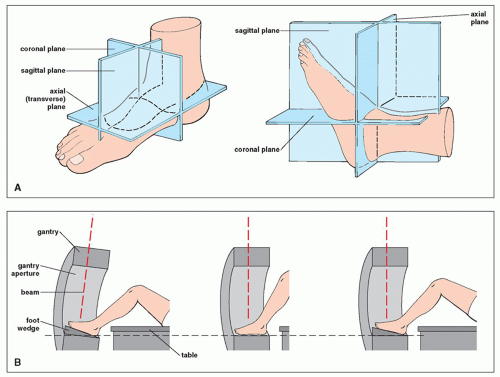 FIGURE 10.14 Anatomic and imaging planes. (A) Anatomic planes of the ankle and foot and (B) CT imaging planes. (B, Modified from Berquist TH, ed. Radiology of the foot and ankle. New York: Raven Press; 1989.) |
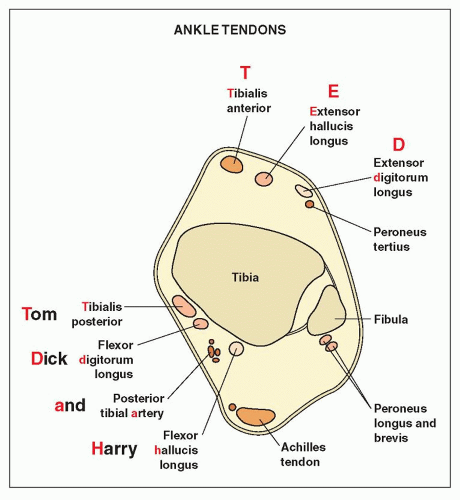 FIGURE 10.15 Schematic representation of ankle tendons on axial MRI. (Modified from Helms CA, Major NM, Anderson MW, et al. Musculoskeletal MRI, 2nd ed. Philadelphia: Saunders/Elsevier; 2009:384-429.) |
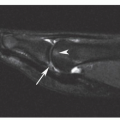
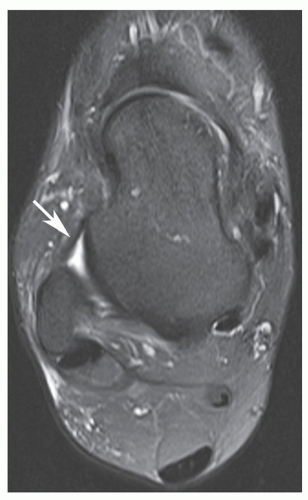 FIGURE 10.16 MRI of the anterior talofibular ligament. Axial T2-weighted MR image through the lateral malleolus and talus demonstrates normal anterior talofibular ligament (arrow). |
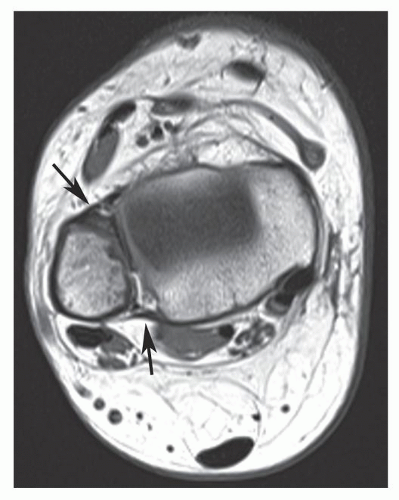 FIGURE 10.17 MRI of the anterior and posterior tibiofibular ligaments. Axial T1-weighted MR image shows normal anterior and posterior tibiofibular ligaments (arrows). |
section (Fig. 10.19). The coronal plane is also effective in the visualization of various ligaments and tendons (Fig. 10.20).
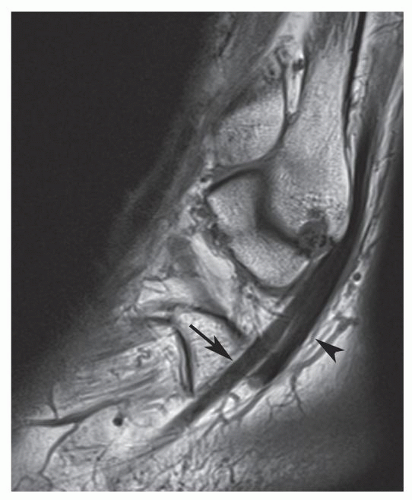 FIGURE 10.18 MRI of the peroneus longus tendon. Sagittal T1-weighted MR image through lateral malleolus shows normal appearance of peroneus brevis (arrow) and longus (arrowhead) tendons as they curve around the lateral malleolus. |
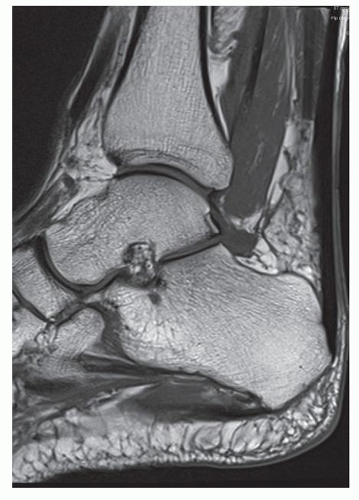 FIGURE 10.19 MRI of the Achilles tendon. Midline sagittal T1-weighted MR image demonstrates normal Achilles tendon. Note the uniformly low signal intensity of the tendon contrasting with the high signal intensity of the anterior fat pad. |
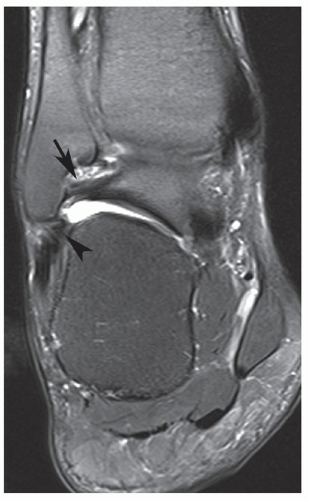 FIGURE 10.20 MRI of the posterior talofibular and calcaneofibular ligaments. Coronal T2-weighted MR image of the ankle shows normal posterior talofibular (arrow) and calcaneofibular (arrowhead) ligaments. |
subtalar joint occasionally require special, tangential projections such as the posterior tangential (Harris-Beath) view (Fig. 10.25) or oblique tangential (Broden) view (Fig. 10.26). A tangential view of the sesamoid bones of the great toe (Fig. 10.27) may also be necessary.
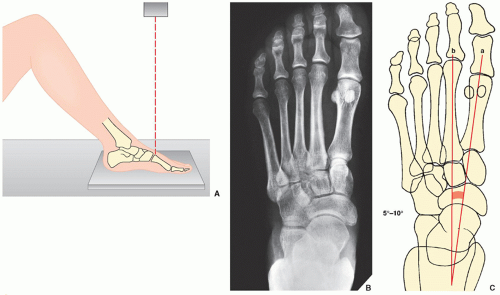 FIGURE 10.21 Anteroposterior view. (A) For the anteroposterior (dorsoplantar) view of the foot, the patient is supine, with the knee flexed and the sole placed firmly on the film cassette. The central beam is directed vertically to the base of the first metatarsal bone. (B) On the radiograph obtained in this projection, injury to the metatarsal bones and phalanges can be adequately assessed. Note that 75% of the talar head articulates with the navicular bone. (For identification of the bones of the foot, see Fig. 10.2.) (C) The first intermetatarsal angle is formed by the intersection of the lines bisecting the shafts of the first (a) and second (b) metatarsals. |
Unimalleolar, when the fracture involves the medial (tibial) or lateral (fibular) malleolus (Figs. 10.33 and 10.34)
Bimalleolar, when both malleoli are fractured (Fig. 10.35)
Trimalleolar, when fractures involve the medial and lateral malleoli as well as the posterior lip (or tubercle) of the distal tibia (the third malleolus) (Fig. 10.36)
Complex fractures, known also as pilon fractures, when comminuted fractures of the distal tibia and fibula occur (Fig. 10.37)
Fractures/dislocations (Figs. 10.38 and 10.39).
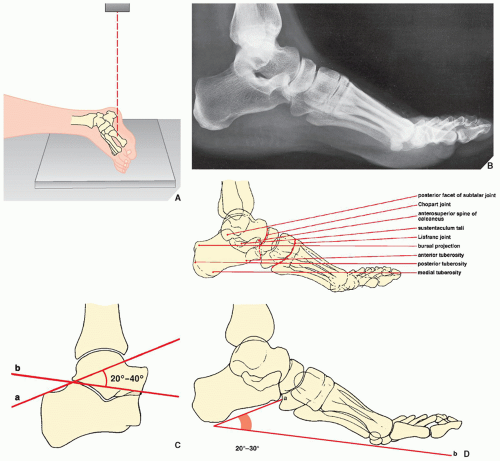 FIGURE 10.22 Lateral view. (A) For the lateral view of the foot, the patient lies on his or her side with the knee slightly flexed and the lateral aspect of the foot against the film cassette. The central beam is directed vertically to the midtarsus. (B) The lateral radiograph demonstrates the bursal projection, the most prominent feature on the posterior aspect of the calcaneus; the posterior tuberosity where the Achilles tendon inserts; the medial tuberosity on the plantar surface where the plantar fascia inserts; the anterior tuberosity; the anterosuperior spine of the calcaneus; the posterior facet of the subtalar joint; the sustentaculum tali; and the talonavicular and calcaneocuboid articulations. The Chopart and Lisfranc joints are also well visualized. (C) The lateral view also allows evaluation of the angular relationship between the talus and the calcaneus—Boehler angle. This feature is determined by the intersection of a line (a) drawn from the posterosuperior margin of the calcaneal tuberosity (bursal projection) through the tip of the posterior facet of the subtalar joint, and a second line (b) drawn from the tip of the posterior facet through the superior margin of the anterior process of the calcaneus. Normally, this angle ranges between 20 and 40 degrees. (D) Calcaneal pitch is described by the intersection of a line drawn tangentially to the inferior surface of the calcaneus and one drawn along the plantar surface of the foot. |
 FIGURE 10.23 The angle of Gissane. This measurement is obtained on the lateral radiograph of the hindfoot. The angle is formed by intersection of the lines drawn along the downward and upward slopes of the calcaneal dorsal surfaces, with normal values between 125 and 140 degrees. |
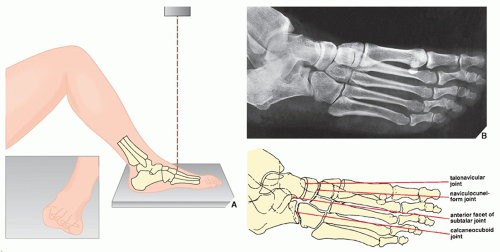 FIGURE 10.24 Oblique view. (A) For the oblique view of the foot, the patient is supine on the table with the knee flexed. The lateral border of the foot is elevated about 40 to 45 degrees (inset) so that the medial border of the foot is forced against the film cassette. The central beam is directed vertically to the base of the third metatarsal. (B) On the oblique radiograph of the foot, the phalanges and metatarsals are well demonstrated, as are the anterior part of the subtalar joint and the talonavicular, naviculocuneiform, and calcaneocuboid joints. |
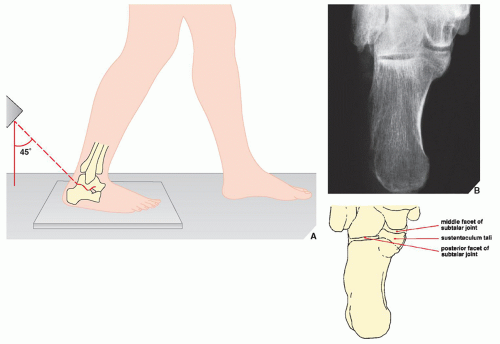 FIGURE 10.25 Harris-Beath view. (A) For the posterior tangential (Harris-Beath) view of the foot, the patient is erect, with the sole of the foot flat on the film cassette. The central beam is usually angled 45 degrees toward the midline of the heel, but 35 or 55 degrees of angulation may also be used. (B) On the radiograph in this projection, the middle facet of the subtalar joint is seen, oriented horizontally; the sustentaculum tali projects medially. The posterior facet projects laterally and is parallel to the middle facet. The body of the calcaneus is well demonstrated. |
 FIGURE 10.26 Broden view. (A) For the Broden view of the foot, the patient is supine, with the knee slightly flexed and supported by a small sandbag. The foot rests on the film cassette, dorsiflexed to 90 degrees, and, together with the leg, rotated medially approximately 45 degrees (inset). The central beam is directed toward the lateral malleolus. Films may be obtained at 10, 20, 30, and 40 degrees of cephalad angulation of the tube. (B) A radiograph obtained at 30-degree cephalad angulation demonstrates the posterior facet of the subtalar joint. Note also the good demonstration of the sustentaculum tali and the excellent visualization of the talofibular joint and the tibiofibular syndesmosis. |
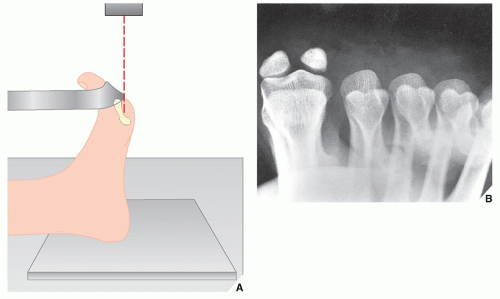 FIGURE 10.27 Tangential view. (A) For a tangential view of the sesamoid bones, the patient is seated on the table, with the foot dorsiflexed on the cassette, holding the toes in a dorsiflexed position with a strip of gauze. The central beam is directed vertically to the head of the first metatarsal bone. (B) This sesamoid view demonstrates the metatarsal heads and the sesamoid bones of the first metatarsal. |
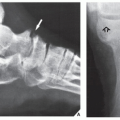
 FIGURE 10.28 Accessory ossicles. (A,B) The numerous accessory ossicles of the foot and ankle can complicate the evaluation of foot injuries by mimicking fracture. Fractures, however, may go undetected when misinterpreted as ossicles, as seen here on the anteroposterior (C) and sesamoid (D) views of the foot, which demonstrate a fracture of the lateral (fibular) sesamoid (arrows) (compare with Fig. 10.27B). |
TABLE 10.1 Checklist for Evaluation of Magnetic Resonance Imaging of the Foot and Ankle | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 10.2 Standard and Special Radiographic Projections for Evaluating Injury to the Ankle and Foot | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 10.3 Ancillary Imaging Techniques for Evaluating Injury to the Ankle and Foot | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
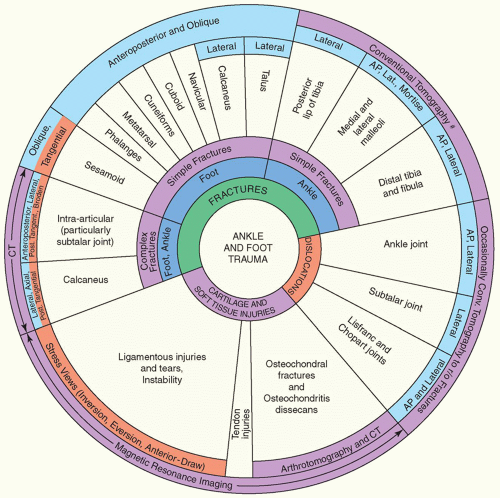 FIGURE 10.29 Spectrum of radiologic imaging techniques used to evaluate trauma to the ankle and foot. The radiographic projections or radiologic techniques indicated throughout the diagram are only those that are the most effective in demonstrating the respective traumatic conditions. #Replaced almost completely by CT. AP, anteroposterior; Lat., lateral; CT, computed tomography; Conv., conventional; r/o, rule out. |
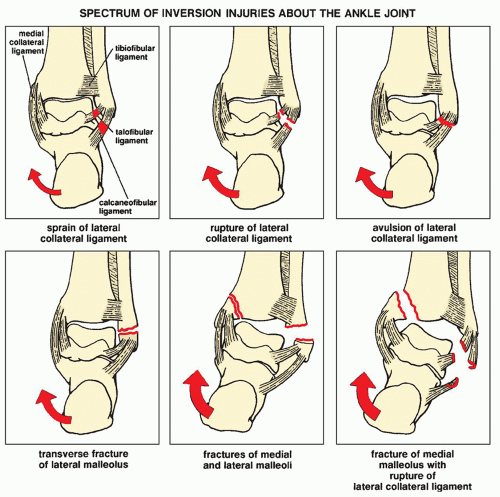 FIGURE 10.30 Inversion injuries. Depending on its severity, an inversion force (red arrows) delivered to the lateral structures of the ankle joint may manifest in a broad spectrum of injuries of the lateral collateral ligament complex as well as the lateral and medial malleoli. Note, however, that inversion-stress forces do not affect the posterior tibiofibular or medial collateral ligaments. (Modified from Edeiken J, Cotler JM. Ankle trauma. Semin Roentgenol 1978;13: 145-155.) |
 FIGURE 10.31 Eversion injuries. Depending on its severity, an eversion force delivered to the medial structures of the ankle joint may manifest in a broad spectrum of injuries of the medial collateral (deltoid) ligament complex as well as the medial and lateral malleoli. Note, however, that eversion-stress forces do not affect the posterior tibiofibular or lateral collateral ligaments. (Modified from Edeiken J, Cotler JM. Ankle trauma. Semin Roentgenol 1978;13:145-155.) |
 FIGURE 10.32 Classification of ankle fractures. Ankle fractures can be classified according to the anatomic structure as unimalleolar, bimalleolar, trimalleolar, or complex. |
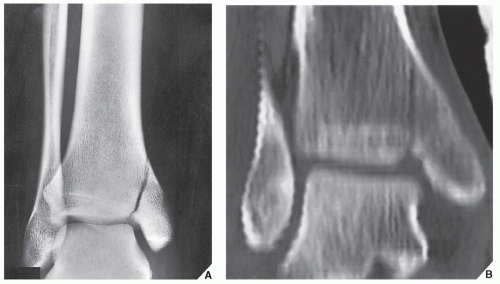 FIGURE 10.33 Unimalleolar fracture. Anteroposterior radiograph of the ankle (A) and coronal CT reformatted image (B) demonstrate the typical appearance of a unimalleolar fracture involving the medial malleolus. |
 FIGURE 10.34 Unimalleolar fracture. Anteroposterior radiograph of the left ankle shows a transverse fracture of the lateral malleolus. |
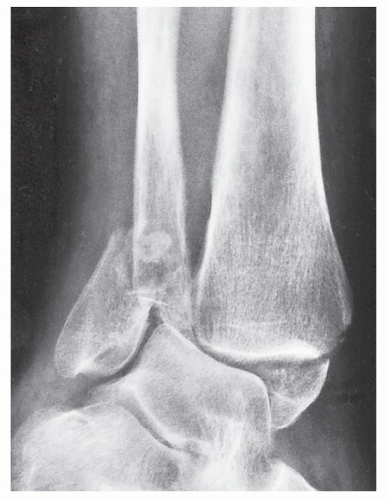 FIGURE 10.35 Bimalleolar fracture. Oblique radiograph of the ankle shows a bimalleolar fracture involving the tibial and fibular malleoli. |
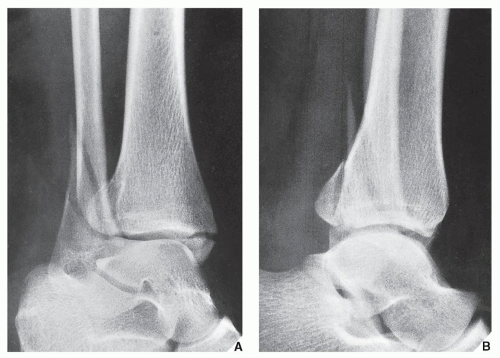 FIGURE 10.36 Trimalleolar fracture. Oblique (A) and lateral (B) radiographs of the ankle show a trimalleolar fracture affecting both malleoli and the posterior lip of the distal tibia. The latter feature is better seen on the lateral projection. |
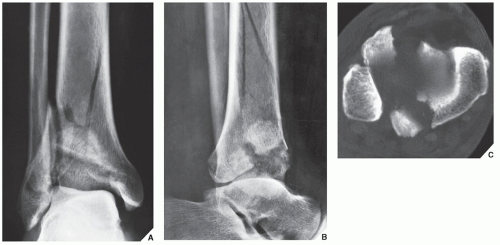 FIGURE 10.37 Pilon fracture. Anteroposterior (A) and lateral (B) radiographs of the ankle demonstrate a complex, comminuted fracture of the distal tibia and fibula in a 30-year-old man who fell from a third-floor window. (C) Axial CT section through the tibial plafond shows typical appearance of pilon fracture. |
 FIGURE 10.38 Fracture/dislocation of the ankle. A 28-year-old woman injured her right ankle in a skiing accident. Note comminuted fractures of the distal fibula and medial malleolus associated with posterior dislocation in the ankle joint. |
 FIGURE 10.39 3D CT of fracture/dislocation of the ankle. (A) Anteroposterior and (B) cross-table lateral radiographs of the left ankle show trimalleolar fracture associated with posterior dislocation in the ankle joint. (C) Coronal reformatted and (D) 3D reconstructed CT images were obtained after the dislocation was relocated. |
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Anomalies of the Upper and Lower Limbs
Anomalies of the Upper and Lower Limbs
 Radiologic Evaluation of Trauma
Radiologic Evaluation of Trauma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


