TABLE 15.1 Clinical and Imaging Hallmarks of Connective Tissue Arthritides (Arthropathies) | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
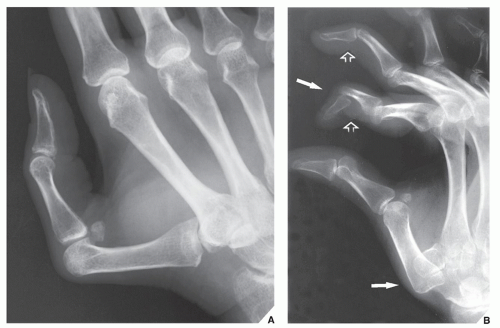 FIGURE 15.1 Systemic lupus erythematosus. (A) Typical appearance of the thumb in a 43-year-old woman with SLE. Note subluxations in the first carpometacarpal and metacarpophalangeal joints without articular erosions. (B) In another patient, a 32-year-old woman, the oblique radiograph of her left hand shows dislocations at the first carpometacarpal joint and distal interphalangeal joint of the index finger (arrows), and subluxations in the metacarpophalangeal joints of the index and middle fingers associated with swan-neck deformities (open arrows). |
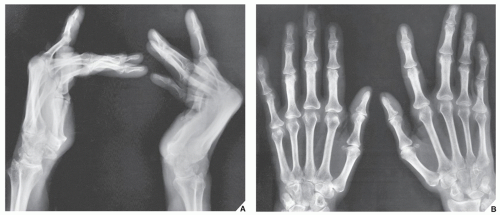 FIGURE 15.2 Systemic lupus erythematosus. (A) Lateral radiograph of both hands of a 42-year-old woman with documented SLE for the past 4 years demonstrates flexion deformities in the metacarpophalangeal joints. On the dorsovolar projection (B), the flexion deformities have been corrected by the pressure of the hands against the radiographic cassette. |
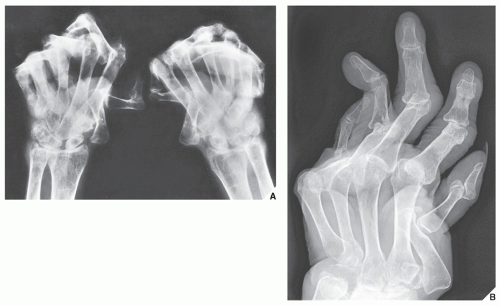 FIGURE 15.3 Systemic lupus erythematosus. (A) 62-year-old woman presented with a 15-year history of SLE. Dorsovolar view of both hands shows severe deformities, subluxations, and articular erosions. Note the advanced osteoporosis secondary to disuse of the extremities and treatment with corticosteroids. (B) In another patient, a 51-year-old woman, note flexion contractions, subluxations, and dislocations in the several joints of the right hand. |
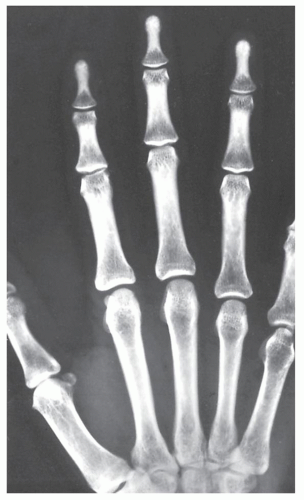 FIGURE 15.4 Systemic lupus erythematosus. Dorsovolar film of the hand of a 29-year-old woman with SLE demonstrates sclerosis of the distal phalanges (acral sclerosis). Similar sclerotic changes are also occasionally seen in rheumatoid arthritis and scleroderma. |
and dermatomyositis because the two tests provide a broader perspective than either test alone.
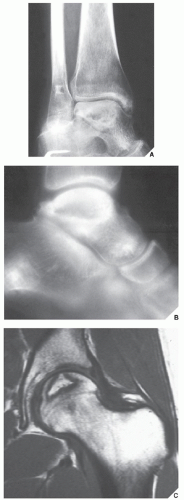 FIGURE 15.5 SLE complicated by osteonecrosis. Oblique radiograph (A) and lateral tomogram (B) of the ankle demonstrate osteonecrosis of the talus in a 26-year-old woman with lupus who was treated with massive doses of steroids. (C) Coronal T2-weighted MRI in an 18-year-old woman with SLE demonstrates a focal area of osteonecrosis of the femoral head. |
 FIGURE 15.6 Scleroderma. A 24-year-old woman presented with atrophy of the soft tissues at the distal phalanges of the index, middle, and ring fingers (arrows). |
 FIGURE 15.7 Scleroderma. A 32-year-old woman with progressive systemic sclerosis exhibits soft-tissue calcifications in the distal phalanges of the right hand (arrows), a typical feature of this disorder. |
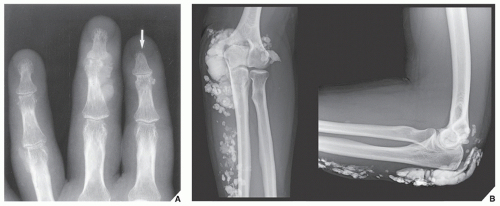 FIGURE 15.8 Scleroderma. (A) Dorsovolar radiograph of the fingers of a 44-year-old woman reveals acroosteolysis (arrow), soft-tissue calcifications, and destructive changes of the distal interphalangeal joint of the middle finger. (B) In another patient, a 46-year-old woman, extensive soft-tissue calcifications are present around the elbow and the forearm. |
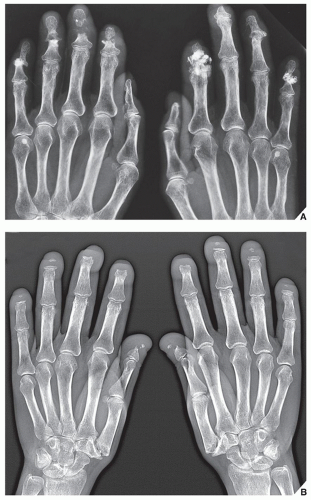 FIGURE 15.9 Scleroderma. (A) Dorsovolar radiograph of the hands of a 50-year-old man with documented systemic sclerosis shows destructive changes in the distal interphalangeal joints as well as soft-tissue calcifications and resorption of the tip of the distal phalanx of the left middle finger. (B) Dorsovolar radiograph of the hands of a 53-year-old woman with longstanding systemic sclerosis shows acroosteolysis of all distal phalanges. Note also erosions of the first carpometacarpal joints. |
phenomenon, polyarthralgia, swelling of the hands, esophageal hypomotility, inflammatory myopathy, and pulmonary disease. Women constitute approximately 80% of affected patients. Patients with MCTD have prominent joint abnormalities, with typical involvement of the small articulations of the hand, wrist, and foot; large joints such as the knee, elbow, and shoulder may also be affected. The joint deformities mimic those seen in rheumatoid arthritis but occasionally joint subluxation may be nonerosive, as in SLE. Soft-tissue abnormalities are identical to those encountered in scleroderma (Figs. 15.12, 15.13, 15.14).
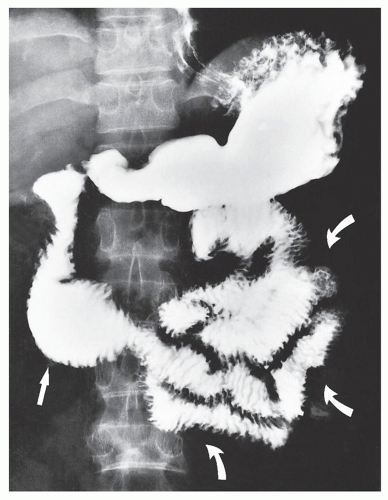 FIGURE 15.10 Scleroderma. Upper gastrointestinal series and small bowel study in the patient shown in Figure 15.9A demonstrate dilatation of the second and third portions of the duodenum (arrow) and jejunum (curved arrows), with a pseudoobstruction pattern. |
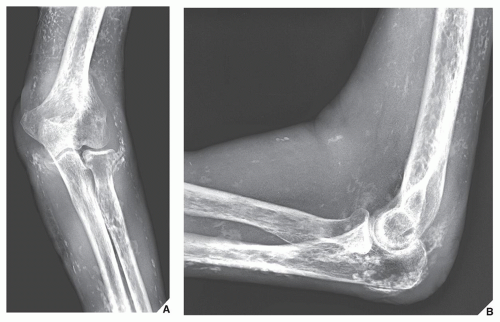 FIGURE 15.11 Dermatomyositis. (A) External oblique and (B) lateral radiographs of the left elbow of a 64-year-old woman show extensive soft-tissue calcifications, characteristic for this disorder. Note also prominent periarticular osteoporosis. |
 FIGURE 15.12 Mixed connective tissue disease. A 44-year-old woman presented with clinical and imaging features of rheumatoid arthritis. In addition, she had clinically documented dermatomyositis. A dorsovolar radiograph of her left hand shows extensive articular erosions at radiocarpal, metacarpophalangeal, and proximal interphalangeal joints, typical for rheumatoid arthritis. The muscle biopsy result was consistent with polymyositis. |
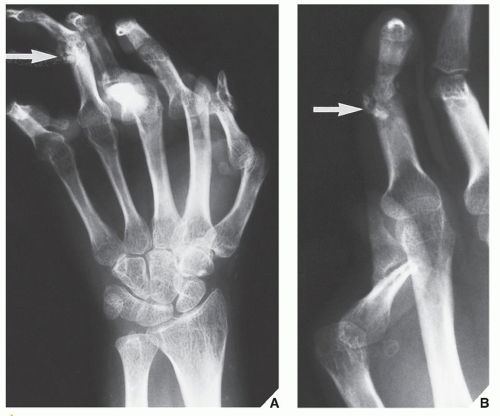 FIGURE 15.13 Mixed connective tissue disease. A 26-year-old woman presented with swelling of both hands, polyarthralgia, and Raynaud phenomenon. She tested positively for the rheumatoid factors and ANAs, and her clinical findings were characteristic for SLE and scleroderma. Oblique radiograph (A) of the right hand and coned-down view (B) of the thumb and index finger of the left hand show flexion deformities and subluxations in the multiple joints. Deformities of both thumbs are characteristic for SLE, whereas soft-tissue calcifications (arrows) are typical for scleroderma. The clinical diagnosis was MCTD. |
 FIGURE 15.14 Mixed connective tissue disease. Dorsovolar radiograph of the hands of a 55-year-old woman with documented long-standing rheumatoid arthritis, lupus erythematosus, and scleroderma shows erosive changes in both wrists, subluxations in the metacarpophalangeal joints, and soft-tissue calcifications. |
TABLE 15.2 Clinical and Imaging Hallmarks of Metabolic, Endocrine, and Miscellaneous Arthritides | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 FIGURE 15.15 Gouty arthritis. (A) Dorsovolar radiograph of the left hand of a 43-year-old man with tophaceous gout shows multiple sharply marginated articular and periarticular erosions and soft-tissue masses at the proximal interphalangeal joints of the index and middle fingers, representing tophi. (B) Dorsovolar radiograph of the fingers of a 70-year-old man with gouty arthritis shows multiple articular and periarticular erosions associated with large tophi (arrows). |
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


