Chapter 92 Hepatic neoplasms constitute approximately 2% of all childhood tumors and approximately 6% of pediatric abdominal neoplasms. Two thirds of liver tumors in children are malignant, and they represent the third most common intraabdominal malignancy in the pediatric age group after Wilms tumor and neuroblastoma. The most common hepatic malignant tumors in order of frequency are hepatoblastomas, hepatocellular carcinomas (HCC), undifferentiated embryonal sarcomas, angiosarcomas, and embryonal rhabdomyosarcomas.1 Benign hepatic tumors in pediatrics include tumors specific to children such as vascular tumors and mesenchymal hamartomas, as well as entities that also are seen in adults, such as focal nodular hyperplasia (FNH), hepatocellular adenoma, and nodular regenerative hyperplasia (NRH). A differential diagnosis of liver tumors can be obtained based on the age of the patient, laboratory findings such as serum alpha fetoprotein (AFP) levels, and imaging characteristics (Table 92-1). However, the serum AFP level is normally elevated at birth (25,000-50,000 ng/mL) and does not reach adult levels (<25 ng/mL) until 6 months of age.2,3 Table 92-1 Summary for Differential Diagnosis of Liver Tumor AFP, Alpha fetoprotein; CT, computed tomography; MRI, magnetic resonance imaging. Overview: Hepatoblastoma is the most common primary malignant liver tumor in infants and children. Sixty-eight percent of cases are seen in the first year of life, and 90% occur in patients younger than 5 years, with a male predominance of 2 : 1.3 Four percent of cases are congenital.1,3–6 Etiology: Predisposing conditions include Beckwith-Wiedemann syndrome, familial adenomatous polyposis, type 1A glycogen storage disease, Gardner syndrome, fetal alcohol syndrome, Wilms tumor, and trisomy 18. It also is reported in premature infants, low-birth-weight infants, and in infants born of mothers taking oral contraceptives. A strong association exists between low birth weight and hepatoblastoma, raising the issue of potential contribution by a variety of iatrogenic exposures in the neonatal intensive care unit.7 Clinical Presentation: Hepatoblastoma usually presents as a palpable mass in the right upper quadrant and may be confused with hepatomegaly. Nonspecific clinical symptoms include pain, weight loss, irritability, vomiting, and infrequently, jaundice and precocious puberty (related to the secretion of chorionic gonadotropins). Distant metastases are present in fewer than 10% of cases at diagnosis, with the lungs being the most common site, followed by the lymph nodes, bone, brain, eye, and ovary. Compression or invasion of the hepatic vasculature and inferior vena cava may occur. Serum AFP, which is markedly elevated in approximately 90% of patients with hepatoblastoma, can be used to monitor therapy and detect recurrence. Hepatoblastoma is classified into two histologic types: the epithelial type, which represents the majority of these tumors, and the mixed epithelial mesenchymal type.1–3 Hepatoblastoma is usually solitary, but these tumors may be multifocal or, less commonly, diffusely infiltrating. Multifocal disease may consist of a dominant mass with satellite nodules or multiple small masses. When it is solitary, hepatoblastoma is most commonly located in the right hepatic lobe (60% of cases).8 Imaging: Plain radiographs may show hepatomegaly or a mass with or without calcifications. On sonography, hepatoblastomas are most often well-defined and hyperechoic relative to adjacent liver (Fig. 92-1 and e-Fig. 92-2). Epithelial-type hepatoblastomas are more homogeneous, whereas mixed tumors are more heterogeneous and often contain hyperechoic foci with acoustic shadowing indicating calcifications and hypoechoic or anechoic foci representing necrosis or hemorrhage.9–11 Intravascular tumor thrombus may be seen within the hepatic or portal veins. Flow within the thrombus on color Doppler imaging is useful to differentiate neoplastic from nonneoplastic thrombus. Infiltrative hepatoblastomas show diffuse heterogeneous echogenicity, with loss of normal parenchymal architecture.9–11 Figure 92-1 Hepatoblastoma. e-Figure 92-2 Hepatoblastoma. Unenhanced CT typically shows a well-circumscribed mass with decreased attenuation relative to the surrounding liver. Speckled or amorphous calcifications are seen in more than 50% of cases.9 On contrast-enhanced computed CT, the tumor enhances in a heterogeneous fashion and may be hyperdense compared with liver parenchyma in the early arterial postcontrast phase; it usually is isodense or hypodense on delayed images. Peripheral enhancement can be seen. CT angiography can help define vascular invasion when present and assess its potential to be resected. On MRI, epithelial-type hepatoblastomas are homogeneously hypointense on T1-weighted images and hyperintense on T2-weighted images relative to adjacent liver, and they enhance after intravenous (IV) administration of gadolinium contrast material.9 Mixed-type tumors show more heterogeneous signal intensity. However, areas of calcification, necrosis, hemorrhage, and septation may influence the signal intensity.9–11 Hemorrhage is most often hyperintense on T1-weighted images and bands of fibrosis or septation are hypointense on T1- and T2-weighted sequences.9 Vascular invasion is demonstrated with gradient-echo sequences; tumor thrombus appears as a high signal on T1-weighted images and as a signal void on gradient-echo images. On postgadolinium arterial and venous phase images, the tumor thrombus enhances and shows a filling defect, respectively. MR angiography is useful for preoperative evaluation of the relationship of the tumor to the hepatic vasculature. Hepatic scintigraphy currently is not performed in persons with a hepatoblastoma but may demonstrate increased activity on the initial angiographic phase as a result of tumor vascularity and photopenia on the delayed images. Rarely, increased uptake of the radiopharmaceutical agent may be seen on delayed images, which is a finding more typical of focal nodular hyperplasia. Currently, catheter angiography is rarely performed and usually shows tumor hypervascularity except in avascular areas of necrosis.9–11 Treatment: The treatment for hepatoblastoma is surgical resection. However, in about 40% to 60% of cases, the tumor cannot be resected at diagnosis.12 Initial treatment with chemotherapy permits up to 85% of these tumors to become resectable.3 The overall survival rate is reported to be 65% to 70%. 1,9–11 Imaging is crucial for assessment of the surgical resectability of hepatoblastomas at presentation and after the patient undergoes chemotherapy. Disseminated tumors have been treated successfully with chemotherapy and multiple resections of metastases. Radiofrequency ablation may be a promising treatment for recurrence.13 Liver transplantation can be useful in lesions that are considered unresectable; the presence of pulmonary metastases is not considered an absolute contraindication to liver transplantation because of their sensitivity to chemotherapy.9 Poor prognostic factors include AFP levels less than 100 ng/mL or more than 1,000,000 ng/mL, vascular invasion, and aneuploid nuclear content. Factors associated with favorable prognosis include single lobe involvement, pure fetal histologic composition, and AFP levels between 100 and 1,000,000 ng/mL.9 Overview: HCC, the second most common liver tumor in children after hepatoblastoma, accounts for 35% of primary pediatric hepatic malignancies.14 It affects two age peaks in childhood: 4 to 5 years and (more commonly) 12 to 14 years. HCCs, like hepatoblastoma, occur more often in the right than in the left lobe of the liver and demonstrate a high propensity for vascular invasion, which is seen in approximately 75% of cases. Neoplastic cells vary from very well-differentiated to poorly differentiated. The most helpful histologic feature in distinguishing HCC from metastases is the presence of bile canaliculi or bile pigment.1 Kupffer cells also may be present.9 Etiology: In nonendemic areas of the world, approximately half of HCCs arise in patients with underlying liver disease. Predisposing conditions include entities leading to cirrhosis, such as biliary atresia, infantile cholestasis, Alagille syndrome, hemochromatosis, hereditary tyrosinemia, glycogen storage disorder, α1-antitrypsin deficiency, Wilson disease, galactosemia, and viral hepatitis (hepatitis B and C). Clinical Presentation: The clinical symptoms and presentation are similar to those of hepatoblastoma, in that patients often present with an abdominal mass, abdominal pain, fever, and cachexia. The serum AFP level is markedly elevated in 70% of patients.14,15 Imaging: HCCs have three main growth patterns: solitary, multifocal, and diffuse/infiltrative.9 The ultrasound findings of HCC are variable. With respect to liver parenchyma, smaller lesions may be isoechoic or hyperechoic, although most tend to be hypoechoic9,10; larger lesions are heterogeneous. Internal areas of increased echogenicity may represent acute hemorrhage, fat, or calcifications (which is less common than in hepatoblastoma), whereas areas of decreased echogenicity may represent necrosis. If a capsule is present, it may be detected as a thin halo of decreased echogenicity. Doppler demonstrates high-velocity arterial flow and is useful for identifying vascular invasion by showing blood flow within the substance of tumoral thrombus.9 On unenhanced CT, an HCC appears as a solitary mass or as multiple well-defined or poorly defined, hypointense to isodense masses.10 The tumor shows variable enhancement after IV administration of contrast material and may contain low-attenuation regions of necrosis. The tumor capsule may also show a rim of low attenuation on unenhanced images that enhances on the delayed phase after injection of contrast material (Fig. 92-3).9 Vascular tumor thrombi may be seen as intraluminal filling defects with a surrounding meniscus of contrast and can be better evaluated with angiographic sequences. When the tumor arises in a cirrhotic liver, differentiation from regenerating nodules may be difficult. Figure 92-3 Hepatocellular carcinoma in a 14-year-old girl without underlying liver disease. With MRI, the tumor typically is slightly hyperintense on T2-weighted images and hypointense on T1-weighted images, although the latter presentation tends to be more variable; hyperintense areas of fat or hemorrhage may be seen on T1-weighted images. If a fibrous pseudocapsule is present, MRI shows low signal intensity on T1- and T2-weighted pulse sequences.16 After administration of gadolinium, in the early arterial phase, the lesion demonstrates enhancement and washes out with relatively low signal intensity during the portal venous phase. Vascular invasion appears as lack of a signal on spin-echo images and as an intravascular arterial enhancing mass with a delayed filling defect on dynamic gadolinium-enhanced images.17 Nuclear scintigraphy is rarely performed in patients with HCC and usually shows decreased uptake. Gallium scans, however, are characteristic and may help distinguish HCC, which is gallium-avid, from regenerating nodules, which are not gallium-avid. Fluorodeoxyglucose (FDG) positron emission tomography (PET) is useful in evaluating the degree of tumor differentiation. FDG uptake is variable in HCCs; uptake may be normal in well-differentiated tumors, with markedly elevated uptake usually seen in poorly differentiated tumors. FDG-PET may be useful in the staging of HCC or in distinguishing regenerating nodules in cirrhotic livers from HCC. Combining FDG-PET and gallium scintigraphy can be worthwhile when grading tumors.18 For example, low-grade tumors typically show normal uptake on PET and increased uptake on gallium scans. However, gallium uptake also is seen in other processes, such as metastatic disease (lymphoma) and hepatic adenoma. Treatment: The treatment for HCC is complete surgical resection when possible, but approximately two thirds of children present with unresectable tumors as a result of multifocal or massive involvement of the liver, major vascular involvement, or metastases. HCC is relatively insensitive to systemic chemotherapy.19 The impact of chemotherapy is unclear, with no evidence that it offers additional benefit in children with resectable localized HCC. Liver transplantation has been reported for an unresectable tumor but remains controversial.14 Radiofrequency ablation and intraarterial chemotherapy have been reported, but the benefits require further investigation.20,21 The prognosis is variable and is directly related to the resectability and histology of the lesion. In tumors with favorable histology and complete resection, the 2-year survival rate may exceed 97%. However, without complete resection and with unfavorable histology, the 2-year survival rate may be less than 20%.14 In places where the prevalence of tyrosinemia is especially high, routine neonatal screening and immediate treatment of positive cases by 2-(2-nitro-4-3 trifluoromethylbenzoyl)-1,3-cyclohexanedione (NTBC) have resulted in marked decrease in the prevalence of HCC in this population.22 In Quebec, where the prevalence of tyrosinemia is especially high, routine neonatal screening and immediate treatment of positive cases with NTBC have resulted in 100% prevention of subsequent HCC to date in patients treated at birth. However, patients with delayed diagnosis who are treated with NTBC are at risk of having HCC develop. Overview: Fibrolamellar carcinoma (FLC) is a variant of HCC that occurs in patients without underlying hepatic disease. It has distinctive clinical and pathologic features and represents approximately 5% to 8% of all cases of HCC. FLC tends to occur in younger patients, with a peak in the late teens; approximately 85% of patients with FLC are younger than 35 years, and it may be diagnosed in children as young as 10 years. The incidence is similar in males and females.23 Etiology: The etiology of FLC is unknown. It has been reported in association with syndromes, including Wilms, Carney, Fanconi anemia, and familial adenomatous polyposis; these associations have been implicated in shared molecular pathways. FLC also has been associated with FNH, but currently evidence does not support such an association.23 Clinical Presentation: Clinically, patients present with abdominal symptoms or pain and sometimes a palpable mass. Uncommon presentations are gynecomastia, jaundice, and venous compression or thrombosis.9 Metastatic lymphadenopathy is seen in 70% of cases.24 AFP levels generally are normal.16 In 80% to 90% of patients, the gross pathological appearance is one of a large, circumscribed, and nonencapsulated mass.16 Other patterns can be seen, including satellite lesions, multiple diffuse masses, or a bilobed mass. Fibrous tissue within a central scar is common (appearing in 30% of cases) and typically does not enhance after administration of contrast material. Calcifications are seen in 35% to 55% of tumors and are localized in the central scar.16 Imaging: Plain radiographs may demonstrate hepatomegaly or calcifications. Ultrasound shows a well-defined mass with heterogeneous echo texture and isoechoic or hyperechoic areas.25 If it is present, the central scar appears hyperechoic and may contain shadowing hyperechoic calcifications. CT shows a hypoattenuating, well-defined, lobulated mass with calcifications in 30% to 55% of cases and a central scar in 45% to 60% of cases (Fig. 92-4). Adjacent lymphadenopathy often is present in the hepatic hilum at diagnosis. After IV injection of contrast material, in the early arterial phase, the tumor is hyperattenuating relative to the adjacent liver with variable attenuation during the portal venous phase. The central scar is hypoattenuating with little or no enhancement on CT. Figure 92-4 Fibrolamellar carcinoma in an 18-year-old girl. On T1-weighted MRI, the tumor is hypointense (86%) to isointense (14%), and it is slightly hyperintense (85%) to isointense (15%) on T2-weighted images. The fibrous scar is hypointense on T1-weighted images and hypointense on T2-weighted images, and it does usually not enhance after IV administration of contrast material.9,11,15,25,26 These features are useful in distinguishing FLC from FNH, in which the central scar has increased signal on T2-weighted sequences and enhances with IV administration of contrast material. Treatment: The primary treatment of FLC is surgical resection, with surgical resectability considered to be the most important prognostic factor.25 However, when the tumor is not resectable, orthotopic liver transplantation, systemic chemotherapy, or hepatic intraarterial chemoembolization is considered. Recent literature reports no significant difference in the prognosis of FLC compared with HCC in patients without underlying hepatic disease.23,24 Normal hepatic function, younger age, absence of vascular invasion or thrombosis, lack of lymphadenopathy, and negative surgical margins are favorable prognostic indicators. The 5-year survival rate ranges from 30% to 67%.20,21,23,24 Overview: Undifferentiated embryonal sarcoma, previously called malignant mesenchymoma, embryonal sarcoma, or fibromyxosarcoma, is a rare, aggressive tumor of mesenchymal origin. Most commonly, the tumor affects children around 6 to 10 years of age with a slight male predominance.27 In one review, this was the third most common malignant pediatric liver tumor, following hepatoblastoma and HCC.28 Etiology: The etiology of undifferentiated embryonal sarcoma is uncertain. It has been linked to mesenchymal hamartoma as its malignant counterpart,3,15 and some tumors have been reported to arise in a background of mesenchymal hamartoma.29 On histology, an undifferentiated embryonal sarcoma shows primitive spindle-shaped, sarcomatous satellite cells closely packed in sheets or whorls and scattered throughout a background of loose myxoid tissue, which contains foci of hematopoiesis in 50% of cases.27 Clinical Presentation: The most common presenting symptoms include an abdominal mass, pain, and discomfort. An undifferentiated embryonal sarcoma usually is large at presentation, is solitary, involves the right lobe of the liver (in 75% of cases), and is predominantly solid with occasional cystic, necrotic, or hemorrhagic areas.27 AFP levels are normal.15 Imaging: Plain radiographs show a large, typically noncalcified mass. On sonography, the tumor is solid and isoechoic to hyperechoic relative to normal liver with small anechoic spaces that correspond to necrosis, hemorrhage, or cystic degeneration.27,30 On CT, the tumor reveals predominantly water attenuation correlating with myxoid stroma (88% of tumor volume) (e-Fig. 92-5).9,27 After administration of IV contrast material, a dense enhancing peripheral rim can be seen in relation to the pseudocapsule. Uncommon hyperattenuation regions may indicate hemorrhage and calcifications. e-Figure 92-5 Undifferentiated embryonal sarcoma in a 9-year-old girl. With MRI, the tumor shows low signal intensity on T1-weighted sequences and increased signal intensity on T2-weighted sequences (Fig. 92-6). A hypointense rim on T1- and T2-weighted images indicates a pseudocapsule. Bright areas on T1-weighted images correspond to regions of hemorrhage. Fluid levels, internal debris, and septa may be seen on T2-weighted images.27,30 Heterogeneous enhancement of the tumor is seen after IV administration of gadolinium contrast material.31 MRI permits excellent evaluation of tumor resectability, vascular invasion, and involvement of adjacent lymph nodes. Metastases usually are to the lungs and bone. Treatment: Treatment consists of complete tumor resection. As late as three decades ago, the prognosis was poor, with death occurring within 12 months in many cases.28 However, more recent reports of multimodal treatment show markedly improved survival rates. Patients with unresectable tumors that are not responsive to chemotherapy can be treated with liver transplantation.9 Overview: Although rhabdomyosarcoma can be found throughout the body, involvement of the biliary ducts is one of the rarest forms of this mesenchymal tumor. It occurs almost exclusively in the pediatric age group and often in children younger than 5 years (in 75% of cases).9 Etiology: The tumor arises from the biliary tree beneath the biliary epithelium, with which the tumor is invested,32 and grows as a polypoid mass within the biliary tree. Only the embryonal subtype of rhabdomyosarcoma arises in the biliary tree.9 The tumor most commonly involves major extrahepatic bile ducts but can arise within the intrahepatic bile ducts, gallbladder, and cystic duct. Histologically, rhabdomyosarcoma demonstrates undifferentiated blue cells with scant cytoplasm and primitive nuclei that form a firm, lobulated mass with infiltrative margins and a well-defined pseudocapsule.6,9,12,33 Clinical Presentation: Jaundice, the most frequent manifestation, can be associated with abdominal distention, pain, nausea, vomiting, or fever. Elevated levels of conjugated bilirubin and alkaline phosphatase with normal levels of AFP are typical of the laboratory workup. At diagnosis, metastases are present in 30% of cases9 and typically appear in the lung, appendicular skeleton, skull, and pericardium, although the tumor has a greater propensity to invade contiguous structures.32 The clinical presentation may resemble that of hepatitis, which may lead to delay in obtaining diagnostic tests.34 Imaging: Multiplanar imaging demonstrates a mass within the biliary ducts. The tumor most frequently involves the common bile duct, in or near the porta hepatis. In large lesions, necrosis can be seen. Ultrasound may reveal a solitary, heterogeneous, relatively hypoechoic mass or multiple hypoechoic nodules associated with biliary duct dilation and intraductal extension.9,35 Portal vein displacement without thrombosis is common.35 CT shows a homogeneous or heterogeneous hypoattenuating or hyperattenuating intraductal mass with variable contrast enhancement associated with biliary dilatation (Fig. 92-7).35,36 MRI usually shows low signal intensity on T1-weighted sequences and high signal intensity on T2-weighted sequences, with intense, heterogeneous enhancement after IV administration of contrast material.9,35 Magnetic resonance cholangiopancreatography often demonstrates a partially cystic lesion in the common bile duct and a mass adjacent to the duct causing mural irregularity. Percutaneous cholangiography displays an intraluminal polypoid mass.35–37 Gallium uptake can help localize metastatic disease.35
Neoplasia
Overview
Malignant Hepatobiliary Tumors
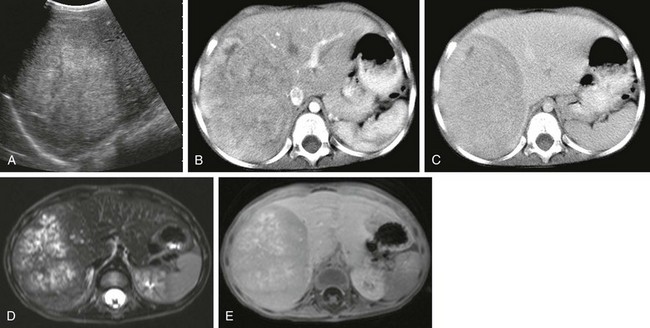
A, A longitudinal abdominal sonogram in a 3-year-old boy shows a well-defined lesion that is hyperechoic relative to the liver. B, A computed tomography (CT) scan in the early arterial postcontrast phase demonstrates a heterogeneous mass that is hyperdense compared with the liver. C, A CT scan in the delayed contrast phase shows a hypodense lesion. D, An axial T2-weighted magnetic resonance (MR) image shows hyperintense nodules with intervening hypointense septa. E, An axial T1-weighted MR image after intravenous administration of gadolinium demonstrates enhancement of the septa and capsule.
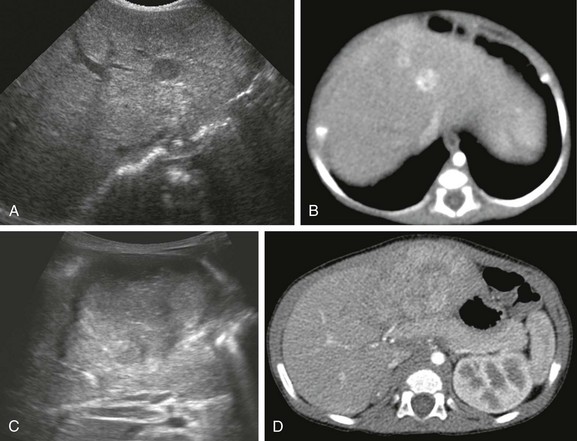
A, A sonogram of a 71-day-old girl with Beckwith-Wiedemann syndrome shows a hypoechoic lesion in segment IV-A of the liver. B, An enhanced computed tomography (CT) scan reveals marked enhancement of the lesion. C, Eight months after the first ultrasound, a transverse ultrasound image shows a large hypoechoic mass with a lobular margin. D, An enhanced CT scan shows a circumscribed heterogeneous lesion with lobular enhancement.
Hepatocellular Carcinoma
A, An abdominal sonogram shows a heterogeneous hepatic lesion. B, An unenhanced computed tomography scan demonstrates the liver mass, with slightly decreased attenuation compared with adjacent normal liver parenchyma. Postcontrast arterial (C) and venous phase (D) images show enhancement during the arterial phase, which decreases during the venous phase. After administration of contrast material, the tumor margins are more conspicuous.
Fibrolamellar Carcinoma

Axial contrast-enhanced computed tomography shows a lobulated mass (arrows) in the left lobe of the liver with a hypoattenuating central scar.
Undifferentiated Embryonal Sarcoma
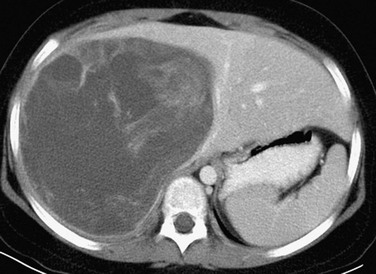
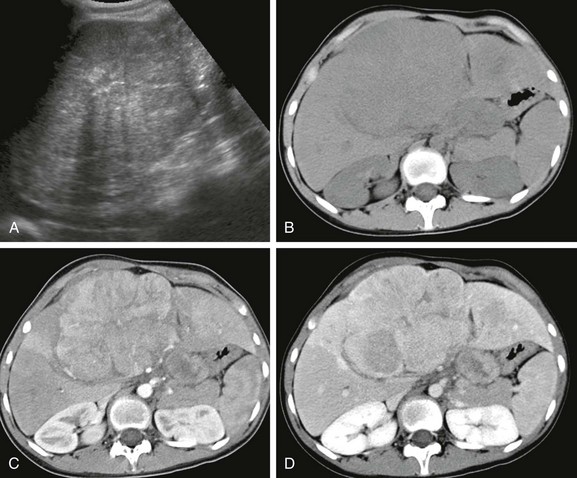
A postcontrast computed tomography image shows a large, well-defined, heterogeneously enhancing but low-attenuation mass in the right hepatic lobe. (Courtesy Robert P Guillerman, MD.)
Rhabdomyosarcoma of the Biliary Tree
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








