Associated with other diseases and drugs (e.g., myeloproliferative; immunosuppressives)
Signs of portal hypertension are common (> 50%)
• LRNs
Multiple focal liver masses or nodules 0.5-5 cm in size with persistent enhancement on hepatobiliary-enhanced MR
Hyperintense on T1WI (75%); iso- to hyperintense on T2WI
Hypervascular on arterial, portal venous and delayed phase imaging (no washout)
May have central scar ± perinodular “halo”
MR with hepatobiliary agents: Uptake and prolonged enhancement
– Confirms benign hepatocellular nature of lesions
With signs of underlying disease (e.g., Budd-Chiari; thrombosed hepatic veins + IVC)
• LRNs: Multiple hypervascular nodules up to 5 cm with persistent delayed enhancement on hepatobiliary-enhanced MR
TOP DIFFERENTIAL DIAGNOSES
• Imaging features are more diagnostic than histologic features
• Multifocal hepatocellular carcinoma
• Focal nodular hyperplasia (multiple)
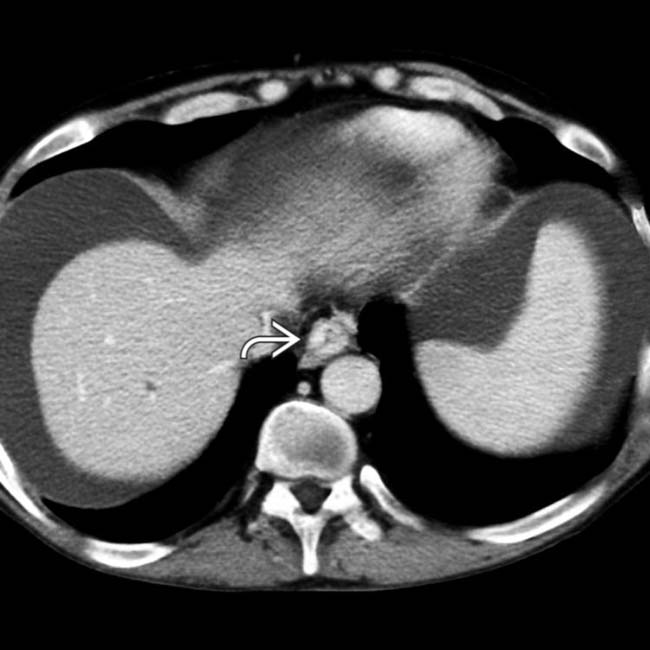
(Left) Axial CECT in a 52-year-old man with a renal transplant shows massive ascites and esophageal varices .
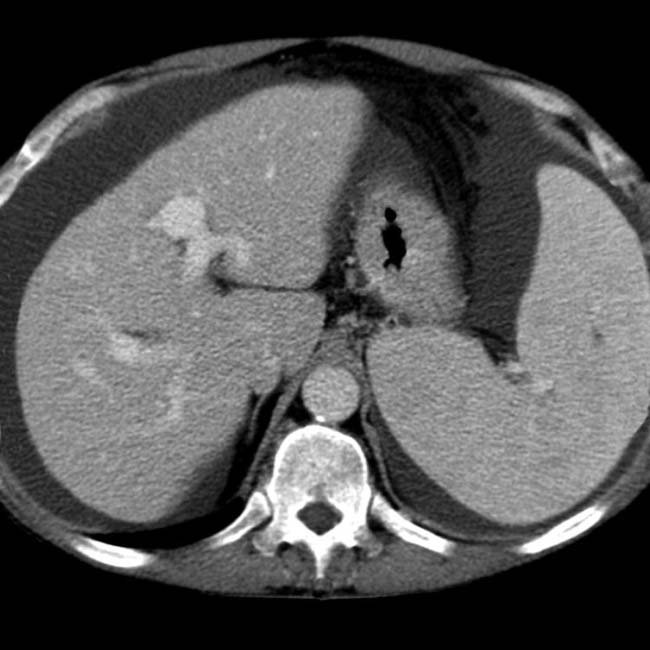
(Right) Axial CT section of the liver in the same patient shows no evidence of fibrosis or focal lesions; liver biopsy showed no cirrhosis, but diffuse nodular regenerative hyperplasia (NRH) was found. This is a recognized cause of liver failure in the absence of cirrhosis and a known complication of solid organ transplantation, among many other etiologies.
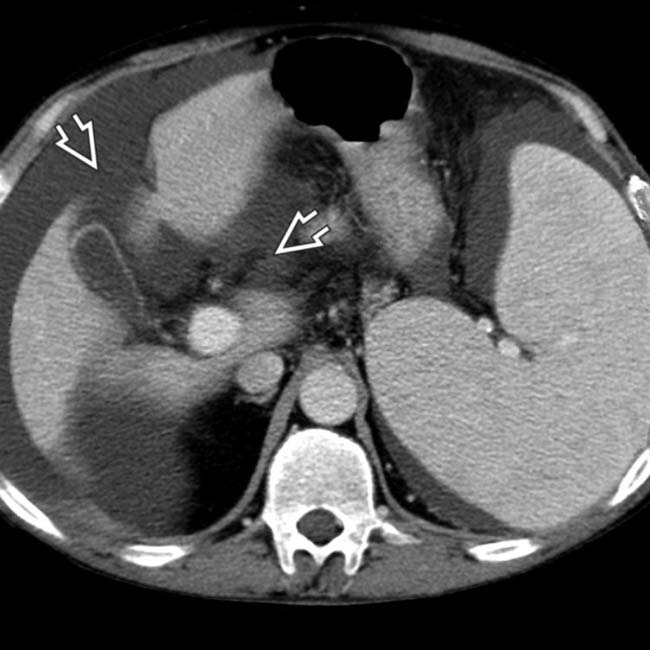
(Left) Another CT section in the same renal transplant patient shows widened hepatic fissures , suggestive of cirrhosis. Liver biopsy showed diffuse nodular regenerative hyperplasia.
(Right) Trichrome stain highlights the nodules . By definition, there are no fibrous septa between the nodules in nodular regenerative hyperplasia. (Courtesy S. Kakar, MD.)
TERMINOLOGY
Abbreviations
• Nodular regenerative hyperplasia (NRH)
Synonyms
• Nodular transformation, noncirrhotic nodulation
Definitions
• Uncommonly recognized disorder characterized by diffuse micronodular or macronodular transformation of hepatic parenchyma without fibrous septa between nodules
• Larger focal lesions are called multiacinar (large) regenerative nodules (LRNs)
IMAGING
General Features
• Best diagnostic clue
LRNs: Multiple hypervascular nodules up to 5 cm with persistent delayed enhancement on hepatobiliary-enhanced MR
• Location
Diffuse involvement; microscopic nodules predominantly distributed in periportal region
• Size
Monoacinar lesions in NRH are only ∼ 1 mm in diameter, with clusters of lesions up to 10 mm
LRNs are 0.5-5 cm in diameter
• Key concepts
Diffuse NRH and focal LRNs have different predisposing conditions and different imaging features
CT Findings
• NECT
Nodules are usually isoattenuating to normal liver
Diffuse low attenuation in Budd-Chiari syndrome or steatosis may result in hyperattenuation of nodules
• CECT
Diffuse nodular regenerative hyperplasia
– No focal liver masses; liver may appear normal or dysmorphic
– Signs of portal hypertension are common (> 50% of reported cases)
Splenomegaly, ascites, varices
Large regenerative nodules
– Multiple focal liver masses or nodules (2 to hundreds)
Size of nodules: 0.5-5 cm
Homogeneously hypervascular on arterial and portal venous phase imaging (no washout)
May have central scar ± perinodular hypo-/hyperdense halo
Along with signs of underlying disease (e.g., for Budd-Chiari = thrombosed hepatic veins and IVC, central hepatic hypertrophy, and peripheral atrophy)
Signs of portal hypertension in > 50%
MR Findings
• T1WI
LRNs: Hyperintense (75%)
• T2WI
Isointense or hypointense nodules; fewer detected
May appear hyperintense (due to infarction)
Halo sign: Nodule surrounded by peliosis
• Multiphasic enhanced MR
Bright homogeneous enhancement on arterial and portal venous phase
± ring (halo) enhancement; ± central scar
• MR with hepatobiliary contrast (e.g., gadoxetate): Uptake and prolonged enhancement
Confirms benign hepatocellular nature of lesions
Bright uniform or peripheral enhancement
Mimics appearance of focal nodular hyperplasia (FNH) (as does histology)
Ultrasonographic Findings
• Grayscale ultrasound
Nodules may appear as hypoechoic (38%), isoechoic (10%), or hyperechoic (53%) lesions
• Color Doppler
Nodules have prominent arterial supply
May detect signs of underlying disease (e.g., Budd-Chiari with hepatic vein, IVC thrombosis, ascites)
Angiographic Findings
• Conventional
Nodules
– May fill from periphery on angiography
– Vascular
– Sometimes contain small hypovascular areas due to hemorrhage or scar
Nuclear Medicine Findings
• Nodules take up technetium sulfur colloid
Imaging Recommendations
• Best imaging tool
Multiphasic CT or MR
• Protocol advice
MR with gadobenate dimeglumine or gadoxetate enhancement
– Allows definitive diagnosis of LRNs
DIFFERENTIAL DIAGNOSIS
Multifocal Hepatocellular Carcinoma (HCC)
• Heterogeneously hyperdense on arterial phase with rapid washout (CT and MR)
Only gold members can continue reading. Log In or Register to continue

 Multiple focal liver masses or nodules 0.5-5 cm in size with persistent enhancement on hepatobiliary-enhanced MR
Multiple focal liver masses or nodules 0.5-5 cm in size with persistent enhancement on hepatobiliary-enhanced MR




 .
.
 , suggestive of cirrhosis. Liver biopsy showed diffuse nodular regenerative hyperplasia.
, suggestive of cirrhosis. Liver biopsy showed diffuse nodular regenerative hyperplasia.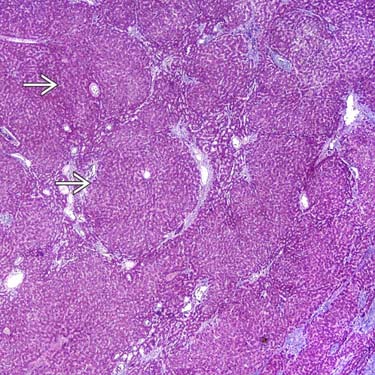
 . By definition, there are no fibrous septa between the nodules in nodular regenerative hyperplasia. (Courtesy S. Kakar, MD.)
. By definition, there are no fibrous septa between the nodules in nodular regenerative hyperplasia. (Courtesy S. Kakar, MD.)


































