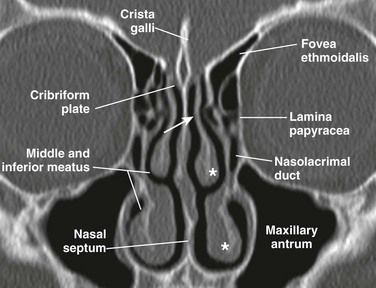
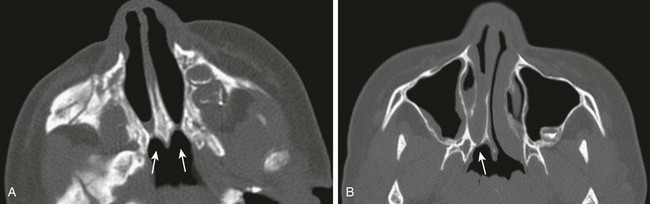
Chapter 8 The nasal cavity is triangular and is separated in the midline by the nasal septum. The nasal cavity is composed of a cartilaginous portion anteriorly and an osseous portion posteriorly, which is formed by the perpendicular plate of the ethmoid posterosuperiorly and the vomer posteroinferiorly. The opening to each nasal cavity is known as the vestibule, which is bounded medially by the columella and nasal septum and laterally by the nasal alae. The cribriform plate is the roof of the nasal cavity, and the floor is the hard and soft palate. Posteriorly, the nasal cavity communicates with the nasopharynx via the choanae, after rupture of the oronasal membrane during the fetal period. From the lateral wall of the nasal cavity, three pairs of turbinates (superior, middle, and inferior) project into the nasal cavity, each with a corresponding meatus below them. The middle turbinate is attached to the cribriform plate via the vertical lamella and to the lamina papyracea via the basal lamella (Fig. 8-1). The paranasal sinuses form as diverticula from the walls of the nasal cavities and become air-filled extensions in the adjacent bones—maxilla, ethmoid, frontal, and sphenoid. The original openings of the diverticula persist as the ostia of the sinuses that communicate with the nasal cavity (Fig. 8-2, A and B). Figure 8-2 Normal sinus openings. The mucosal lining of the nasal cavities is contiguous with the paranasal sinuses and consists of pseudostratified, columnar, ciliated epithelium containing mucinous and serous glands,1 whereas the nasal septum is lined by squamous mucosa.2 In the human embryo, ethmoidal and maxillary sinus budding can be detected at 11 to 12 gestational weeks and at 14 to 15 gestational weeks, respectively.3 In general, only rudimentary maxillary and ethmoid sinuses, which continue to expand until puberty or early adulthood, are present at birth.4 The sinuses also are linked to facial growth and dentition and have been studied extensively by different anatomic and imaging methods (Fig. 8-3, A-C).4–11 Figure 8-3 Normal anatomy of the sinuses demonstrated by fully developed sinuses in a 13-year-old boy. At birth the ethmoid sinuses are already developed in number and pneumatized, but they continue to expand, reaching adult proportions at about 12 years of age.12 The ethmoid sinuses consist of a paired group of a variable number of cells (3 to 18) within the lateral masses of the ethmoid bone, also known as labyrinths. In addition to the lateral masses, the ethmoid bone consists of the cribriform plate superiorly and the perpendicular plate, which is part of the nasal septum (see Fig. 8-3, A). The ethmoid sinus is bordered medially by the nasal cavity and laterally by the lamina papyracea; its roof is formed by the cribriform plate and fovea ethmoidalis (see Fig. 8-1). The anterior and posterior ethmoid air cells are separated by the basal lamella (see Fig. 8-3, C), which is the lateral attachment of the middle turbinate to the lamina papyracea. Drainage of the anterior ethmoid air cells occurs via the ethmoid bulla into the hiatus semilunaris and middle meatus. The posterior ethmoid air cells drain into the superior meatus and then into the sphenoethmoid recess (see Fig. 8-2, A). The anterior ethmoidal artery arises from the ophthalmic artery in the orbit, pierces the lamina papyracea, and exits via its respective foramina by passing through the ethmoid roof in the superomedial wall of the orbit, 2 to 3 mm behind the anterior wall of the bulla ethmoidalis. Occasionally the anterior ethmoidal artery passes within bony septae of the ethmoid sinuses and is suspended in a mesentery without bony cover (e-Fig. 8-4).13 The roof of the anterior ethmoid sinus is formed by the cribriform bone medially and the fovea ethmoidalis laterally (see Fig. 8-1). Any asymmetry in the height of the ethmoid roof should be documented by the radiologist because a higher incidence of surgical penetration occurs during endoscopic surgery on the side where the position of the roof is lower.14,15 An increased risk of inadvertent intracranial penetration may occur if the fovea ethmoidalis plane passes through the midorbital plane or below. Concha bullosa refers to the pneumatization of the middle turbinate as a result of intramural extension of posterior ethmoid air cells (Fig. 8-5, B). A large concha bullosa eventually can cause obstruction of the airway. Figure 8-5 Anatomic variants. Extramural expansion of ethmoid air cells can result in anatomic variants, including the following: Agger nasi cells (Fig. 8-5, A), which are the most anterior and inferior cells involving the lacrimal bone or maxilla; Haller cells, which are middle ethmoid air cells extending into the inferomedial floor of the orbit (Fig. 8-5, C); and Onodi cells, which are posterior sphenoethmoid air cells with prominent superolateral pneumatization in close relationship to the optic nerve canal.13 The maxillary sinuses are very small and pneumatized at birth, measuring an ellipsoid volume (sinus volume index) of approximately 0.24 ± 0.36 cm3.4 During the first years of life, the maxillary sinuses undergo rapid inferolateral expansion, reaching full size between 15 to 18 years of age. The floor of the maxillary sinus usually is seen at the level of the middle meatus during infancy; it reaches the level of the nasal floor by 8 to 9 years of age, and by age 12 years, it is located at the level of the hard palate.6 However, variation exists in the final descent of the floor, which lies below the level of the nasal floor in 65% of adults (e-Fig. 8-6, A–D).16 e-Figure 8-6 Maxillary sinus development. The maxillary sinus is the largest of the sinuses. Its roof is formed by the orbital floor, which carries the bony canal for the infraorbital nerve; the medial wall is formed by the lateral nasal wall. The posterior wall of the maxillary sinus forms the pterygopalatine fossa (Fig. 8-7, A). The maxillary sinus drains via the maxillary ostium located superomedially into the infundibulum, the hiatus semilunaris, and the middle meatus (Fig. 8-2, A). Figure 8-7 Sphenoid sinus anatomy and variants. The sphenoid sinus begins to pneumatize in a ventrodorsal direction from 7 months to 2 years of age. A significant acceleration in sinus expansion occurs between 3 and 8 years of age, with complete pneumatization usually present by age 10 years (e-Fig. 8-8, A–E).9 Its border is formed superiorly by the sella turcica, posteriorly by the clivus, anteriorly by the ethmoid sinus, and inferiorly by the nasopharynx (see Fig. 8-2, A and B). This sinus drains anteriorly via the sphenoethmoid recess. Lateral recesses of the sphenoid sinus are formed from pneumatization of the pterygoid process in 44% of people (see Fig. 8-7, A). Benign sphenoid marrow variants, which sometimes are mistaken for lesions, can be seen adjacent to the pneumatized sphenoid sinus (e-Fig. 8-9, A-C). e-Figure 8-8 Sphenoid sinus development is shown in magnetic resonance sagittal T1-weighted images. e-Figure 8-9 Benign sphenoid marrow variants. Important anatomic relationships of the sphenoid sinus include the optic canal and nerve located superolaterally; the foramen rotundum with the maxillary nerve that courses along the inferolateral margin of the sphenoid sinus; the vidian canal, which usually runs along the floor of the sphenoid sinus; and the cavernous portion of the internal carotid artery, which protrudes laterally into the sinus (see Fig. 8-7, B). The sphenoid sinus septum usually is aligned anteriorly with the nasal septum, but the sinus septum can deviate posteriorly, forming unequal sphenoid cavities (see Fig. 8-7, C). Absent pneumatization in a child older than 9 years is usually abnormal and warrants clinical investigation (see Fig. 8-7, D). The frontal sinuses are absent at birth and are the last to develop once bone marrow conversion has occurred. The frontal sinus is considered an extension of the anterior ethmoid air cells and pneumatizes between 2 to 8 years, with the most significant growth taking place between ages 1 to 5 years. The frontal sinuses can continue to expand up until the second decade of life.6,11 The frontal sinuses consist of paired, often asymmetric cells. The anterior wall corresponds to the outer cortical table of the frontal bone, and the posterior wall of the sinus separates it from the anterior cranial fossa. Drainage of this sinus occurs via the frontal recess, which is an hourglass-like narrowing between the frontal sinus and the anterior middle meatus (see Fig. 8-2, A). Hypoplasia and aplasia of the frontal sinus can be seen in 4% and 5% of the population, respectively. Although plain radiography is less costly and more widely available than computed tomography (CT), it has significant limitations in evaluating the paranasal sinuses. Specifically, plain radiography often overestimates or underestimates findings, it does not localize pathology well, and it does not provide important anatomic detail.17 Traditionally, the paranasal sinus series has consisted of four views (Caldwell, Waters, posteroanterior, and lateral) that are technically difficult to perform in children. The Waters view is obtained by angulating the beam in 5-degree increments per year (up to age 6 years) to compensate for the progressive enlargement of the maxillary antra throughout childhood (Fig. 8-10, A and B). Although this approach improves visualization of the maxillary sinuses by projecting them over the petrous pyramids, it also creates double contours that can simulate mucosal thickening. Radiographic density also is critical because overpenetration of the films can completely obscure density differences created by disease, whereas underpenetration can simulate disease. Air fluid levels also can be obscured as a result of beam angulation. Although some have suggested using only the Waters view radiograph, this modality has been shown to have 32% false-negative results and 49.2% false-positive results when compared with CT. Moreover, most of the abnormalities in the ethmoid and sphenoid sinus are not detected in the Waters radiograph.18 Ethmoid disease on the Caldwell projection can be overdiagnosed or underdiagnosed because of technical and anatomic factors. The lateral view for evaluating the sphenoid sinus is of very little value in children younger than 4 years.17,19 Figure 8-10 Plain radiograph—Waters view. The American College of Radiology does not recommend the use of plain radiography in diagnosing sinusitis in children. Sinusitis is considered a clinical diagnosis that should not be made on the basis of imaging findings alone.20 Similarly, American Academy of Pediatrics (AAP) guidelines state that plain radiographs are unnecessary for diagnosing sinonasal disease in children younger than 6 years.21 Further, plain films do not play a role in evaluating sinonasal masses or complications of sinusitis. In recent years, there has been heightened awareness of and concern about the potentially harmful side effects associated with radiation exposure, particularly in the pediatric population.22,23 For this reason, the practice of the “as low as is reasonably achievable” principle among the radiologic community is critical, with special attention given to CT protocols and parameters.22,24 In evaluating paranasal sinuses, it is possible to reduce radiation techniques for maxillofacial CT imaging, even to a level comparable to that used for standard radiographic images, without sacrificing diagnostic image quality.25 The normal nasal cycle of vasodilation and mucosal edema followed by vasoconstriction and mucosal shrinkage can produce signal changes that can create significant variability in findings and thus differing interpretations. This cycle varies from 50 minutes to 6 hours, and the signal intensity during the edematous phase is indistinguishable from that of inflammatory change. As with CT and plain radiographs, sinus MRI typically shows a high incidence of findings in asymptomatic persons (13% to 37%) and mucosal thickening of <3 mm that is likely insignificant.2 MRI can differentiate mucosal thickening from sinus secretions (Fig. 8-11, A–E). Figure 8-11 Acute bacterial sinusitis in a 10-year-old boy. Regarded as an important anatomic region for potential surgical intervention, the ostiomeatal unit is a complex anatomic structure at the crossroads of mucociliary drainage from the frontal, anterior ethmoid, and maxillary sinuses.26 It includes the uncinate process, infundibulum, ethmoid bulla, hiatus semilunaris, and middle meatus (Fig. 8-12, A and B).13 Figure 8-12 Ostiomeatal unit (OMU). The uncinate process arises from the upper medial maxillary wall and defines the wall of the infundibulum.27 The infundibulum is the channel defined laterally by orbit or Haller cells and medially by the uncinate process. The ethmoid bulla is a dominant middle ethmoid air cell that protrudes inferomedially into the infundibulum and hiatus semilunaris. The hiatus semilunaris is a semilunar region between the tip of the uncinate process and ethmoid bulla (see Fig. 8-12, A and B). Choanal atresia, the most common congenital abnormality of the nasal cavity, is thought to result from failure of rupture of the oronasal membrane during the sixth week of fetal life. It consists of obstruction of the posterior opening of the nasal cavity, which is mixed bony-membranous in approximately 70% of cases and pure bony atresia in 30% of cases. The existence of a purely membranous atresia has been questioned, and evaluation with high-resolution CT often has failed to demonstrate a membranous atresia without a bony component.28 Choanal atresia can be unilateral (in 50% to 60% of cases) or bilateral, and it is more common in girls (the female : male ratio is 2 : 1). Clinical Presentation: Bilateral choanal atresia presents with severe immediate onset of respiratory distress in the newborn, because infants are obligate nasal breathers. Symptoms are aggravated by feeding and relieved by crying. The inability to pass a nasogastric tube in a neonate with well-aerated lungs suggests the diagnosis. Unilateral choanal atresia usually is diagnosed later in childhood and presents with unilateral purulent rhinorrhea. Imaging: Noncontrast CT is the imaging modality of choice. Nasal secretions should be suctioned before imaging is performed; administration of a nasal topical vasoconstrictor spray helps in reducing mucosal thickening. High-resolution imaging in bone algorithm will aid in delineating the bone margins. Findings consist of narrowing of the posterior choana (<0.34 cm in children <2 years of age) and enlargement and thickening of the vomer (>0.23 cm), which sometimes is fused to the maxilla.29 Medial bowing and thickening of the posterior aspect of the lateral wall of the nasal cavity also is seen. The nasal cavity often is filled with air, soft tissue, and fluid (Fig. 8-13, A and B). CT will identify other causes of bilateral nasal obstruction such as pyriform aperture stenosis and bilateral nasolacrimal duct cysts. Bilateral choanal atresia can be associated with other congenital abnormalities in 75% of cases, such as in persons with CHARGE syndrome. Figure 8-13 A,
Nose and Sinonasal Cavities
Development and Anatomy of the Sinonasal Cavities
Paranasal Sinuses
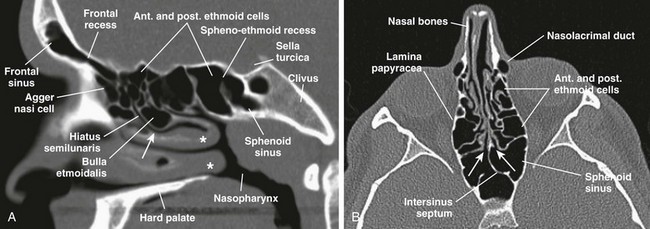
A, A sagittal computed tomography (CT) scan shows frontal recess of the frontal sinus, hiatus semilunaris, middle meatus (arrow), sphenoethmoid recess, and middle and inferior turbinates (asterisks). B, An axial CT view shows sphenoethmoid recesses (arrows).
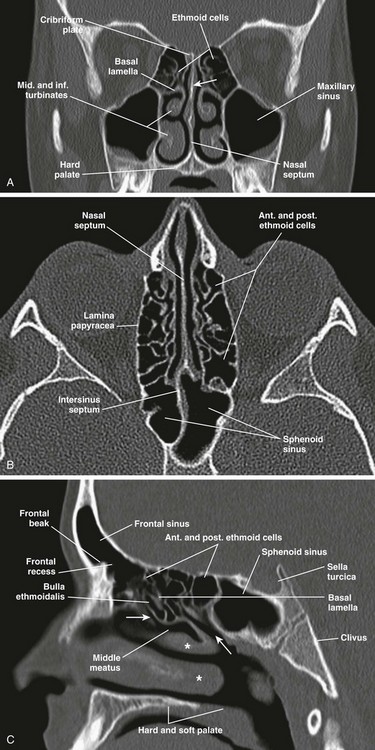
A, A coronal computed tomography (CT) scan shows the perpendicular plate of the ethmoid bone (arrow). B, An axial CT image. C, A sagittal CT image shows hiatus semilunaris (arrow at left), drainage passage of posterior ethmoid cells (arrow at right), and middle and inferior turbinates (asterisks).
Ethmoid Sinuses
Anatomic Variants
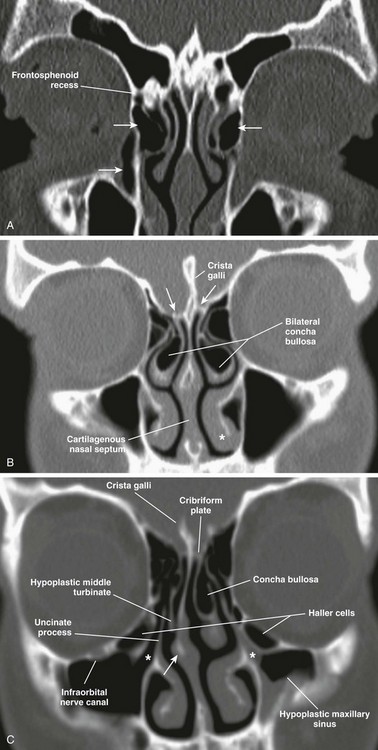
A, A coronal computed tomography scan shows bilateral agger nasi cells (top arrows), the nasolacrimal canal (bottom arrow), and the right frontoethmoidal recess. B, Bilateral concha bullosa, asymmetric height of the ethmoid roofs (arrows), and the inferior turbinate (asterisk) are shown. C, A hypoplastic right middle turbinate, rightward nasal septal deviation, Haller cells, and infundibulum (asterisks) are shown.
Maxillary Sinuses
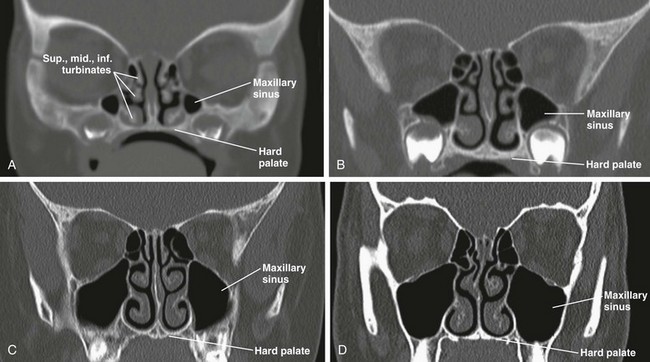
Computed tomography images show maxillary sinuses at 1 month (A), 3 years (B), 7 years (C), and 15 years (D).
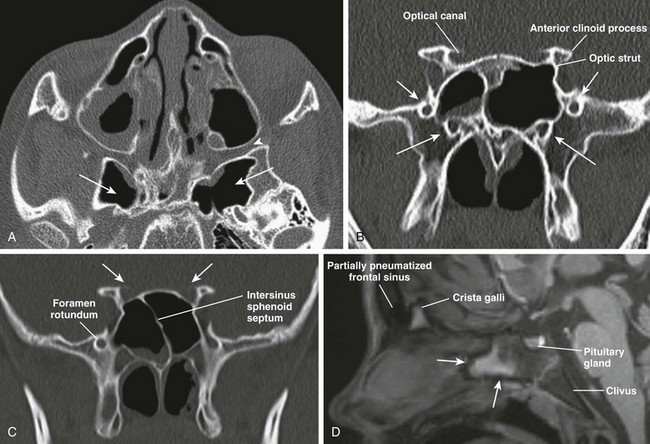
A, An axial computed tomography (CT) image shows hyperpneumatization of the sphenoid sinus involving the pterygoid plates bilaterally (arrows); the pterygopalatine fossa (arrowhead) also is shown. B, A CT image shows foramen rotundum (short arrows) and the vidian canal (long arrows) bilaterally. C, A coronal CT image shows insertion of the intersinus septum into the right optic canal (arrows). D, A sagittal T1-weighted magnetic resonance image demonstrates a nonpneumatized sphenoid sinus in an 11-year-old boy with fatty transformation of its anteroinferior portion (arrows).
Sphenoid Sinus
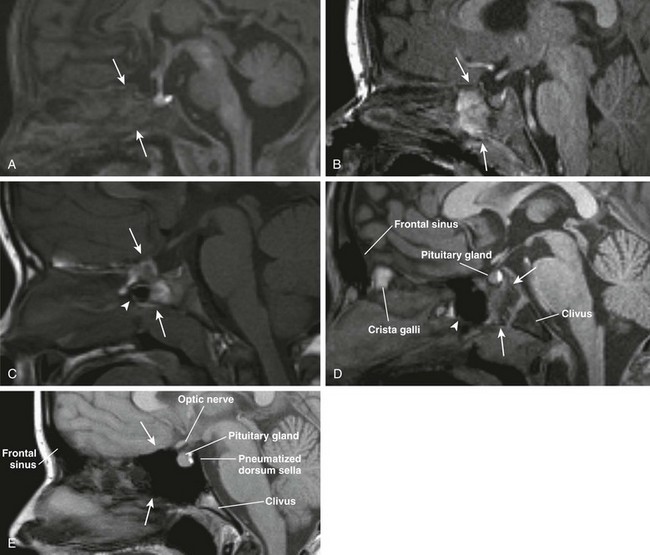
A, Hematopoietic marrow (T1 hypointense) of the sphenoid bone in a newborn (thin arrows). B, Fatty transformation of the anteroinferior aspect of the sphenoid bone in a 12-month-old (arrows). C, Pneumatization of the anteroinferior aspect of the sphenoid sinus in a 3-year-old (arrowhead) with fatty sphenoid marrow (arrows). D, Further pneumatization of the sphenoid sinus (arrowhead) and fatty transformation of the sphenoid bone (arrows). E, Fully pneumatized sphenoid sinus (arrows), including the dorsum sella in a 14-year-old boy.
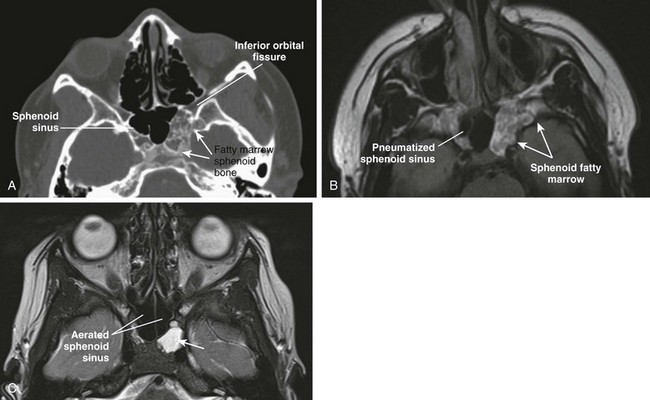
A, An axial computed tomography (CT) image shows asymmetric fatty marrow of nonpneumatized sphenoid bone on the left side. B, An axial T1-weighted image shows correlation of T1-hyperintense normal marrow of the sphenoid bone, which can simulate mass (neoplasm/erosion). C, An axial CT image in another patient shows retained fluid in the left lateral recess of the sphenoid sinus.
Frontal Sinuses
Imaging of the Paranasal Sinuses
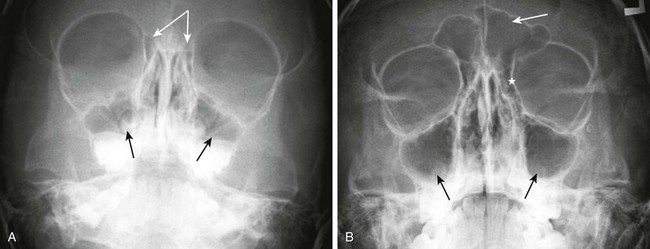
A, Maxillary sinuses (single arrows) and ethmoid air cells (attached arrows) in a 3-year-old child. B, Maxillary sinuses (bottom arrows), frontal sinus (top arrow), and ethmoid air cells (asterisk) in an 11-year-old child.
Computed Tomography
Magnetic Resonance Imaging
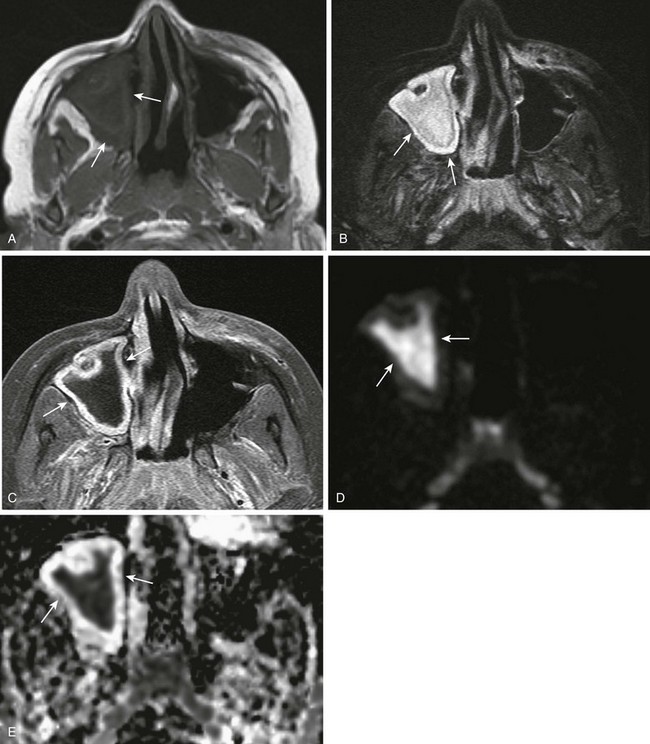
A, An axial T1-weighted magnetic resonance (MR) image shows hypointense material in the right maxillary sinus (arrows). B, An axial T2-weighted MR image shows corresponding T2-hyperintense material (arrows). C, An axial T1-weighted MR image with fat saturation and contrast shows circumferential mucosal enhancement. D and E, Corresponding decreased diffusivity in the right maxillary sinus is shown on diffusion-weighted imaging and apparent diffusion coefficient maps consistent with purulent material.
Imaging Anatomy of the Sinonasal Cavities
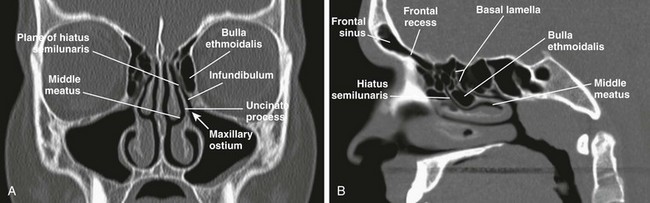
A, A coronal computed tomography (CT) image shows the OMU components: middle meatus, uncinate process, infundibulum, bulla ethmoidalis, maxillary ostium, and plane of the hiatus semilunaris. B, A sagittal CT image demonstrates the hiatus semilunaris.
Congenital Lesions of the Nose
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree