Heterogeneous, encapsulated mass located within omentum (usually in right lower quadrant)
– Surrounding inflammatory change and fat stranding ± small free fluid
Variable attenuation, but usually foci of fat attenuation
Usually well circumscribed with peripheral hyperdense rim
– May appear ill defined as poorly marginated fat stranding without discrete mass in earliest stages
No central dot sign (seen with epiploic appendagitis)
Whorled pattern of vessels leading to infarct may reflect torsion of vessels feeding omentum
• Ultrasound appearance
Hyperechoic, nonmobile, noncompressible fixed mass arising in omentum
– Decreased or absent flow within echogenic mass
Focal tenderness with graded compression
PATHOLOGY
• Most cases idiopathic (obesity is predisposing factor)
• Other causes include abdominal surgery, trauma, incarcerated hernia, etc.
CLINICAL ISSUES
• Clinical presentation may mimic acute appendicitis
Usually normal WBC and lack of nausea, vomiting, diarrhea, or constitutional symptoms
• Benign disorder almost never associated with complications
• Usually self-limiting process that resolves spontaneously and should be treated only with pain management
• If diagnosed prospectively on CT, surgery should not be performed
(Left) Axial CECT in a patient with abdominal pain demonstrates an ill-defined, fat-containing mass in the omentum with a subtle peripheral rim, in keeping with an omental infarct. The patient’s pain resolved in a few days with conservative therapy.
(Right) Axial CECT demonstrates a well-circumscribed fatty mass with a peripheral hyperdense rim in the right omentum. The patient had experienced RLQ pain about 1 week earlier, and this was thought to be a subacute omental infarct.
(Left) Axial CECT in a patient with abdominal pain shows a classic omental infarct as a fatty mass with a hyperdense rim adjacent to the ascending colon.
(Right) Axial CECT in the same patient demonstrates a “swirled” appearance of an omental vessel within the infarcted omentum, indicating twisting of the omental pedicle, which may be the etiology of the infarct in some cases.
TERMINOLOGY
Definitions
• Fat necrosis caused by interruption of arterial blood supply to omentum
IMAGING
General Features
• Best diagnostic clue
Focal mass of heterogeneous density within omental fat with surrounding soft tissue inflammation
• Size
Varies from 3.5-15 cm
Larger infarcts often associated with surgery
• Morphology
Focal heterogeneous mass composed of inflamed omental fat ± hemorrhage
Usually well circumscribed, and appear triangular, ovoid, or cake-like in shape
CT Findings
• Heterogeneous, encapsulated mass located within omentum between anterior abdominal wall and colon
Can have variable internal attenuation, but usually some internal foci of fat attenuation (-20 to -50 HU)
Usually well-circumscribed margins with peripheral hyperdense rim, particularly when occurring after surgery
– Infarcts in earliest stages may appear ill defined: Sites of poorly marginated fat stranding without discrete mass
Does not have central dot sign seen with epiploic appendagitis
Whorled pattern of vessels leading to infarct may reflect torsion of vessels feeding omentum
• Often associated with surrounding inflammatory change and fat stranding ± small free fluid
• May be adherent to either colon or parietal peritoneum
Only rarely causes reactive colonic wall thickening
Rarely causes reactive thickening of overlying abdominal wall
• Usually located in right inferior omentum, especially when idiopathic
Usually located adjacent to site of surgery when occurring in postoperative setting
Ultrasonographic Findings
• Grayscale ultrasound
Echogenic, nonmobile, noncompressible fixed mass arising in omentum
– Associated with focal tenderness when graded compression applied to site
– Echogenic fat surrounding mass (reflects inflammation) ± small free fluid
• Color Doppler
Decreased or absent flow within echogenic mass
Nuclear Medicine Findings
• PET/CT
Omental infarcts may demonstrate FDG avidity suggesting tumor (if not correlated with CT appearance)
Imaging Recommendations
• Best imaging tool
CECT
• Protocol advice
DIFFERENTIAL DIAGNOSIS
Acute Appendicitis
• Can mimic omental infarction clinically, but distinction readily made with cross-sectional imaging
• Dilated appendix with wall thickening, mucosal hyperemia, and periappendiceal fat stranding, inflammation, and free fluid
May demonstrate reactive wall thickening of cecum or terminal ileum
Fluid collection, abscess, or ectopic gas in setting of perforation
Appendicolith may be seen in 10-15% of cases
• Noncompressible appendix ≥ 7 mm on graded compression US often with increased color flow vascularity
Epiploic Appendagitis
• Benign and self-limited disorder: 1% of patients with acute right lower quadrant pain
Most commonly caused by primary thrombosis or torsion of epiploic appendage, but rarely secondary to adjacent inflammation (diverticulitis, appendicitis, etc.)
• May appear similar to omental infarct, but distinction is irrelevant, as both entities treated conservatively
• CT: Small fatty mass with hyperattenuating ring abutting colon with mild adjacent fat stranding
Central dot sign due to thrombosed vessel commonly present, not seen with omental infarcts
May rarely cause reactive wall thickening of colon and thickening of parietal peritoneum
Most common in left lower quadrant (rectosigmoid), unlike omental infarcts which occur in right lower quadrant
Liposarcoma
• Large omental infarcts can mimic fatty tumor (i.e., liposarcoma)
• Distinction based on clinical presentation (omental infarcts present with acute pain) and change over time (tumor grows over time while infarct should get smaller)
• Biopsy may be required in some rare cases
Pancreatitis With Extrapancreatic Fat Necrosis
• Focal or diffuse enlargement of pancreas with peripancreatic fluid and stranding ± fluid collections
• Release of pancreatic enzymes into surrounding tissues can cause extrapancreatic fat necrosis
May appear focal and mimic omental infarct or tumor
Only gold members can continue reading. Log In or Register to continue







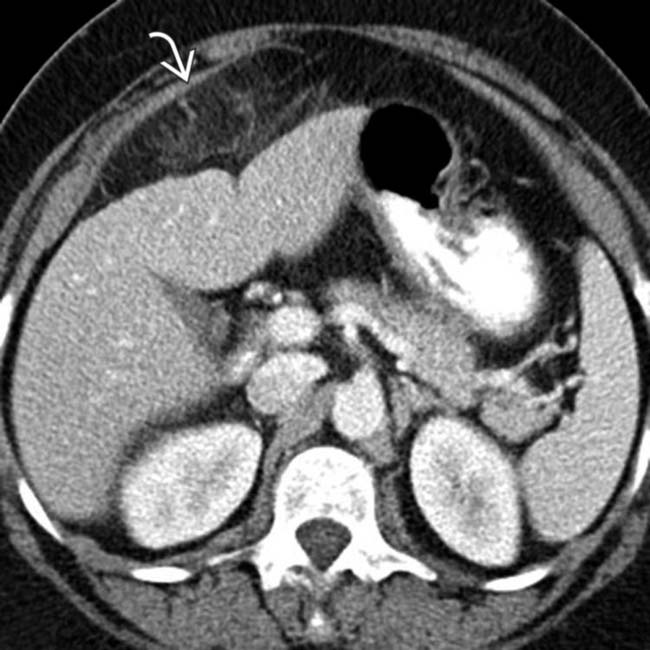
 in the omentum with a subtle peripheral rim, in keeping with an omental infarct. The patient’s pain resolved in a few days with conservative therapy.
in the omentum with a subtle peripheral rim, in keeping with an omental infarct. The patient’s pain resolved in a few days with conservative therapy.
 with a peripheral hyperdense rim in the right omentum. The patient had experienced RLQ pain about 1 week earlier, and this was thought to be a subacute omental infarct.
with a peripheral hyperdense rim in the right omentum. The patient had experienced RLQ pain about 1 week earlier, and this was thought to be a subacute omental infarct.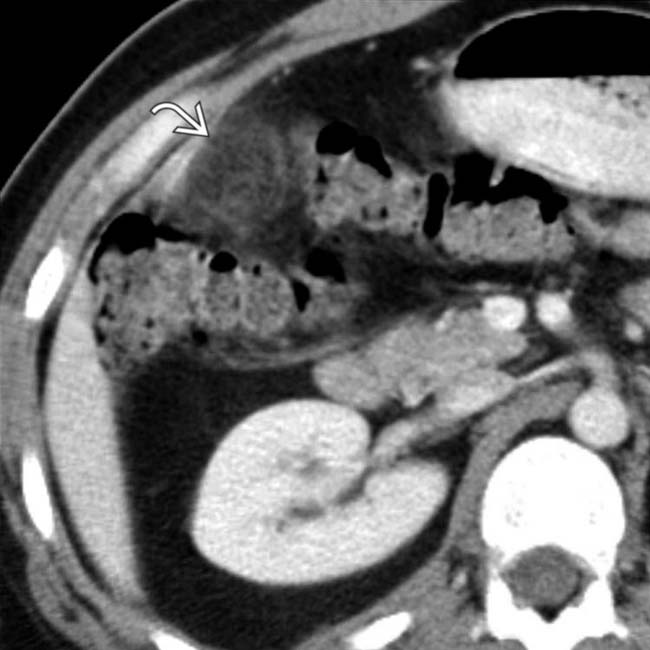
 with a hyperdense rim adjacent to the ascending colon.
with a hyperdense rim adjacent to the ascending colon.
 within the infarcted omentum, indicating twisting of the omental pedicle, which may be the etiology of the infarct in some cases.
within the infarcted omentum, indicating twisting of the omental pedicle, which may be the etiology of the infarct in some cases.




 Can have variable internal attenuation, but usually some internal foci of fat attenuation (-20 to -50 HU)
Can have variable internal attenuation, but usually some internal foci of fat attenuation (-20 to -50 HU) Usually well-circumscribed margins with peripheral hyperdense rim, particularly when occurring after surgery
Usually well-circumscribed margins with peripheral hyperdense rim, particularly when occurring after surgery























