• Protozoan (Cryptosporidium, Microsporidia, and Giardia)
Duodenum and jejunum, sparing distal SB and colon
Fold thickening without much submucosal edema
Excess fluid (luminal distention) of proximal small bowel
No ascites; uncommon lymphadenopathy
• Bacterial (Clostridium difficile colitis, Campylobacter, and others)
Segmental or, more commonly, pancolitis
Striking mucosal hyperenhancement and submucosal edema
Ascites (present in 40% of cases)
May progress to toxic megacolon or perforation
TOP DIFFERENTIAL DIAGNOSES
• Gastrointestinal lymphoma
CLINICAL ISSUES
• Prevalence of opportunistic GI infections in HIV patients has markedly decreased with potent antiretroviral therapy
DIAGNOSTIC CHECKLIST
• Specific diagnosis can be suggested by CT
• Diagnosis depends on microbiological confirmation by analysis of bowel content or even biopsy
(Left) This young woman has cystic fibrosis and lung transplantation, with new onset diarrhea. Axial CECT shows hyperenhancement and submucosal edema affecting most of the small bowel (SB).
(Right) Coronal CECT in the same patient shows the widespread enteritis with engorged mesenteric vessels . The colon is spared. Endoscopy and biopsy confirmed cytomegalovirus (CMV) enteritis.
(Left) This 35-year-old man with AIDS developed profuse diarrhea and abdominal pain. Axial CECT shows pancolitis with marked submucosal edema but no hyperenhancement of the mucosa.
(Right) Coronal CECT in the same patient shows more evidence of pancolitis , proven to be due to CMV, which may induce ischemic injury to both the SB and colon in immunocompromised patients.
TERMINOLOGY
Abbreviations
•
Synonyms
Definitions
• Symptomatic gastrointestinal (GI) infection of immunocompromised host by organisms that usually cause no or minor illness in immunocompetent individuals
IMAGING
General Features
• Best diagnostic clue
Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema
– Distribution: Small bowel (SB), colon > stomach, esophagus, rectum
Favors distal small bowel and colon
– Pattern CECT: Mucosal hyper- or hypoenhancement
Reflects active inflammation vs. ischemic necrosis
Deep ulcers may be transmural, causing mesenteric infiltration
– Pattern on upper GI series, small bowel series, or barium enema
Aphthoid erosions in earlier stages
Deep ulcers, even sinus tracts in later stages
– Barium studies and CT findings may mimic Crohn disease or ulcerative colitis
– Associated findings
Lymphadenopathy is very uncommon
Infiltration of mesenteric fat by transmural, deep ulceration
Mycobacterial
– Mycobacterium avium-intracellulare (MAI): Thickened SB folds with relatively little submucosal edema
Micronodular fold thickening on SB follow-through
– Tuberculosis (TB)
Favors ileocecal distribution
Wall thickening, luminal narrowing, ± obstruction
– Associated findings
Mesenteric lymphadenopathy, often with low density (caseation)
Exudative ascites (peritonitis)
Peritoneal and omental thickening (may mimic peritoneal carcinomatosis)
Most affected patients do not have overt lung disease
Protozoan (Cryptosporidium and Giardia)
– Distribution
Duodenum and jejunum
Ileum and colon are spared
– Pattern
Fold thickening without much submucosal edema
Excess fluid (luminal distention) of proximal small bowel
– Associated findings
No ascites nor lymphadenopathy
Bacterial (Clostridium difficile colitis, Campylobacter, and others)
– Distribution
Segmental or, more commonly, pancolitis
Terminal ileum affected uncommonly
Only gold members can continue reading. Log In or Register to continue



 Mycobacterium avium-intracellulare (MAI): Thickened SB folds with relatively little submucosal edema
Mycobacterium avium-intracellulare (MAI): Thickened SB folds with relatively little submucosal edema











 affecting most of the small bowel (SB).
affecting most of the small bowel (SB).
 . The colon
. The colon  is spared. Endoscopy and biopsy confirmed cytomegalovirus (CMV) enteritis.
is spared. Endoscopy and biopsy confirmed cytomegalovirus (CMV) enteritis.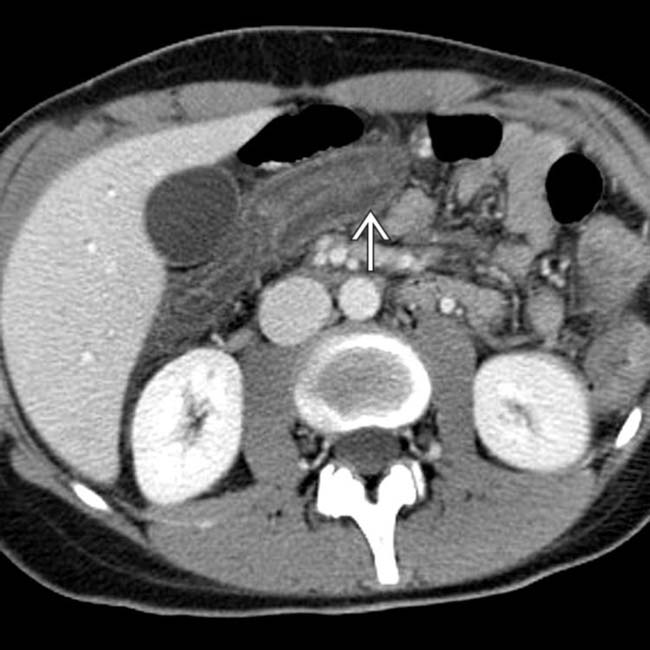
 but no hyperenhancement of the mucosa.
but no hyperenhancement of the mucosa.
 , proven to be due to CMV, which may induce ischemic injury to both the SB and colon in immunocompromised patients.
, proven to be due to CMV, which may induce ischemic injury to both the SB and colon in immunocompromised patients. Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema
Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema Mycobacterial
Mycobacterial Bacterial (Clostridium difficile colitis, Campylobacter, and others)
Bacterial (Clostridium difficile colitis, Campylobacter, and others)



























