– Enhancing septa predominate over cystic spaces, producing solid hyperenhancing lesion on imaging
• Peripheral rim enhancement on arterial or venous phase
• Calcifications common, and can be peripheral (most common), central, or along septations
• Does not typically result in biliary or pancreatic ductal obstruction or pancreatic atrophy
• MR able to better characterize internal morphology than CT, with ↑ sensitivity for microcysts
TOP DIFFERENTIAL DIAGNOSES
• Pancreatic pseudocyst
• Mucinous cystic pancreatic tumor
• Intraductal papillary mucinous neoplasm (IPMN)
• Pancreatic epithelial (true) cyst
• Pancreatic neuroendocrine tumors
CLINICAL ISSUES
• Many lesions (∼ 40%) are discovered incidentally in asymptomatic patients
• Often described as “grandmother tumor” due to preponderance in older women
• Vast majority are benign with no malignant potential
• Lesions measuring > 4 cm have been shown to grow more quickly and cause more symptoms
• Treatment
Asymptomatic small tumors with classic imaging features: Serial imaging follow-up
Indeterminate lesions without classic imaging appearance: MR or endoscopic ultrasound
Complete surgical excision for large tumors (especially > 4 cm) with mass effect or patient symptomatology
(Left) Graphic shows a mass in the pancreatic head. The mass has a sponge or “honeycomb” appearance and is characterized by innumerable small cysts, a central scar, and no obstruction of the pancreatic or bile duct.
(Right) Axial CECT in an elderly woman with vague abdominal pain shows a large lobulated mass in the pancreatic head. Note the sponge-like appearance with multiple cystic spaces surrounding an enhancing fibrous scar , typical of a serous cystadenoma.
(Left) Axial T2 FS MR of a pancreatic lesion thought to be indeterminate on CT (not shown) demonstrates a cystic mass composed of many tiny internal cysts, classic for a “microcystic” serous cystadenoma.
(Right) Endoscopic ultrasound of a serous cystadenoma demonstrates the characteristic multiple tiny cysts . Aspiration of the cyst contents revealed thin fluid with no cellular atypia or elevated tumor markers.
TERMINOLOGY
Synonyms
• Glycogen-rich, microcystic, or macrocystic serous adenoma
Definitions
• Benign pancreatic tumors lined by glycogen-rich cells that arise from acinar cells
Associated Syndromes
• Von Hippel-Lindau syndrome: Lesions may be multiple
IMAGING
General Features
• Best diagnostic clue
Honeycomb or sponge-like mass in pancreatic head
• Location
Classically thought to be more common in pancreatic head
Recent data suggests that lesions may be equally distributed throughout pancreas
• Size
Indolent lesions that can rarely become large masses
Range in size from 1-12 cm (mean 4-5 cm)
• Morphology
Well-circumscribed lesions with lobulated contour
Calcifications more common in serous than mucinous tumors (36% vs. 16%)
Radiographic Findings
CT Findings
• Well-circumscribed mass with lobulated contour and 3 primary morphologies





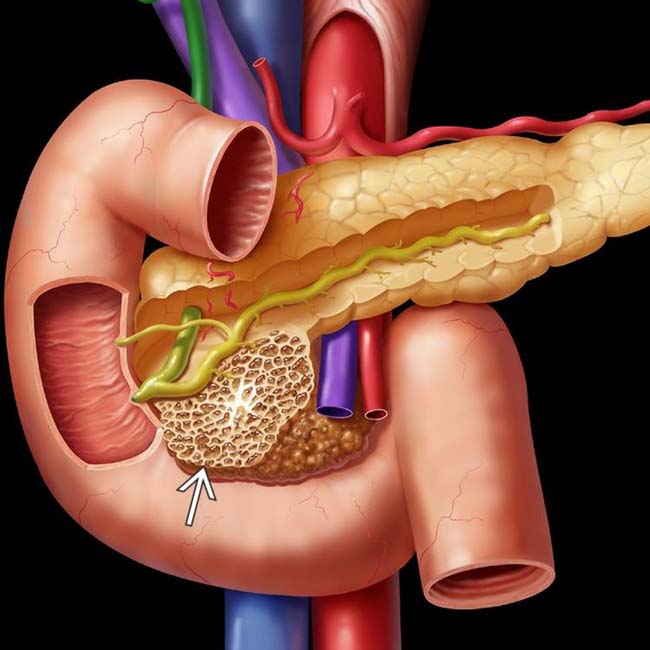
 in the pancreatic head. The mass has a sponge or “honeycomb” appearance and is characterized by innumerable small cysts, a central scar, and no obstruction of the pancreatic or bile duct.
in the pancreatic head. The mass has a sponge or “honeycomb” appearance and is characterized by innumerable small cysts, a central scar, and no obstruction of the pancreatic or bile duct.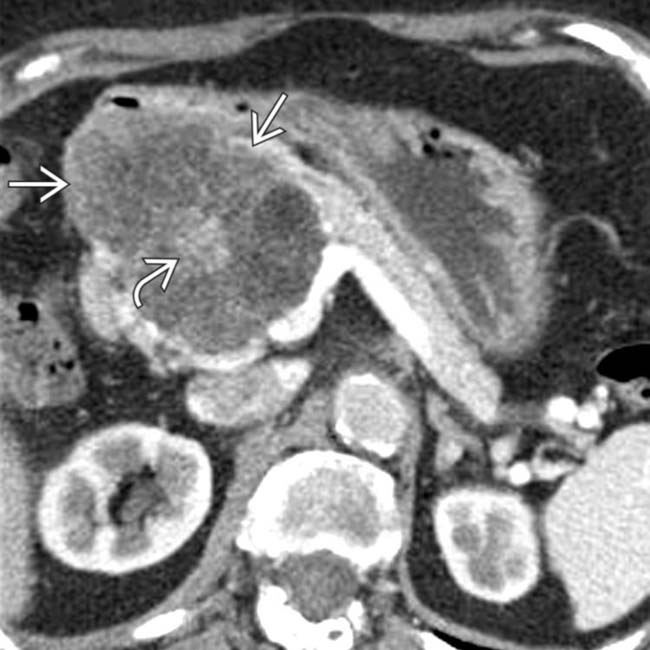
 in the pancreatic head. Note the sponge-like appearance with multiple cystic spaces surrounding an enhancing fibrous scar
in the pancreatic head. Note the sponge-like appearance with multiple cystic spaces surrounding an enhancing fibrous scar  , typical of a serous cystadenoma.
, typical of a serous cystadenoma.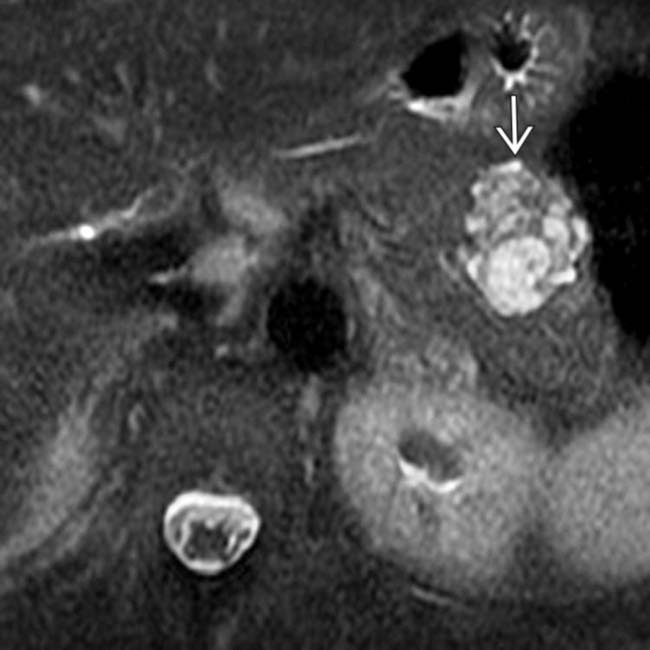
 composed of many tiny internal cysts, classic for a “microcystic” serous cystadenoma.
composed of many tiny internal cysts, classic for a “microcystic” serous cystadenoma.
 . Aspiration of the cyst contents revealed thin fluid with no cellular atypia or elevated tumor markers.
. Aspiration of the cyst contents revealed thin fluid with no cellular atypia or elevated tumor markers.






 Microcystic adenoma (i.e., classic serous cystadenoma)
Microcystic adenoma (i.e., classic serous cystadenoma)











