CT: Homogeneous soft tissue mass in right abdomen with adjacent suture line at duodenal stump
MR: Normal pancreatic parenchyma is isointense to renal cortex on T1WI and isointense to muscle on T2WI
US: Normal pancreas transplant homogeneous and hypoechoic to adjacent mesenteric fat
• Imaging of major complications
Allograft pancreatitis: Edema, enlargement and heterogeneous pancreas with peripancreatic fluid
Acute rejection: Enlargement and edema of graft with increased T2WI signal on MR
Chronic rejection: Small and atrophic graft with decreased T1 and T2WI signal on MR
Vascular complications: Venous thrombosis is more common than arterial
– Arterial thrombosis on US: No Doppler flow within artery or graft parenchyma
– Venous thrombosis on US: Echogenic intraluminal thrombus, absent vascular flow, and high-resistance arterial waveforms with reversed diastolic flow
– Graft infarction on US: Enlarged avascular transplant
Intraabdominal fluid collections: May represent abscess, seroma, lymphocele, urinoma, or pseudocyst
PATHOLOGY
• Goal of pancreas transplantation is treatment of diabetes by restoring endogenous insulin secretion
CLINICAL ISSUES
• Graft survival is better with combined pancreas-kidney transplant than with pancreas alone
• Graft pancreatitis is common after transplantation
35% experience mild, self-limited pancreatitis; usually related to reperfusion injury after surgery
• Chronic rejection is leading cause of late allograft loss
• Vascular thrombosis is 2nd leading cause of graft dysfunction (usually in acute postoperative setting)
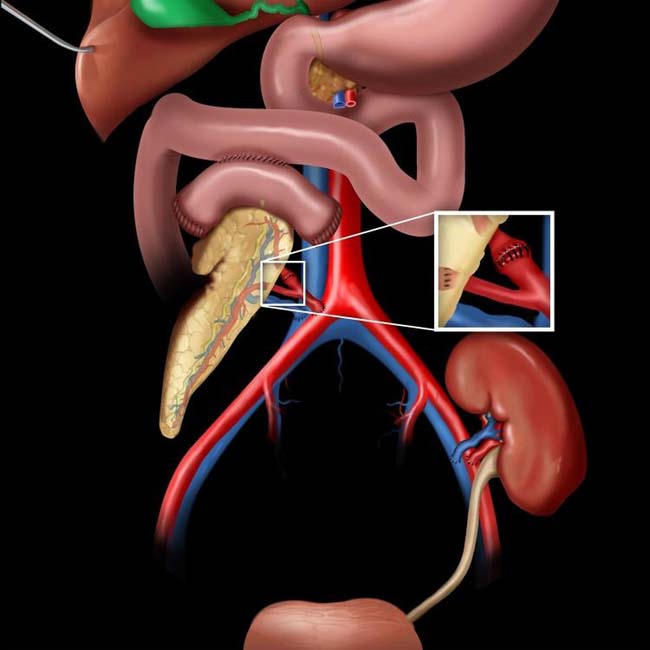
(Left) Graphic shows the usual surgical anatomy of a combined pancreas-kidney transplant with pancreatic-enteric drainage. The donor iliac artery is anastomosed to the donor superior mesenteric and splenic arteries to perfuse the pancreatic allograft (inset). The venous drainage can be to the iliac vein (as drawn) or the superior mesenteric vein.
(Right) Coronal MRA of a kidney-pancreas transplant reveals that the renal and the pancreatic allografts show normal perfusion and parenchymal enhancement.
(Left) Coronal NECT demonstrates the right lower quadrant transplant pancreas to be enlarged and hypodense with adjacent fat stranding and induration. Based on the CT findings, this could represent either graft ischemia or pancreatitis.
(Right) Sagittal power Doppler ultrasound in the same patient demonstrates the pancreatic transplant to be enlarged and diffusely hypoechoic, without appreciable internal vascularity, compatible with infarction.
IMAGING
General Features
• Location
80% are placed simultaneously with or following renal transplantation (Tx) for type 1 diabetes
– Pancreatic graft survival is increased with simultaneous transplantation
Pancreatic allograft usually placed on right side (renal allograft on left)
– Graft in bladder drainage transplants is usually in right iliac fossa, parallel to ascending colon
– Graft position in enteric drainage transplants is more variable, but usually vertical on right side
Multivisceral transplant
– Usually refers to transplantation of liver and small bowel
– If pancreas is also transplanted, it is often placed in upper abdomen, in transverse orientation
– Liver, bowel, and pancreas allografts all supplied by donor aortic graft
• Surgical technique
Bladder drainage
– Older technique that drains pancreatic secretions into bladder via duodenal interposition segment
– Associated with many complications, including accelerated insulin resistance, atherosclerosis, urinary tract infections, and graft pancreatitis
Enteric drainage
– Now considered preferred technique, with allograft head (which is obtained with segment of duodenum) placed in cephalic location with side-to-side pancreatic-duodenal to jejunal anastomosis
Venous drainage
– Donor portal vein anastomosed to systemic vein (common/external iliac or IVC) or mesenteric vein (more physiologic, but technically more difficult)
Arterial supply
– Donor iliac artery “Y” graft with one end anastomosed to recipient’s common, external, or internal iliac artery and “Y” limbs anastomosed to donor splenic and superior mesenteric arteries (end blindly after supplying allograft)
• Normal imaging appearance
CT: IV contrast often not used due to renal toxicity and concurrent chronic renal failure
– Oral contrast very useful (and usually necessary) to distinguish graft from adjacent bowel
– For bladder-drained allografts, can introduce contrast into bladder via catheter
– Homogeneous soft tissue mass closely associated with adjacent bowel (typically with adjacent suture line at duodenal stump)
– Graft may be normally enlarged and heterogeneous in early post-transplant period (< 4 weeks) with surrounding fluid and hematoma, and should not be confused with pancreatitis
Pancreas graft gradually becomes well defined and similar in density (on both NECT and CECT) to normal pancreas, with no surrounding fluid
MR: Normal pancreas parenchyma is isointense to renal cortex on T1WI and isointense to muscle on T2WI
• Imaging of major complications
Allograft pancreatitis: Edema, enlargement, and heterogeneous enhancement of pancreas on CT and MR, typically with peripancreatic fluid
– Peripancreatic fluid can evolve into loculated collections or pseudocysts
– May see bowel wall thickening of adjacent intestine
Acute rejection: Nonspecific CT findings, with enlargement and edema of graft
– MR: Increased parenchymal T2WI signal and heterogeneous enhancement due to edema
Chronic rejection: Nonspecific CT findings, with small and atrophic graft
– MR: Decreased signal intensity on T1 and T2 due to parenchymal fibrosis and reduced extracellular fluid
Secretin-augmented MR may demonstrate diminished exocrine function with ↓ secretion of pancreatic juice from dysfunctional allograft
Vascular complications: Venous thrombosis is more common than arterial
– MRA and CTA can map arterial and venous anatomy to identify sites of stenosis or thrombosis
More typically a troubleshooting tool when ultrasound findings are equivocal
Can be used to monitor anticoagulation therapy in patients with venous stump thrombosis
– Pseudoaneurysms and arteriovenous fistulae may be due to prior biopsy, pancreatitis, or surgical technique
– Graft infarction: Heterogeneous enhancement of pancreas on MR or CT ± liquefied/necrotic parenchyma ± gas bubbles
Impossible to distinguish infarction from infected pancreatic necrosis after pancreatitis, although treatment is same (surgical resection)
Ischemia or necrosis can affect graft focally or diffusely
Postoperative hemorrhage: May be visualized on routine postoperative US, but full extent (and presence of active extravasation) best seen with CECT
Intraabdominal fluid collections: May represent abscess, seroma, lymphocele, urinoma, or pseudocyst
– Presence of excessive extraluminal gas, fluid, or oral contrast should raise concern for leakage at enteric anastomosis
Post-transplant lymphoproliferative disorder (PTLD): New lymphadenopathy or solid masses in abdomen after transplant should raise suspicion
Radiographic Findings
• Radiography
Normal pancreatic transplant: Vague lower quadrant soft tissue density (usually in right lower quadrant) with 2 or 3 rows of staples
– Stapled ends of duodenum, plus side-to-side anastomosis to jejunum (or bladder)
Only gold members can continue reading. Log In or Register to continue
 MR: Normal pancreatic parenchyma is isointense to renal cortex on T1WI and isointense to muscle on T2WI
MR: Normal pancreatic parenchyma is isointense to renal cortex on T1WI and isointense to muscle on T2WI
 Vascular complications: Venous thrombosis is more common than arterial
Vascular complications: Venous thrombosis is more common than arterial





 and the pancreatic allografts
and the pancreatic allografts  show normal perfusion and parenchymal enhancement.
show normal perfusion and parenchymal enhancement.
 to be enlarged and hypodense with adjacent fat stranding and induration. Based on the CT findings, this could represent either graft ischemia or pancreatitis.
to be enlarged and hypodense with adjacent fat stranding and induration. Based on the CT findings, this could represent either graft ischemia or pancreatitis.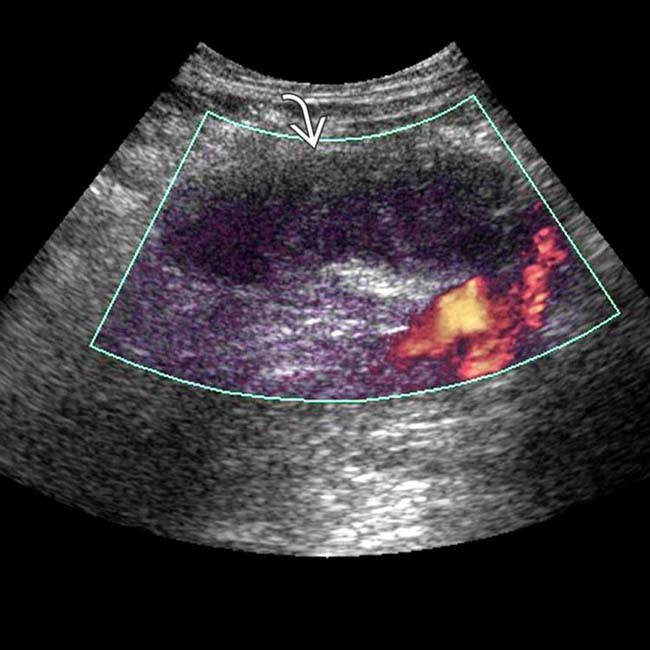
 to be enlarged and diffusely hypoechoic, without appreciable internal vascularity, compatible with infarction.
to be enlarged and diffusely hypoechoic, without appreciable internal vascularity, compatible with infarction. Pancreatic allograft usually placed on right side (renal allograft on left)
Pancreatic allograft usually placed on right side (renal allograft on left)





 CT: IV contrast often not used due to renal toxicity and concurrent chronic renal failure
CT: IV contrast often not used due to renal toxicity and concurrent chronic renal failure

 Allograft pancreatitis: Edema, enlargement, and heterogeneous enhancement of pancreas on CT and MR, typically with peripancreatic fluid
Allograft pancreatitis: Edema, enlargement, and heterogeneous enhancement of pancreas on CT and MR, typically with peripancreatic fluid Vascular complications: Venous thrombosis is more common than arterial
Vascular complications: Venous thrombosis is more common than arterial Postoperative hemorrhage: May be visualized on routine postoperative US, but full extent (and presence of active extravasation) best seen with CECT
Postoperative hemorrhage: May be visualized on routine postoperative US, but full extent (and presence of active extravasation) best seen with CECT








 Normal pancreatic transplant: Vague lower quadrant soft tissue density (usually in right lower quadrant) with 2 or 3 rows of staples
Normal pancreatic transplant: Vague lower quadrant soft tissue density (usually in right lower quadrant) with 2 or 3 rows of staples





