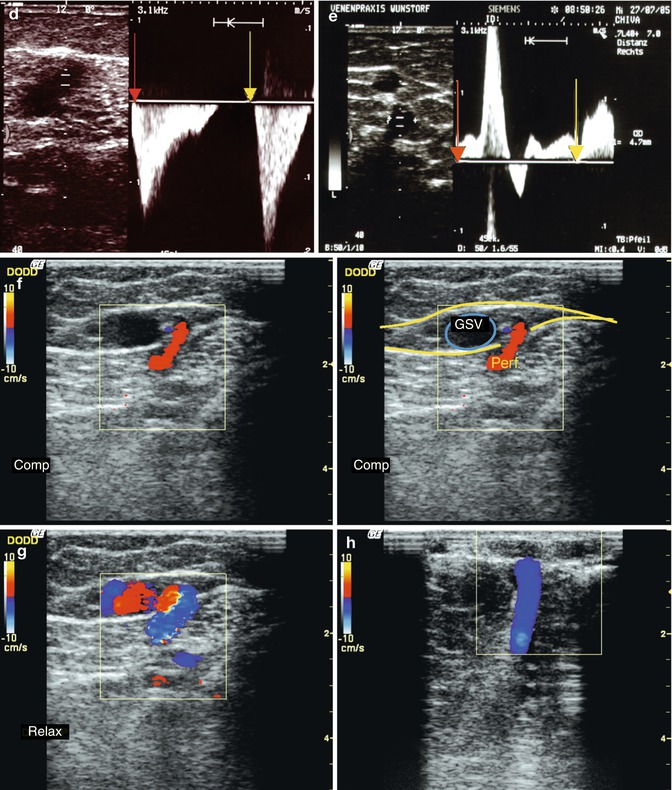
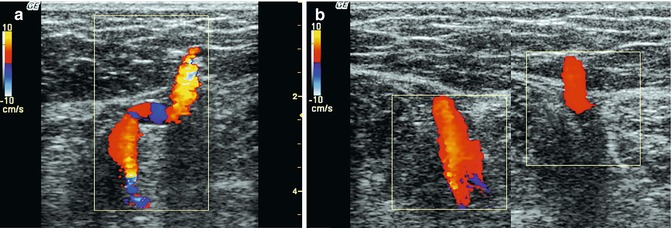
Fig. 9.1
Blood flow in perforating veins under provocation manoeuvres; red arrow, start of muscular systole; yellow arrow, start of muscular diastole; above baseline, outward reflux; and below baseline, antegrade inward flow. (a) Flow in a grossly dilated paratibial perforating vein with an incompetent great saphenous vein. The blood flows through this perforating vein to the deep vein. This results from secondary dilation, not primary incompetence. (b) Flow in a grossly dilated paratibial perforating vein to the deep vein with an incompetent great saphenous vein. The inward flow results from secondary dilatation, not primary incompetence. (c) Flow in the posterior tibial perforating vein (formerly Cockett 2). The volume which flows outwards during muscular systole appears to be greater than the inward re-entry volume. This subject had severe varicose veins with secondary deep vein incompetence. However, since the diastolic blood flow is still inwards, drainage must be initially through a perforating vein dilated by the reflux volume, which is not in itself incompetent. In procedures which eliminate the reflux source, it is possible to wait before treating this vein. Once the recirculation has been eliminated, it will become apparent whether the perforating vein recovers its normal calibre or must be interrupted. (d) A muscle vein in the calf at the end of a varicose tributary. The blood flows inwards towards the deep veins during both muscular systole and diastole. This perforating vein has bidirectional flow from secondary dilatation; it is not primarily a refluxive vein. (e) Distal perforating vein of the adductor canal (formerly Hunter) as a proximal reflux source of a recirculation. Outward flow occurs during both muscular systole and diastole. This is a clear diagnosis of an incompetent perforating vein. (f) Transverse view through the inner thigh showing the perforating vein of the adductor canal (formerly Dodd) joining the side of the great saphenous vein. The perforating vein appears refluxive in calf muscle systole with outward flow (red in colour duplex). Manual compression of the calf causes an increase in pressure in the deep veins driving blood through the perforating vein in the relaxed musculature of the thigh and then into the superficial veins (online material). (g) Relaxation phase in the same subject as in (f) demonstrating flow reversal. Inward flow from the refluxive great saphenous vein via the perforating vein into the deep vein. The perforating vein is not a reflux source for recirculation, but a re-entry drainage point. (h) Transverse view through the inside of the calf demonstrating a dilated paratibial perforating vein (formerly Boyd) with incompetence of the great saphenous vein (GSV), above and below the knee. There is distal drainage through the perforating veins of the posterior tibial veins (formerly Cockett group). The Wunstorf manoeuvre is demonstrated by the film sequences on the online material which show inward flow during muscular diastole. Colour artefacts are observed during muscular contraction which are unavoidable as the musculature is moving in the image. The flow after prolonged standing can also be seen with small volumes of blood flowing from the deep to the superficial system. This indicates that there is a re-entry perforating vein
Copyright: [Author]
The flow after muscle relaxation is essential for diagnosis (Fig. 9.1). All perforating veins should be assessed during muscular diastole. If there is outward flow during diastole, the perforating vein is incompetent (Fig. 9.1e). However, it is more common to find a higher pressure in the incompetent superficial vein than in the deep vein after muscular contraction. In this case, the blood flows inwards through the dilated perforating vein during diastole (Fig. 9.1b–d). Further studies have to enlighten the direction taken by the blood before and after flow through a perforating vein. For example, these interactions could be out and up, out and down, up and in and down and in, depending on the situation. This may help also to identify whether the perforating vein acts as a source of reflux or a re-entry point. Outward and upward flow, for example, may be less detrimental than outward and downward flow. The extent this has on therapeutic decisions needs further investigation.
The practice of applying a tourniquet above the perforating vein in order to measure its flow under manual compression and decompression may give a false pathological result. If the incompetent vein is occluded above the perforating vein by the tourniquet, the refluxive recirculation downwards will not occur in diastole. However, a perforating vein which is dilated by recirculation is often in contact with an incompetent vein further down. After decompression, the blood will flow out of the deep veins, through the dilated perforating vein and into the incompetent distal segment of the superficial vein. A vein thus appears incompetent which under physiological conditions (without the tourniquet) serves as a re-entry point.
9.3.1 Perforating Veins as Sources of Recirculation
Diastolic reflux or outward flow during muscular diastole is a sine qua non for describing a perforating vein as a reflux source.
The further down the leg, the less likely a perforating vein is to serve as the reflux source for a recirculation. The only exception is secondary varices after trauma to the calf which may occur with periosteal injuries to the tibia (Sect. 9.10). It is not unusual to find a single refluxive muscle vein after trauma, for example, in footballers. These fill varicose tributaries and form a proximal source of reflux. The proximal reflux source is often the proximal perforating veins of the adductor canal (formerly Dodd) (Fig. 9.2), less often the distal perforating vein of the adductor canal (formerly Hunter; Fig. 9.1e) and very rarely the proximal paratibial perforating veins (formerly Boyd; Figs. 9.3 and 7.48). The latter are more often refluxive with secondary varices arising from reflux in the deep axis above the posterior tibial vein.
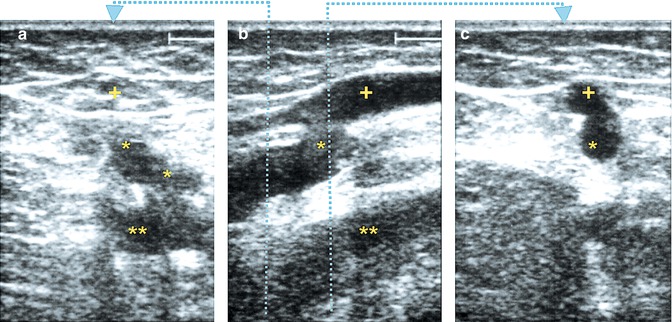
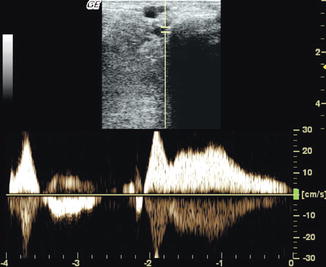
Fig. 9.2
(a) Transverse view through a competent great saphenous vein (+) in the mid thigh. Beneath it, an incompetent perforating vein of the adductor canal (formerly Dodd) is seen connecting to the femoral vein (**). (b) Longitudinal view at the junction of the perforating vein with the great saphenous vein which becomes refluxive and dilated. The perforating vein typically arises from the deep system and courses downwards. (c) Junction of the perforating vein and the great saphenous vein in transverse view (dotted line in b: section levels for a and c)
Copyright: [Author]
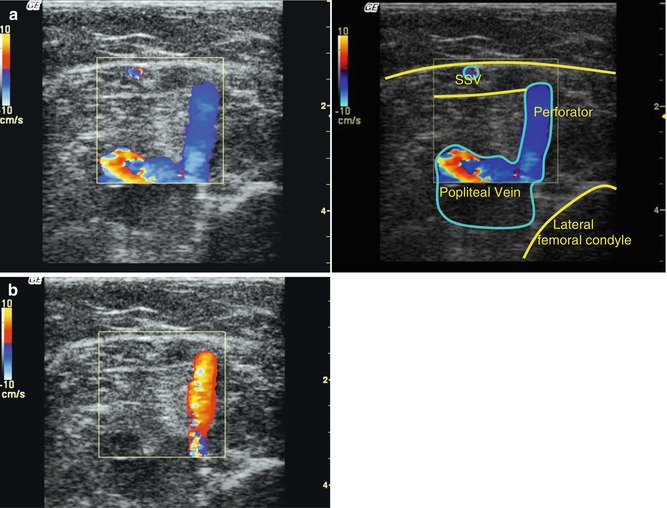
Fig. 9.3
Transverse view through the upper third of the left calf demonstrating an incompetent proximal paratibial perforating vein (formerly Boyd). The perforating vein is dilated and acts as a reflux source for the great saphenous vein. Note the outward flow during calf diastole
Copyright: [Author]
Incompetent muscle veins may be the source for subcutaneous reticular varices on the back and lateral or medial aspect of the calf (Fig. 9.4 and Sect. 9.9). These frequently develop after trauma. A perforating vein in the back of the thigh may be incompetent, refluxing into the Giacomini anastomosis or a varicose tributary (Fig. 9.5). Occasionally, a perforating vein arising directly from the popliteal vein may be found near the saphenopopliteal junction or slightly further proximal (Fig. 9.6).
Get Clinical Tree app for offline access
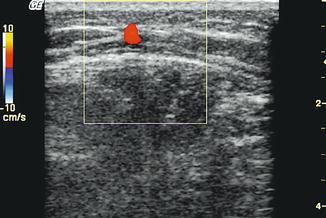
Fig. 9.4
Transverse view through the back of the left thigh. A small-calibre, refluxive perforating vein is seen emerging from the muscle fascia to fill a subcutaneous reticular network. Subcutaneous treatments of reticular veins are less likely to succeed in the presence of a feeding perforating vein unless this is also treated
Copyright: [Author]
Fig. 9.5
(a) Longitudinal view through the back of the thigh in a patient with a visible varicose tributary above the knee. A large, refluxive perforating vein is seen with duplex running distally for a short distance under the muscle fascia and then piercing the fascia and filling the tributary (online material). (b) Transverse view of the same perforating vein; left (further proximal) where it is still deep, right (further distal) where it pierces the fascia to become superficial
Copyright: [Author]
Fig. 9.6
Transverse view through the right popliteal region. The saphenopopliteal junction is 10 cm higher up. A large perforating vein is seen arising from the popliteal vein and refluxing into a (not shown) subcutaneous varicosity. (a) During muscular systole, there is antegrade flow in small saphenous vein and inward flow in the perforating vein. (b




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
