Grows along bile ducts and is elongated, spiculated, or branch-like
• Progressive, gradual, and concentric filling (centripetal) on delayed phase images
Usually not isodense to vessels (unlike hemangioma)
• Substantial delayed enhancement (i.e., greater than that of liver parenchyma) is common (74%)
Attributed to fibrous stroma in CCA
• ± capsular retraction (frequent), with parenchymal atrophy of liver segments peripheral to tumor
• Bile ducts will be dilated upstream from tumor
Duct lining may be thickened and enhanced
Rare with other types of hepatic tumors
TOP DIFFERENTIAL DIAGNOSES
• Hepatic metastases and lymphoma
• Hepatocellular carcinoma
• Focal confluent fibrosis
PATHOLOGY
• Based on growth characteristics
Mass forming (exophytic/nodular); most common form
Periductal infiltrating (sclerosing)
Intraductal growing (polypoid/papillary)
CLINICAL ISSUES
• Only minority of cholangiocarcinomas are peripheral type
• Large size at presentation contributes to poor prognosis
(Left) Intrahepatic cholangiocarcinomas generally arise in noncirrhotic livers. This gross photograph shows a white-tan, firm, and distinct mass in a background of noncirrhotic liver. (Courtesy M. Yeh, MD, PhD.)
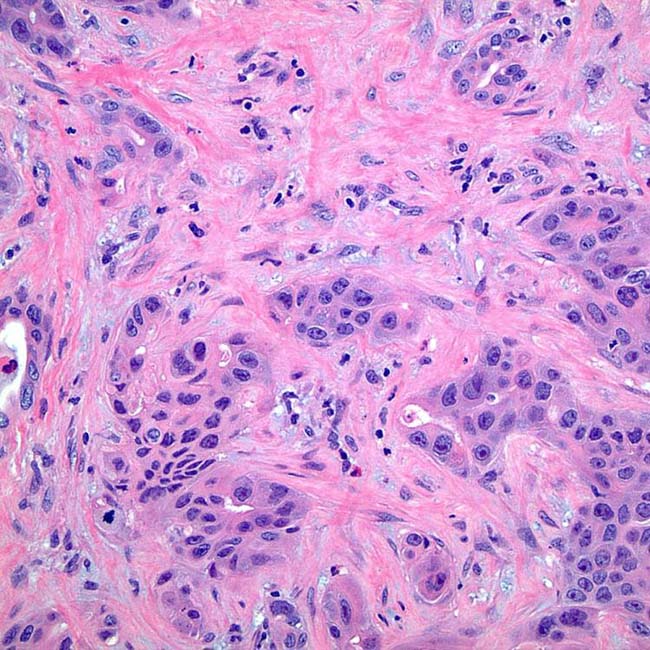
(Right) Desmoplastic stroma is a common finding in intrahepatic cholangiocarcinoma. (Courtesy M. Yeh, MD, PhD.)
(Left) Axial CECT of a 46-year-old woman with jaundice shows the portal vein and bile ducts encased and obstructed by the tumor , accounting for the altered perfusion of the right hepatic lobe. Hepatic veins were encased as well, resulting in collateral blood vessels seen within the right lobe .
(Right) Axial 10-minute delayed CECT in the same patient shows heterogeneous, persistent enhancement of the tumor , a feature of cholangiocarcinoma (and other tumors with fibrous stroma).












 and bile ducts
and bile ducts  encased and obstructed by the tumor
encased and obstructed by the tumor  , accounting for the altered perfusion of the right hepatic lobe. Hepatic veins were encased as well, resulting in collateral blood vessels seen within the right lobe
, accounting for the altered perfusion of the right hepatic lobe. Hepatic veins were encased as well, resulting in collateral blood vessels seen within the right lobe  .
.
 , a feature of cholangiocarcinoma (and other tumors with fibrous stroma).
, a feature of cholangiocarcinoma (and other tumors with fibrous stroma).







 Mass-forming PCC
Mass-forming PCC








 Dynamic MR: Minimal or moderate rim enhancement and progressive and concentric filling with contrast material
Dynamic MR: Minimal or moderate rim enhancement and progressive and concentric filling with contrast material






