Ascites may be slightly higher in attenuation (15-30 HU) on CT than simple ascites
Internal complexity within ascites fluid (septations, debris) is common and easier to appreciate on MR or US
• Smooth thickening and hyperenhancement of peritoneum
Smooth peritoneal thickening and hyperenhancement does not always suggest peritonitis: Can be iatrogenic (after surgery or other intervention which irritates peritoneal lining) or in earliest stages of carcinomatosis (more commonly nodular and irregular, rather than smooth)
• Infiltration and fat stranding within mesentery/omentum
• Presence of ectopic gas suggests either hollow viscus perforation or gas-forming infection
• Other imaging findings may reveal cause of peritonitis (i.e., diverticulitis, appendicitis, low-attenuation nodes in TB)
• In chronic setting peritoneal lining may be thickened with smooth, curvilinear calcification
Most common in sclerosing peritonitis due to chronic peritoneal dialysis: Frequently described as “abdominal cocoon” due to peritoneal thickening and calcification
TOP DIFFERENTIAL DIAGNOSES
• Peritoneal carcinomatosis
• Benign ascites
• Pseudomyxoma peritonei
• Hemoperitoneum
PATHOLOGY
• Innumerable different causes including spontaneous bacterial peritonitis in cirrhotic patients, bowel perforation, gastrointestinal infections, TB, trauma, surgery, etc.
• Peritonitis does not necessarily always imply infection: Sterile peritonitis also possible
Sclerosing encapsulating peritonitis: Chronic form of peritoneal inflammation most often due to peritoneal dialysis resulting in severe fibrotic thickening of both visceral and parietal peritoneum
(Left) Axial CECT in a cirrhotic patient with spontaneous bacterial peritonitis demonstrates loculated ascites with enhancement and thickening of the parietal and visceral peritoneum . There are bilateral drains in place.
(Right) Axial CECT in a patient on chronic peritoneal dialysis with constant symptoms of bowel obstruction shows loculated ascites with thickened, enhancing parietal/visceral peritoneum encasing the small bowel and creating functional obstruction. Note the dilated segments of bowel .
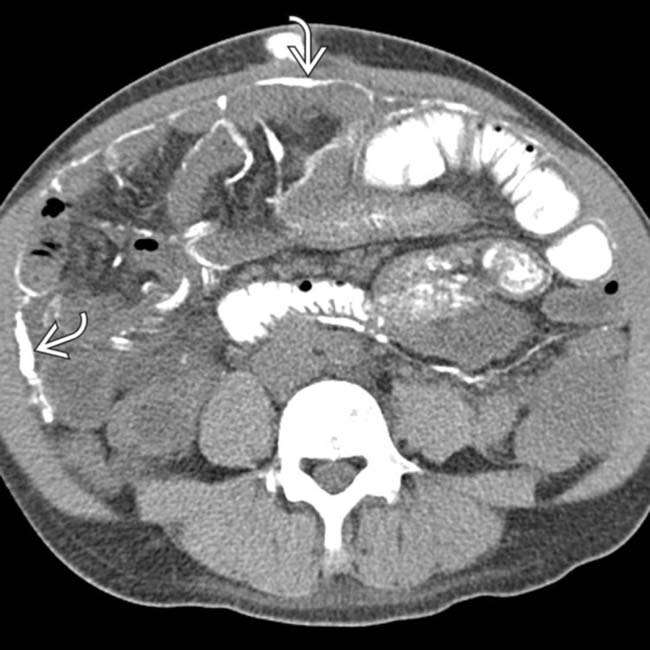
(Left) Axial NECT in a patient with a history of peritoneal dialysis demonstrates extensive calcifications and thickening of the peritoneal lining.
(Right) Axial NECT in the same patient demonstrates even more dramatic calcification surrounding bowel loops in the pelvis. These findings are classic for sclerosing peritonitis, most typically seen in patients on chronic peritoneal dialysis.
TERMINOLOGY
Definitions
• Infectious or inflammatory process involving peritoneum or peritoneal cavity
IMAGING
General Features
• Best diagnostic clue
Ascites and omental/mesenteric fat stranding with symmetric, smooth enhancement and thickening of peritoneal lining
• Location
Peritoneal surface, mesentery, and omentum
• Size
May be localized or generalized in peritoneal cavity
• Morphology
Symmetric, smooth thickening and enhancement of peritoneum
CT Findings
• Ascites ± loculated fluid collections or discrete abscess
Ascites may be slightly higher in attenuation (15-30 Hounsfield units) than simple ascites, but lower in attenuation than hemoperitoneum
• Smooth, regular thickening and enhancement of peritoneum (can be either localized adjacent to site of inflammation or generalized throughout abdomen)
Smooth peritoneal thickening and enhancement does not always suggest peritonitis
– Can be iatrogenic (after surgery or other intervention that irritates peritoneal lining) or appear in earliest stages of carcinomatosis (more commonly nodular and irregular, rather than smooth)
• Infiltration and fat stranding within mesentery and omentum (either localized or generalized)
• Presence of ectopic gas suggests either hollow viscus perforation or gas-forming infection
• Other imaging findings may reveal cause of peritonitis (i.e., diverticulitis, appendicitis, low-attenuation nodes in tuberculous peritonitis)
• In chronic setting (usually after multiple bouts of peritonitis) peritoneal lining may be thickened with smooth, curvilinear calcification and encapsulation/tethering of bowel loops
Classically seen in sclerosing peritonitis as result of chronic peritoneal dialysis
– Extensive peritoneal thickening and calcification may result in frequent small bowel obstructions
MR Findings
• Presence of ascites (low signal on T1WI and high signal on T2WI)
± loculated fluid collections or discrete abscesses with peripheral enhancement
Septations and complexity within ascites fluid may be present and best appreciated on T2WI
• Smooth thickening and enhancement of peritoneal lining on T1WI C+ images
May be localized or generalized depending on site and extent of infection/inflammation
• Thickening and inflammation of omentum and mesentery (generally high signal on T2WI)
Ultrasonographic Findings
• Peritoneal free fluid ± evidence of loculation or complexity (internal septations, debris, hemorrhage, etc.)
• Omental and mesenteric fat may appear echogenic and hyperemic on color Doppler US as result of inflammation, particularly adjacent to primary source of infection/inflammation
• Ultrasound may be best tool along with MR for diagnosing many pelvic sources of peritonitis
i.e., dilated fallopian tube with fluid-debris level (pyosalpinx) or complex adnexal cystic masses (tubo-ovarian abscesses [TOAs]) in pelvic inflammatory disease (PID)
Radiographic Findings
• Radiography
Evidence of ascites: > 500 mL required for plain film diagnosis
– Flank bulging
– Indistinct psoas margin
– Small bowel (SB) loops floating centrally
– Lateral edge of liver displaced medially (Hellmer sign): Visible in 80% of patients with significant ascites
– Pelvic “dog’s ear” present in 90% of patients with significant ascites
– Medial displacement of cecum and ascending colon present in 90% of patients with significant ascites
± free air (usually in cases with hollow viscus perforation or gas-forming infection)
Hydropneumoperitoneum
Air in lesser sac with perforated gastric ulcer
Imaging Recommendations
• Best imaging tool
CECT
• Protocol advice
DIFFERENTIAL DIAGNOSIS
Peritoneal Carcinomatosis
• Metastatic disease to omentum, peritoneum, or mesentery (most commonly ovarian cancer and gastrointestinal malignancies)
• Ascites with nodularity, thickening, and induration of omentum (± discrete mass-like peritoneal implants)
Several patterns possible, including micronodular pattern, nodular pattern (more discrete nodules measuring > 5 mm), and omental caking (coalescence of omental metastases into larger conglomerate masses)
Only gold members can continue reading. Log In or Register to continue
 Internal complexity within ascites fluid (septations, debris) is common and easier to appreciate on MR or US
Internal complexity within ascites fluid (septations, debris) is common and easier to appreciate on MR or US



 . There are bilateral drains
. There are bilateral drains  in place.
in place.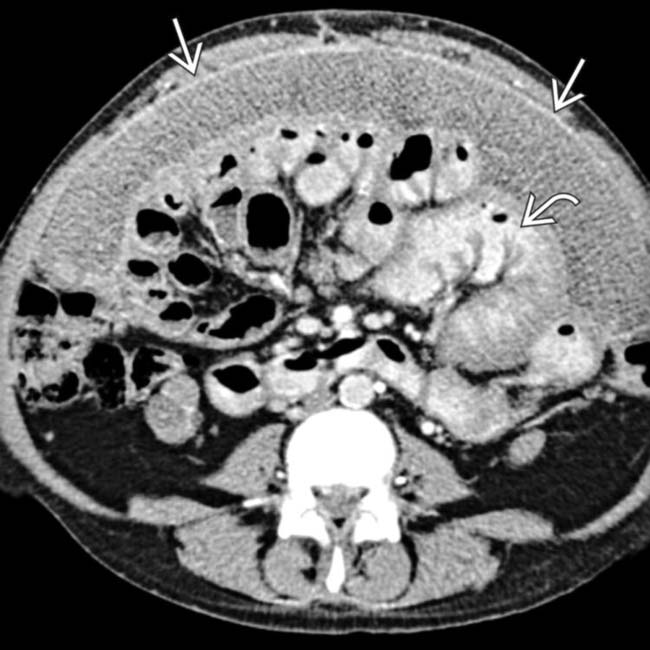
 with thickened, enhancing parietal/visceral peritoneum encasing the small bowel and creating functional obstruction. Note the dilated segments of bowel
with thickened, enhancing parietal/visceral peritoneum encasing the small bowel and creating functional obstruction. Note the dilated segments of bowel  .
.
 and thickening of the peritoneal lining.
and thickening of the peritoneal lining.
 surrounding bowel loops in the pelvis. These findings are classic for sclerosing peritonitis, most typically seen in patients on chronic peritoneal dialysis.
surrounding bowel loops in the pelvis. These findings are classic for sclerosing peritonitis, most typically seen in patients on chronic peritoneal dialysis.
















 Several patterns possible, including micronodular pattern, nodular pattern (more discrete nodules measuring > 5 mm), and omental caking (coalescence of omental metastases into larger conglomerate masses)
Several patterns possible, including micronodular pattern, nodular pattern (more discrete nodules measuring > 5 mm), and omental caking (coalescence of omental metastases into larger conglomerate masses)






