(1)
Department of Radiology, John H Stroger Jr Hospital of Cook County, Chicago, IL, USA
Diagnosis
Tension Pneumothorax
Imaging Features
1.
Plain chest radiograph shows hyperexpanded hemithorax with no lung markings and deep sulcus sign.
2.
The ipsilateral lung is collapsed and the diaphragm depressed.
3.
A few linear strands extend from the collapsed lung to the thoracic wall due to fibrotic adhesions.
4.
The mediastinum is shifted to the contralateral side.
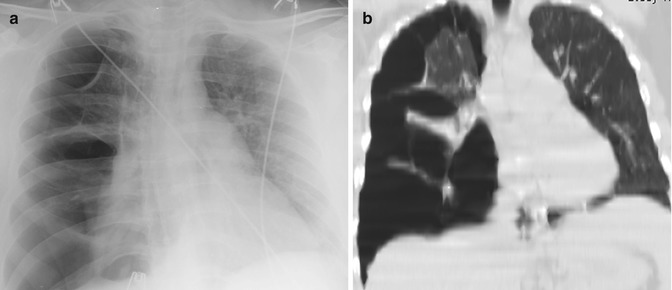
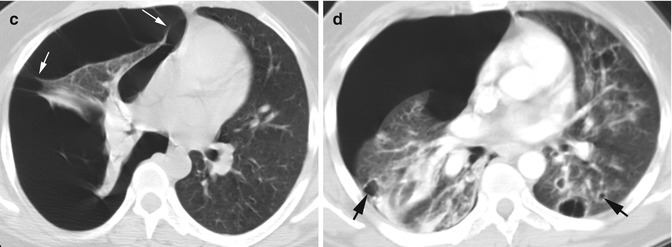
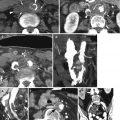
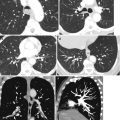
Fig. 9.1
Tension pneumothorax. (a–c) A patient with asthma experienced sudden shortness of breath. (a) Chest AP view and (b) coronal reformatted and (c) axial CT show shift of the mediastinum to the left and a deeper right costophrenic angle. The collapsed right lung shows multiple linear adhesions to the thoracic wall (arrows). (d) Axial CT of a patient with cystic pneumocystis infection shows right tension pneumothorax. Multiple cystic lesions (arrows) are seen bilaterally
Diagnosis
Empyema
Imaging Features
1.
Large fluid and gas collection in the pleural space
2.
Split pleural sign with enhancing pleura
3.
Compressive collapse of the adjacent lung
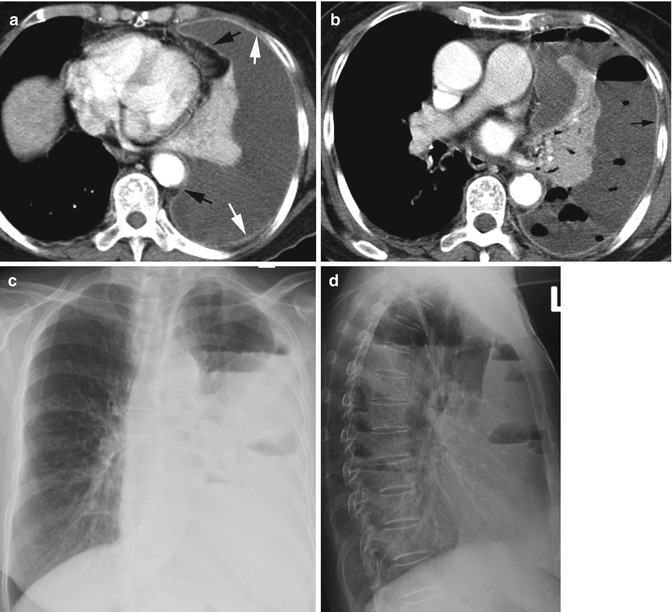
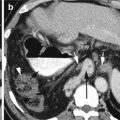
Fig. 9.2
Empyema. (a) Contrast-enhanced axial CT shows large pleural fluid surrounded by enhancing pleura with split pleural sign of parietal pleura (white arrows) and visceral pleura (black arrows). The left lung is collapsed. (b) Axial CT of the chest and (c, d) chest x-ray PA and lateral views 1 week later show development of gas collections in the pleural fluid with air-fluid levels. The pleura is still thick and enhancing (arrow in b)
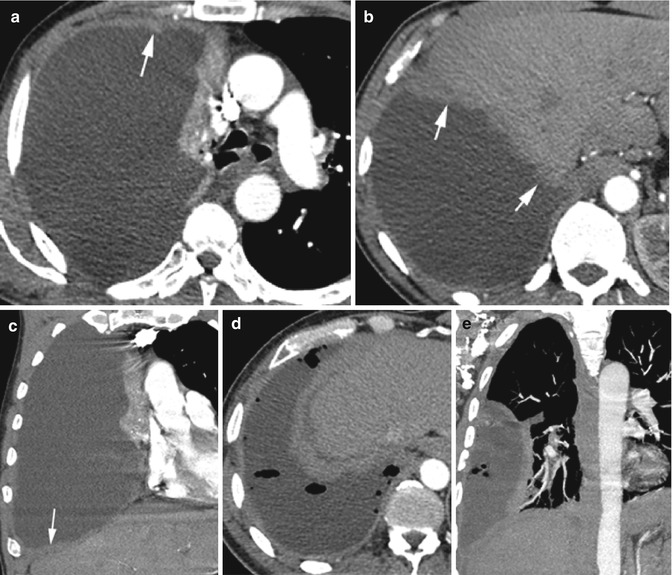
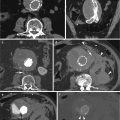
Fig. 9.3




Pleural mesothelioma with TB infection and biopsy-confirmed noncaseating granulomas. Axial (a, b) and coronal reformatted (c) CTs show irregular and nodular thickening of the visceral and parietal pleura (arrows) with enhancement similar to the intercostal muscles and liver. (d, e) Axial and coronal reformatted images show hydropneumothorax from biopsy
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
