Color Doppler US initially: Highly accurate and cost effective
CT or MR: Complete evaluation and to search for cause
TOP DIFFERENTIAL DIAGNOSES
• Streaming artifact
• Extrinsic compression
• Budd-Chiari syndrome
PATHOLOGY
• Most often associated with hepatic cirrhosis and pancreatitis
• Primary PV thrombosis may be 1st sign of hypercoagulable (prothrombotic) condition
CLINICAL ISSUES
• PV tumor invasion (usually from hepatocellular carcinoma) is associated with poor clinical outcome
• Primary PV thrombosis may mimic cirrhosis
Results in dysmorphic and malfunctioning liver
• Treatment: Anticoagulation for acute bland thrombosis or hypercoagulable condition
Add antibiotics for septic thrombophlebitis
DIAGNOSTIC CHECKLIST
• Tumor thrombus expands lumen, enhances, and is contiguous with parenchymal mass
• Thrombosis or fibrosis of extrahepatic portal vein may complicate or preclude liver transplantation
(Left) Axial CECT in a 55-year-old man with hepatitis B who presented for routine CT screening to rule out HCC shows cavernous transformation of the portal vein with numerous small collateral veins in the porta hepatis and hepatoduodenal ligament. The main portal vein cannot be identified.
(Right) CT through the porta hepatis in the same patient reveals no normal portal vein branches, only innumerable tiny collateral veins , diagnostic of cavernous transformation and chronic portal vein occlusion.
(Left) Longitudinal grayscale ultrasound image obtained through the porta hepatis in a 51-year-old woman presenting with vague RUQ pain and a recent elevation of liver function tests reveals no apparent abnormalities of the portal vein .
(Right) Longitudinal power Doppler ultrasound obtained in the same patient in the same field of view reveals an acute thrombosis of the portal vein with a complete absence of flow, which was undetectable with grayscale sonography alone.
TERMINOLOGY
Synonyms
• Portal vein thrombosis (PVT)
Definitions
• Acute, chronic, or neoplastic occlusion of portal vein (PV) due to thrombosis or tumor invasion
• Chronic PV occlusion with numerous periportal collaterals is referred to as “cavernous transformation”
IMAGING
General Features
• Best diagnostic clue
Low-attenuation thrombus in PV on CECT
On MR and power Doppler
– Absence of blood flow or flow void in PV
May be caused by slow flow in portal hypertension
– Nonvisualization of PV (chronic occlusion)
– Cavernous transformation of PV (collateralization in porta hepatis)
• Location
May involve any portion of intra- or extrahepatic PV
CT Findings
• CECT of acute thrombosis
Arterial phase (25-40 seconds post bolus injection)
– High attenuation within involved hepatic lobe or segment due to arterioportal shunting



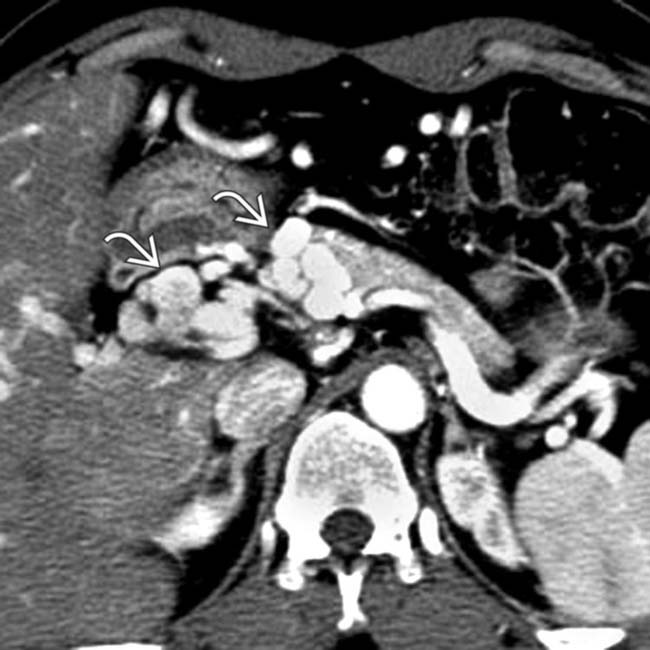
 in the porta hepatis and hepatoduodenal ligament. The main portal vein cannot be identified.
in the porta hepatis and hepatoduodenal ligament. The main portal vein cannot be identified.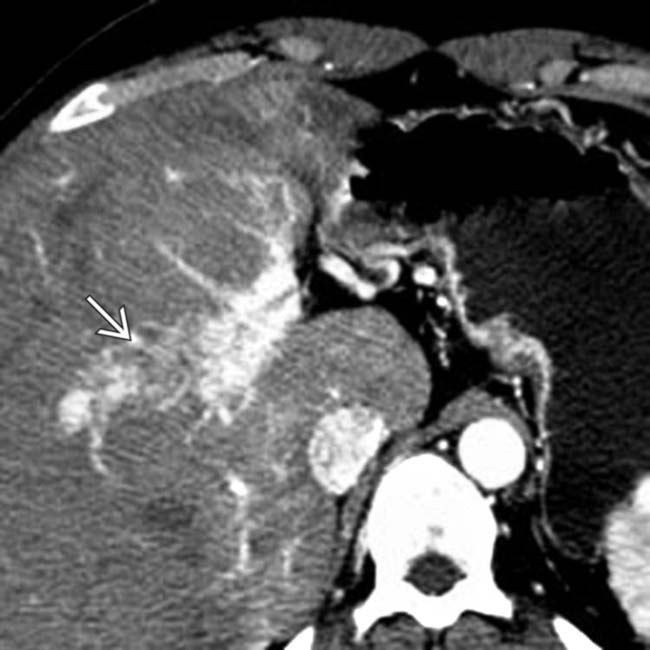
 , diagnostic of cavernous transformation and chronic portal vein occlusion.
, diagnostic of cavernous transformation and chronic portal vein occlusion.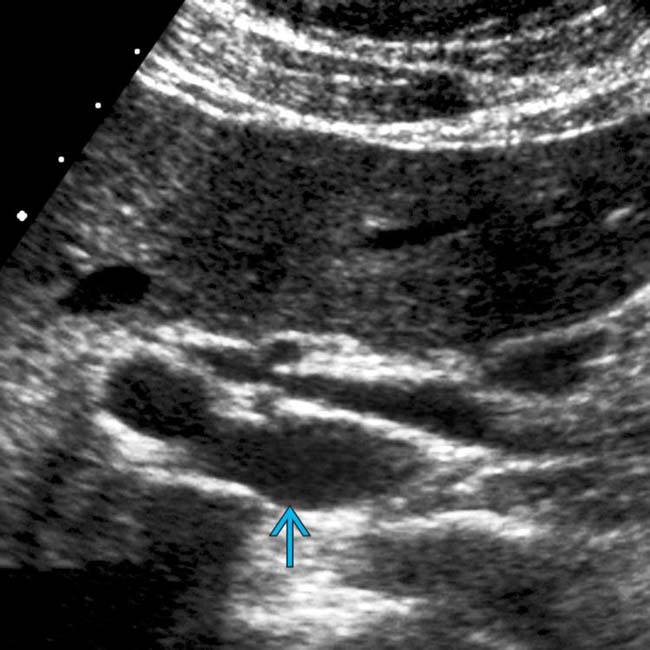
 .
.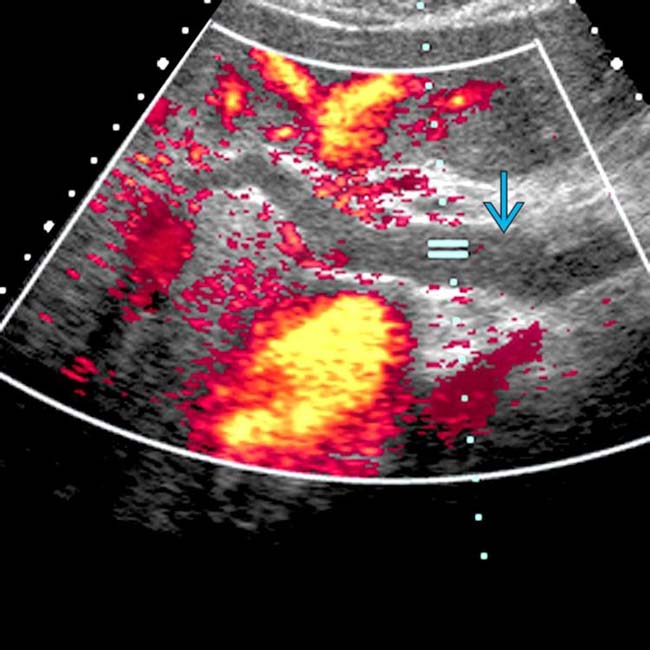
 of the portal vein with a complete absence of flow, which was undetectable with grayscale sonography alone.
of the portal vein with a complete absence of flow, which was undetectable with grayscale sonography alone.




















 Liver parenchyma supplied by thrombosed veins may enhance avidly in arterial phase due to increased hepatic artery flow
Liver parenchyma supplied by thrombosed veins may enhance avidly in arterial phase due to increased hepatic artery flow Tumor thrombus on enhanced MR
Tumor thrombus on enhanced MR






