, Gustav Andreisek2, Erika J. Ulbrich2 and René Roth
(1)
Phoenix Diagnostic Clinic, Cluj-Napoca, Romania
(2)
Institute of Diagnostic and Interventional Radiology, University Hospital Zürich, Zürich, Switzerland
2.1 Anatomy and Normal MRI Appearance
2.1.1 Posterior Cruciate Ligament (PCL)
The posterior cruciate ligament (PCL) is the strongest ligament of the knee. It is intra-articular and extrasynovial. The PCL arises from the anterolateral surface of the medial femoral condyle and reaches the posterior intercondylar area of the tibia. The femoral origin is more anterior than that of anterior cruciate ligament (ACL), and in contrast to the ACL, the PCL is larger at its femoral origin than at its tibial insertion [1]. The tibial attachment is extra-articular, and it is approximately 1 cm distal to the plane of the articular surface [2]. The PCL is the primary restraint to posterior tibial translation relative to the femur and becomes more important in preventing distraction of the joint as the knee reaches higher degrees of flexion [3, 4].
The PCL consists of two functional bundles: the anterolateral and the posteromedial bundle [5]. The anterolateral bundle (65 %) is usually thicker and stronger than the posteromedial bundle (35 %) [6]. Most PCL fibers are not isometric and the bundles have different functions that enable the PCL to resist posterior translation [5]. The length of the ligament is similar to that of the ACL (mean length, 38 mm) [7].
The PCL is seen as a band of low signal intensity in all MR sequences and is usually visualized in its entire length on one or two consecutive sagittal images (Fig. 2.1). The two-bundle anatomy is often well visualized on axial planes, and all axial planes should thoroughly be evaluated for partial (uni-bundle) rupture. To assess the intact attachments of the PCL, axial, sagittal, and coronal images should be evaluated (Fig. 2.1). The axial images are especially helpful for the femoral attachment, whereas the sagittal images are especially helpful for assessing the tibial attachment.

Fig. 2.1
Normal posterior cruciate ligament (PCL) in a 17 year old male. Sagittal proton-density (PD) FSE image (a) shows the PCL as a band of low signal intensity (arrow). Coronal (b) and axial images (c) should always be assessed especially for the femoral (arrow in b) and tibial attachments (arrow in c)
Since the PCL appears as an angulated structure on sagittal MR images, several indirect signs have been described to detect other ligament abnormalities, one of which is the PCL angle. The mean PCL angle is 123° and is smaller in patients with acute anterior cruciate ligament (ACL) tear but also in younger patients without ACL abnormalities [8]. Due to this overlap, indirect signs for ACL tears, i.e., quantitative and semiquantitative signs, should be used with care, especially in the skeletally immature patient [8].
2.1.2 Meniscofemoral Ligaments
The posterior meniscofemoral ligament (Wrisberg ligament) attaches proximally separately from the posteromedial bundle of the PCL [9]. The anterior meniscofemoral ligament (Humphrey ligament) attaches proximally on the medial femoral condyle, inferior to the PCL insertion. Both ligaments attach distally to the posterior horn of the lateral meniscus and contribute to posterior drawer stability [10]. At least one meniscofemoral ligament is present in 70–93 % of knees [4, 7, 11].
The meniscofemoral ligaments are best seen on sagittal and coronal images as low-signal-intensity bands anterior and posterior to the PCL (Figs. 2.2 and 2.3).
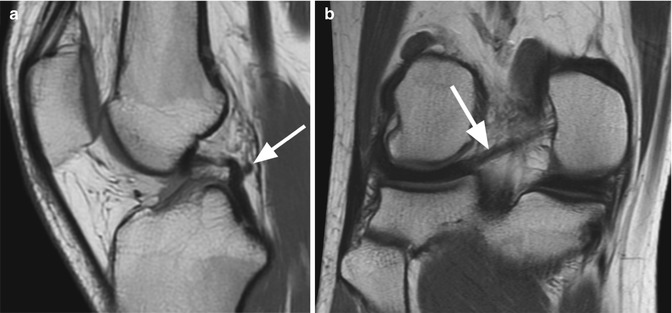
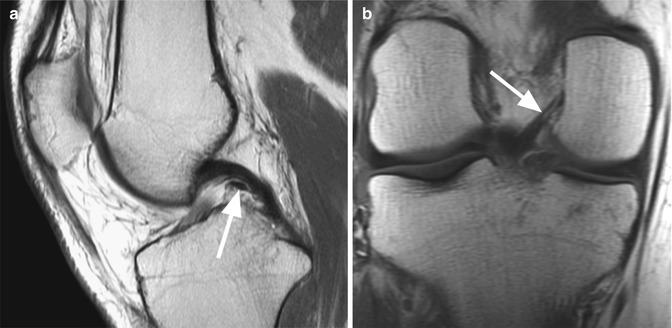
Fig. 2.2
Posterior meniscofemoral ligament (Wrisberg ligament) in a 19 year old female. Sagittal proton-density (PD) FSE image (a) and coronal proton-density (PD) FSE image (b) show the posterior meniscofemoral ligament (arrow) posterior to the posterior cruciate ligament (a) with the distal insertion on the posterior horn of the lateral meniscus and the proximal insertion on the medial femoral condyle (b)
Fig. 2.3
Anterior meniscofemoral ligament (Humphrey ligament) in a 40 year old male. Sagittal proton-density (PD) FSE image (a) and coronal proton-density (PD) FSE image (b) show the anterior meniscofemoral ligament (arrow) anterior to the posterior cruciate ligament (a) with the proximal insertion on the medial femoral condyle (b)
The orientation and characteristic localization of meniscofemoral ligaments should be taken into account in order to differentiate intra-articular lesions such as cartilage displaced and meniscal fragments or pseudotears of the lateral meniscus.
2.1.3 Retrocruciate Fat Pad
Retrocruciate fat pad is situated between the PCL and the posterior joint capsule (Fig. 2.4) [12]. The fat pad may be involved in several pathological intra-articular changes (e.g., fluid collections, inflammation).
Fig. 2.4
Normal retrocruciate fat pad in a 27 year old male. Sagittal proton-density (PD) FSE image shows the retrocruciate fat pad (arrow) situated between the posterior cruciate ligament (small arrow) and the posterior joint capsule (curved arrow). The signal is similar to the subcutaneous fat in all sequences
2.2 MRI Pathological Findings
2.2.1 Acute Tear
Complete Tear
Focal discontinuity and an amorphous high signal intensity due to hemorrhage and edema without visualization of the ligamentous fibers are signs of PCL tear (Figs. 2.5 and 2.6). Isolated PCL tears are found in 24 % of patients [13], and they can be localized at the femoral insertion, in the midsubstance, or at the tibial insertion. The associated findings of other coexisting knee injuries may be present in 76 % of cases and include involvement of medial collateral ligament more often than the lateral collateral ligament and medial meniscus more commonly than the lateral meniscus [13].
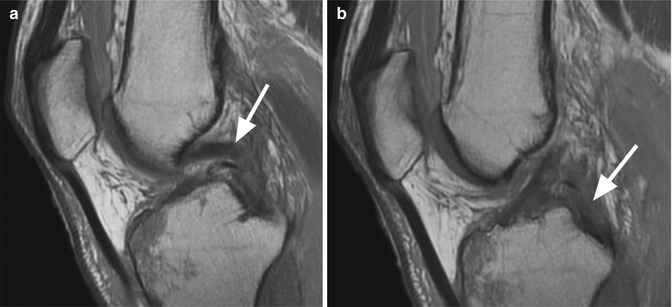
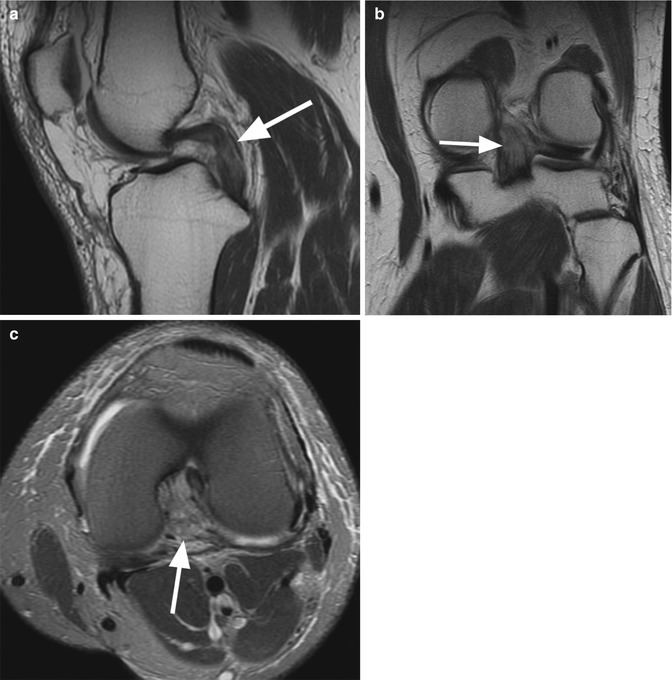
Fig. 2.5
Complete acute tear of the posterior cruciate ligament in a 50 year old male. Two consecutive sagittal proton-density (PD) FSE images (a, b) show complete discontinuity of the fibers (arrow) (a) with hemorrhage and edema in the midsubstance and at the femoral insertion of the ligament (b)
Fig. 2.6
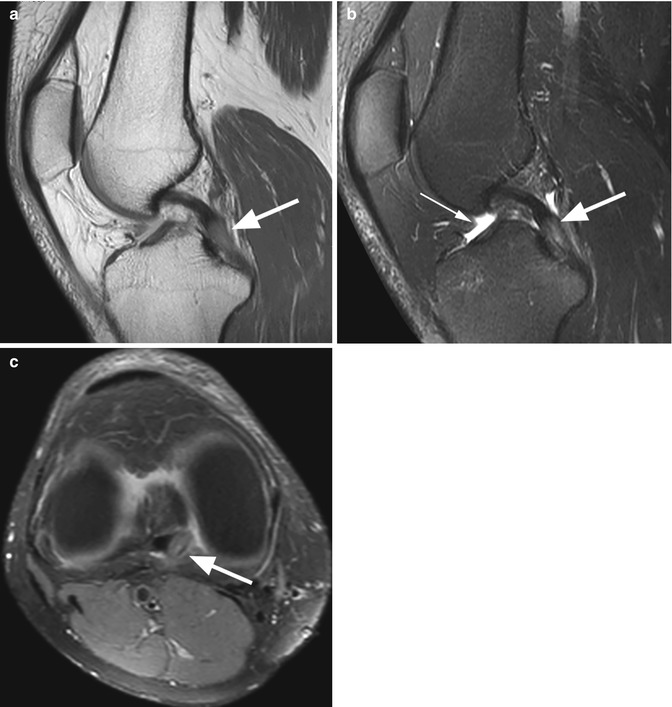
Complete acute tear of the posterior cruciate ligament in a 44 year old female. Sagittal proton-density (PD) FSE images (a) and coronal proton-density (PD) FSE image (b) show diffuse-signal-intensity changes within the ligament (arrow). Although there is the impression of fiber continuity on both sagittal and coronal images (a, b) on axial proton-density (PD) FSE fat-suppressed image (c), there is a complete absence of the fibers with hemorrhage within the distal portion (arrow)
Partial Tear
Partial tears represent 55 % of all PCL tears [13]. Criteria of diagnosis include the presence of increased signal intensity with discernible fibers along the course of the ligament. The partial tear can be interstitial or can involve one of the above described PCL bundles. In partial interstitial tears, there is an increased longitudinal ligamentous signal intensity without disruption of the fibers (Fig. 2.7). In these cases, the PCL bundles can be separated by the signal-intensity changes. The findings of interstitial tear of the PCL must be correlated with an appropriate history of trauma in order to differentiate from a mucoid degeneration of PCL, i.e., in middle-aged patients.
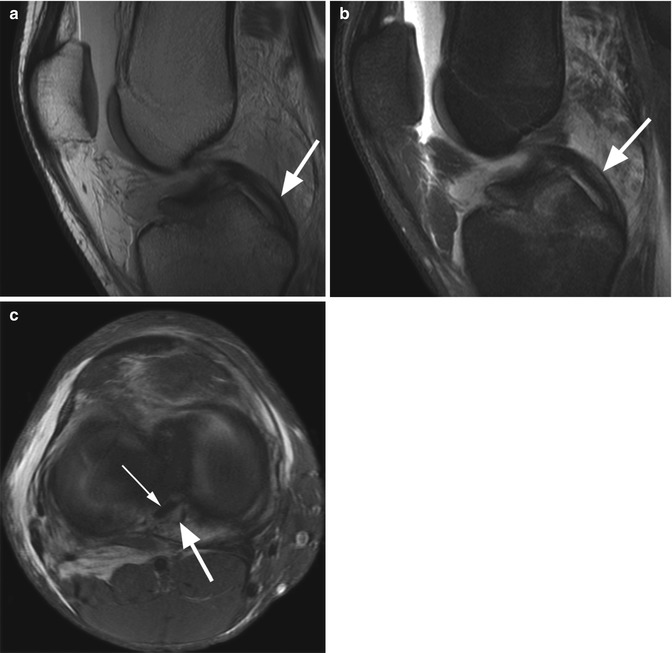
Fig. 2.7
Partial interstitial acute tear of the posterior cruciate ligament involving the posteromedial bundle in an 18 year old male with recent knee trauma. Sagittal proton-density (PD) FSE image (a), sagittal T2-weighted FSE fat-suppressed image (b), and axial proton-density (PD) FSE fat-suppressed image (c) show increased longitudinal signal-intensity changes within the ligament (arrow) without complete discontinuity of the fibers (small arrow in c)
2.2.2 Posterior Cruciate Ligament Avulsion Fracture
The PCL avulsion fracture involves the detachment of the tibial plateau that results from the pulling of PCL from its attachment point. The mechanisms include a severe hyperextension or a direct blow to the anterior tibia with the knee flexed [14]. An early diagnosis is usually possible on standard radiographs where a bony fragment may be visible. At MR imaging, bone marrow edema and a small bone fragment attached to PCL is seen in acute trauma (Fig. 2.8). In chronic cases, the bone marrow edema is usually absent (Fig. 2.9).
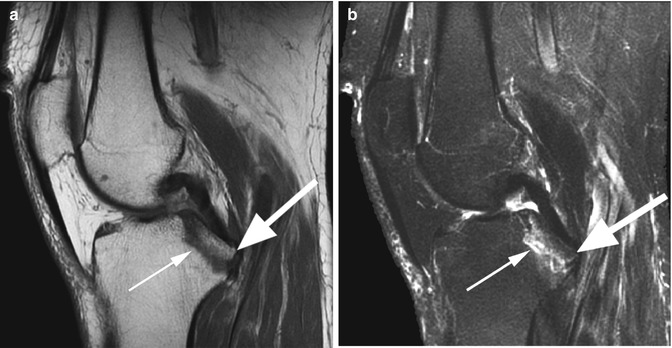

Fig. 2.8
Acute posterior cruciate ligament (PCL) avulsion fracture from pulling from its tibial attachment in a 35 year old female with acute knee trauma. Sagittal proton-density (PD) FSE image (a) and sagittal T2-weighted FSE fat-suppressed image (b) show a bone fragment attached (arrow) to a normal PCL. Bone marrow edema is present at the site of the tibial avulsion (small arrow)
Fig. 2.9
Chronic posterior cruciate ligament (PCL) avulsion fracture in a 68 year old female. Sagittal T2-weighted FSE fat-suppressed image (a) and coronal T1-weighted image (b) show a small bone fragment detached from the tibial attachment (arrow) without adjacent bone marrow edema
2.2.3 Chronic Tear and Mucoid Degeneration
Diffuse thickening (more than 7 mm on sagittal plane) with low or intermediate signal, often seen as focal changes of the PCL, is suggestive for chronic PCL tear [15]. MR imaging shows focal or diffuse changes of low signal intensity on T1-weighted images and intermediate-high signal intensity on T2-weighted images (Fig. 2.10).
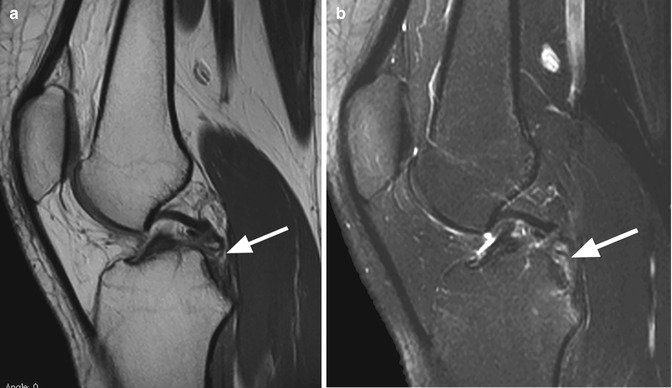
Fig. 2.10
Chronic tear of the posterior cruciate ligament (PCL) in a 17 year old female. Sagittal proton-density (PD) FSE image (a) and sagittal T2-weighted fat-suppressed image (b) show discontinuity of the ligament with focal fibrotic changes without hemorrhage and edema (arrow)
Mucoid degeneration is a rare cause of pain in the middle-aged patients without knee instability [16]. The signal intensity on T2-weighted images is different from that of a joint effusion and enables the differentiation from a ganglion cyst (Fig. 2.11) [16].