Several masses and pseudomasses may present in the orbit, and cross-sectional imaging plays a crucial role in interrogation of these lesions. A strong understanding of orbital anatomy and the pathologies that may affect the structures within allows the radiologist to narrow the differential diagnosis. This article aims to discuss these pathologies with attention to the site of origin, to provide a practical approach to imaging of orbital tumors. While many lesions have characteristic appearances, many features overlap and require correlation with tissue sampling. Nevertheless, imaging is an essential first step to diagnosis, surgical planning, surveillance, and follow-up of orbital masses.
Key points
-
•
Numerous masses and pseudomasses affect the orbit, and knowledge of different structures and spaces helps to narrow the differential.
-
•
Demographics such as age and sex are essential to consider when attempting to diagnose an orbital mass, as are associated symptoms.
-
•
Diffusion weighted imaging often provides clues to malignancy and may help differentiate some orbital masses from one another—however, in some cases tissue sampling may be necessary.
Abbreviations
| ACC | adenoid cystic carcinoma |
| AML | acute myeloid leukemia |
| AVM | arteriovenous malformation |
| CMV | cavernous venous malformation |
| CT | computed tomography |
| DWI | diffusion weighted imaging |
| IOI | idiopathic orbital inflammation |
| NF1 | neurofibromatosis type I |
| NF2 | neurofibromatosis type 2 |
| ONSM | optic nerve sheath meningioma |
| OPG | optic pathway glioma |
| RMS | rhabdomyosarcoma |
Introduction
The orbits house a multitude of different structures, from which various benign and malignant mass and pseudomass lesions may arise. Orbital masses may present with proptosis or with symptoms related to mass effect on the orbital structures. Imaging evaluation plays a key role in the assessment of orbital masses—not only to narrow the differential diagnosis, but to delineate the extent of lesions and assess their involvement of important nearby structures. While computed tomography (CT) provides the best assessment for bone erosion and calcifications, MR imaging provides the best soft tissue contrast, and the 2 are often complimentary. In this article, we will discuss the most common orbital masses based on site of origin, including those arising from the globe, optic nerve sheath complex, extraocular muscles, lacrimal gland, and those that do not seem to arise from any particular structure in the orbit. While infectious processes can mimic orbital masses, and both benign and malignant lesions arising from nearby structures can extend into the orbit, these lesions are beyond the scope of this article. Lesions of the bone that may involve the orbit are also out of the scope of this article.
The recurring characters
Before delving into location-specific lesions, it is worth addressing a few entities, which may appear in multiple different anatomic sites—lymphoma, metastasis, and idiopathic orbital inflammation.
Ocular Adnexal Lymphoma
Despite being overall rare, the most common orbital malignancy in adults is ocular adnexal lymphoma ( Fig. 1 ), , the vast majority of which are of the B-cell mucosa associated lymphoid tissue type. This entity is very rare in the pediatric population. The periorbital tissues including the conjunctiva are a common location (∼25%–40% of cases depending on the case series); however, this entity may be seen anywhere in the orbit. , Classically, lymphoma masses in the orbit mold around the surrounding structures. , When present in the lacrimal gland or the extraocular muscles, these structures may simply appear diffusely enlarged. Due to the high cellularity of lymphoma, lesions classically show reduced diffusivity on diffusion weighted imaging (DWI). This technique has been in particular used to help differentiate lymphoma from chronic inflammatory diseases such as idiopathic orbital inflammation, which does not show reduced diffusivity. ,,,,, Lack of associated pain, presentation in older patients in the 6th or 7th decades, and the presence of lymphadenopathy in patients with systemic lymphoma can be helpful diagnostic clues. Systemic lymphoma is present or may eventually develop in approximately one-third of patients. Prognosis is generally good, particularly in localized disease where radiation therapy may be employed. , As with other lymphomas, systemic staging is essential for treatment planning and selection of therapy.
Ocular adnexal lymphoma in an 88-year-old man. ( A ) Axial DWI shows a large left orbital mass with reduced diffusivity. ( B ) Corresponding axial ADC map confirms low diffusivity (mean ADC value 0.6 × 10–3 mm2/s). ( C ) Coronal T2WI shows molding of the mass around structures without significant distortion. ( D ) Axial postcontrast T1WI shows proptosis and homogeneous contrast enhancement.
Metastasis
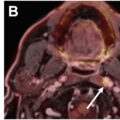
Various malignancies can metastasize to the orbit, most commonly to the bone, soft tissues, and extraocular muscles ( Fig. 2 ). The most common primary tumor of origin is breast cancer, accounting for ∼30 to 60% depending on the case series. Breast metastasis demonstrates a tissue-specific predilection for the extraocular muscles and adjacent fat, as well as the choroid, and may present with rapid onset diplopia or vision loss. Lung, prostate, and cutaneous melanoma are usually the next most common in most case series. ,, Carcinoid tumors, while overall rare, have a proclivity to metastasize to the orbit. Occasionally, a malignancy may first declare itself with an intraorbital metastasis. In rare instances of scirrhous breast cancer, patients may present with paradoxic enophthalmos due to desmoplastic reaction and scarring-related traction within the orbit. , Treatment varies depending on the status of the patient’s systemic disease and symptoms, though overall orbital metastasis suggests a poor prognosis.
Six cases of orbital metastasis. ( A ) Axial postcontrast T1WI shows left lateral rectus muscle metastasis from breast cancer. ( B ) Axial T2WI shows right retroorbital metastasis and enophthalmos from scirrhous breast cancer. ( C ) Axial postcontrast T1WI shows right ocular metastasis from breast cancer. ( D ) Axial CT shows left medial rectus muscle metastasis from cutaneous melanoma. ( E ) Coronal T1WI shows bone metastasis from prostate cancer extending into the orbit. ( F ) Coronal T1WI in a 1-year-old child shows bone metastasis from neuroblastoma extending into the orbit.
In the pediatric population, the most common orbital metastasis is from neuroblastoma, occurring in about one-third of cases and eliciting the characteristic periorbital ecchymosis or racoon eyes . , Leukemia may involve the orbit in children, most commonly with acute myeloid leukemia (AML) presenting as subperiosteal masses seeping into the extraconal space. , Extramedullary masses in AML are termed myeloid sarcoma, historically termed chloroma due to their greenish coloration.
Idiopathic Orbital Inflammation
A benign pseudomass , which may involve multiple structures is idiopathic orbital inflammation (IOI) historically known as orbital pseudotumor ( Fig. 3 ). As the name suggests, this is an inflammatory condition of the orbit, often of unknown etiology and is a diagnosis of exclusion but may be seen associated with immunoglobulin 4 (IgG4)-related disease, other autoimmune or lymphoproliferative diseases. This entity may be unilateral or bilateral and demonstrates a wide variety of clinical presentations in multiple organs. A key clinical feature in the orbit is pain, which may help distinguish this entity from other orbital lesions that may be painless. , While IOI most commonly involves the lacrimal glands, it should also be considered with extraocular muscle enlargement that does not fit well with thyroid eye disease, especially if there is pain, other associated inflammatory findings in the orbit, and involvement of the myotendinous junction. The mainstay treatment is systemic steroids, though refractory cases may be treated with radiation, immunosuppression or biologic agents.
Idiopathic orbital inflammation in three different patients. ( A ) Axial postcontrast T1WI shows involvement of the lacrimal glands. ( B ) Coronal postcontrast T1WI shows involvement of the superior rectus muscle. ( C , D ) Axial postcontrast T1WI and axial ADC map show diffuse involvement of multiple orbital structures without diffusion restriction (mean ADC value 1.7 × 10–3 mm2/s).
Other chronic inflammatory diseases including IgG4-related disease, sarcoidosis, and granulomatosis with polyangiitis can similarly present as a pseudomass and involve multiple structures in the orbit; these are beyond the scope of this article.
Ocular masses
Retinoblastoma
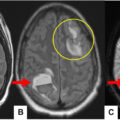
The most common primary intraocular mass in children is retinoblastoma ( Fig. 4 ), with 95% of cases seen before age 5. There are both sporadic cases as well as cases associated with the tumor suppressor RB1 gene mutation, resulting in a cancer predisposition syndrome. Notably, the 2-hit hypothesis for hereditary oncogenesis was first conceived in 1971 by Knudson specifically with respect to retinoblastoma. About 40% of cases are bilateral, the vast majority of which are associated with a germline mutation. Intracranial tumors may also be seen in the pineal or suprasellar regions, resulting in trilateral or quadrilateral retinoblastoma. , Lesions may metastasize to the bones, lymph nodes, or liver. There is also increased risk for sarcomas and other malignancies in patients with retinoblastoma1 gene (RB1) mutation; radiation is therefore avoided due to risk of developing sarcomas, a phenomenon sadly recognized long after patients were treated with radiation in the 1950s.
Retinoblastoma in a 1-year 6-month-old child. ( A ) Coronal T2WI shows an intraocular nodule along the inferior left globe. ( B ) Axial postcontrast T1WI shows contrast enhancement. ( C , D ) Axial DWI and ADC map show reduced diffusivity.
Retinoblastoma classically presents with leukocoria, noticed due to loss of the red reflex on clinical ophthalmologic examination or during flash photography. , In the setting of limited access to medical care, more advanced cases may present with proptosis, vision loss, or glaucoma.
On imaging, tumoral calcifications are a key diagnostic feature, seen in approximately 95% of cases. Although CT effectively demonstrates these calcifications, ultrasound has become the preferred modality due to concerns about an increased risk of secondary cancers from CT-related radiation. MR imaging most commonly demonstrates an irregular enhancing mass with reduced diffusivity. There is risk of subretinal spread associated with retinal detachment, intravitreous spread, and extraocular extension. Imaging should report tumor size and location, presence of retinal detachment, vitreous signal abnormality including hemorrhage, anterior segment invasion (lens, ciliary body, iris, and anterior chamber), extension along the optic nerve, extraocular orbital involvement, and intracranial spread. These findings may impact staging or alter treatment decisions.
While vision-sparing treatment may be used for lower stage lesions, many require enucleation. The prognosis heavily depends on the stage, but is typically excellent in developed nations, with survival greater than 90%. Unfortunately, this is not the case worldwide, with a delay in diagnosis greater than 6 months associated with a 70% mortality in developing countries.
Uveal Melanoma
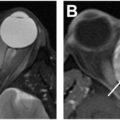
The most common primary ocular mass lesion in adults is uveal melanoma ( Fig. 5 ), arising from 1 of the 3 uveal structures—the choroid (∼90%), ciliary body (∼7%)-, or iris (∼3%). , Lesions of the iris generally have a better prognosis as they are easily seen and therefore identified earlier while they are smaller. The large majority (>95%) occur in patients of northern European descent. These lesions demonstrate varying degrees of pigmentation with about 20% amelanotic, but typically appear as a dark pigmented mass on clinical ophthalmologic examination. If there is a high amount of melanin, these lesions may demonstrate high intrinsic T1 signal on precontrast images, helping to distinguish it from other masses, though this may make assessment for contrast enhancement difficult. Three growth patterns have been described—lentiform, dome-shaped, and mushroom-shaped, with the latter suggesting a subretinal spreading pattern; they commonly metastasize to the liver (90%). Treatment varies, with large lesions requiring enucleation, and smaller lesions potentially amenable to vision-sparing brachytherapy, external beam radiotherapy or transpupillary thermotherapy.
Uveal melanoma involving the medial left globe. ( A ) Coronal T1WI shows intrinsically high signal. ( B ) Coronal T2WI shows low signal; together with high T1 signal, this suggests high melanin content. ( C ) Coronal postcontrast T1WI shows enhancement, though difficult to distinguish from the baseline high T1 signal.
Ocular Metastasis
Due to its high vascularity, the choroid is the most common site of ocular metastases. On MR imaging, they can mimic amelanotic melanomas, and history of a known primary or multifocal disease may be the main clue to the diagnosis.
Optic nerve sheath complex masses
Optic Pathway Glioma
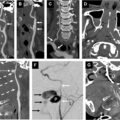
The most common mass involving the optic nerve sheath complex is an optic pathway glioma (OPG), which originates from the optic nerve ( Fig. 6 ). These lesions are typically indolent low-grade pilocytic astrocytomas and most often seen in children. They may occur sporadically or in association with neurofibromatosis type I (NF1), affecting approximately 15% to 30% of children with NF-1 , In NF1, they appear as thickened caliber of the optic nerve itself with tortuosity, possibly with accompanying high T2 signal. There may be low-level enhancement following contrast administration. Non-NF1 associated gliomas are more likely to appear fusiform. Most commonly, they are unilateral but may be bilateral, and have a proclivity for the intraorbital segments of the nerve as well as the optic chiasm. OPGs can also affect any part of the optic apparatus more posteriorly, as well as diencephalic structures, with more posterior involvement generally associated with worse symptoms and prognosis. On imaging, involvement of the contralateral optic nerve as well as any intracanalicular or intracranial extension should be reported.
Optic pathway glioma in a 3-year 10-month-old child with NF1. ( A ) Axial T2WI shows enlargement and tortuosity of the right intraorbital optic nerve. ( B ) Coronal T2WI shows subtle high signal compared to normal white matter. ( C ) Coronal postcontrast T1WI shows a crescent-like area of enhancement along the medial optic nerve sheath, consistent with perineural arachnoidal gliomatosis.
In some cases, crescentic or circumferential thick enhancement and T2 hyperintense signal may be seen within the nerve sheath surrounding the expanded optic nerve, a phenomenon termed perineural arachnoidal gliomatosis. This reflects perineural extension of the optic glioma into the surrounding subarachnoid space and is often associated with NF-1 but can also be seen in isolated cases.
Lesion size does not correlate well with symptoms, and management is more appropriately dictated by clinical visual acuity assessment. Treatment is typically conservative with surveillance or medical therapy with bevacizumab or targeted medical therapies such as mTOR inhibitors. In adults, optic nerve gliomas are very uncommon and likely to be high-grade lesions with very poor prognosis.
Optic Nerve Sheath Meningioma
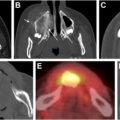
The second most common mass of the optic nerve sheath complex is an optic nerve sheath meningioma (ONSM), which arises from the optic nerve sheath itself ( Fig. 7 ). Like other meningiomas, these lesions may be hormone-responsive and therefore are about 2 to 3 times more common in women, with potential to grow in response to hormone stimulation such as pregnancy. Neurofibromatosis type 2 (NF2) is a risk factor, with about 30% prevalence in children with NF2. Meningiomas involving the orbit may be primary, arising directly from the nerve sheath meninges, or secondary, arising from a larger intracranial mass such as a tuberculum sella meningioma.
Optic nerve sheath meningioma. ( A ) Coronal postcontrast T1WI shows a donut -like rind of circumferential enhancement around a small-caliber right optic nerve. ( B ) Axial postcontrast T1WI shows tram-tracking along the posterior aspect of the intraorbital optic nerve sheath.
On imaging, ONSM classically shows longitudinal and circumferential extension around the periphery of the nerve, giving a tram-track appearance on axial postcontrast imaging and a donut appearance on coronal postcontrast imaging. This appearance may be seen with other orbital diseases such as lymphoma, IOI, sarcoid, metastasis, or perineuritis and is thus not entirely specific. Other possible growth patterns include a tubular or fusiform mass along the nerve sheath, or more rarely as an eccentric nodule. Unlike perineural gliomatosis with optic gliomas, ONSM should not show enlargement of the optic nerve itself. Ga-68-DOTATATE PET-CT can be used to help distinguish ONSM from these other lesions, as meningiomas demonstrate avid uptake due to their strong expression of somatostatin receptors.
The typical presentation is gradual painless vision loss. , On clinical examination, the most common finding is optic disc edema, and in some cases may show optociliary shunt vessels, which form at the disc due to compression of the central retinal vein. , While the lesion is nonlethal, its natural history is typically that of complete or near-complete vision loss if left untreated. Surgical outcomes for these lesions are very poor, almost universally ending with vision loss or worsening due to compromise of the nerve sheath vasculature. Rare cases of exophytic lesions may be more surgically amenable but still carry a high risk of complication. Stereotactic radiation has emerged as an excellent treatment modality, with modern techniques providing excellent lesion control (approaching 100%) and long term visual outcomes (90%).
Extraocular muscle lesions
Recurring Characters
Ocular adnexal lymphoma may present as infiltration of one or more extraocular muscles resulting in enlargement, though is more commonly seen in the lacrimal glands, conjunctive, or extraconal fat. Older age of onset and the presence of systemic lymphoma are again useful distinguishing clues. DWI can help to distinguish cellular lymphomas that show a greater degree of reduced diffusivity compared to chronic inflammatory diseases including thyroid orbitopathy and IOI.
Although uncommon, metastases can involve the extraocular muscles. Breast cancer in particular has a proclivity for the extraocular muscles and adjacent fat and may present with rapid onset diplopia. On MR imaging, this may appear as enlargement of the affected muscle or an enhancing intramuscular nodule. Metastatic disease should be suspected when there is a known primary malignancy, multiple lesions, or rapid growth.
IOI may present in a myositic form, the second most common presentation, with involvement of 1 or more extraocular muscles. Pain is an important distinguishing feature, and hyperenhancement and perimuscular edema are often seen on imaging.
Lacrimal gland masses
The lacrimal gland is comprised of a small palpebral lobe along the upper eyelid and a larger orbital lobe situated more superolaterally within the extraconal orbit. These lobes are divided by the aponeurosis for the levator palpebrae superioris muscle. In evaluation of a lacrimal mass, it should be noted whether 1 or both lobes are involved, if there is diffuse involvement/enlargement, and if there is contour change of the adjacent globe or bone. Epithelial tumors usually appear as more discrete masses within a single lobe (most commonly the orbital lobe) and indent the globe contour. Lymphoma is typically more diffuse, involving both lobes, and as softer lesions will mold to the globe contour. , Lymphoproliferative lesions will also more likely demonstrate uniform signal, whereas epithelial tumors often demonstrate MR imaging signal heterogeneity.
Lacrimal gland enlargement may be inflammatory (50%), lymphoid (25%), and salivary type epithelial neoplasms (25%).
Recurring Characters
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


