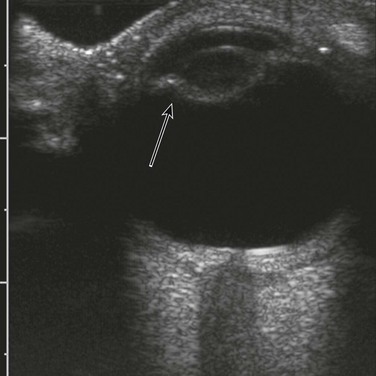
Chapter 5 Ocular evaluation comprises assessment for the presence or absence of eyes, the morphology of the lens and vitreous, and ocular biometry.1 Anophthalmia and Microphthalmia With primary anophthalmia, ocular tissue in the orbit is completely absent because no development of the eyes has occurred. Primary anophthalmia usually is associated with chromosomal abnormalities such as trisomy 13 or genetic syndromes such as CHARGE syndrome, incontinentia pigmenti, Norrie disease, SOX2-related eye disorders, Walker-Warburg syndrome, and oculo-auriculo-vertebral spectrum.2–7 Loss of ocular tissue caused by an insult during development results in secondary anophthalmia. Etiologies include infection (e.g., rubella), a vascular event (e.g., Goldenhar syndrome), or a toxic or metabolic event (e.g., low or high vitamin A levels). The ocular diameter is below the fifth percentile.8 Matthew-Wood syndrome (also known as Spear syndrome, PMD, or PDAC syndrome) is composed of pulmonary hypoplasia/agenesis, diaphragmatic hernia/eventration, anophthalmia/microphthalmia, and cardiac defect.9 In a case of congenital diaphragmatic hernia, associated abnormal orbital morphology and biometry and cardiac anomalies can allow this diagnosis to be made antenatally (Fig. 5-1). Figure 5-1 Matthew-Wood syndrome. Walker-Warburg syndrome, a type of congenital muscular dystrophy, also can be diagnosed antenatally through the association of Dandy-Walker spectrum, along with a Z-shaped brainstem on midline sagittal MRI views, an occipital cephalocele, and ocular asymmetry (Fig. 5-2 and e-Fig. 5-3). Figure 5-2 Walker-Warburg syndrome. e-Figure 5-3 Walker-Warburg syndrome. Aicardi syndrome is a rare genetic malformation syndrome that can be diagnosed antenatally by the association of partial or complete absence of the corpus callosum, ocular abnormalities, and a posterior fossa cyst. Aicardi syndrome is thought to be caused by a defect on the X chromosome because it has only been seen in girls and in boys with Klinefelter syndrome (Fig. 5-4 and e-Fig. 5-5). Figure 5-4 Aicardi syndrome. e-Figure 5-5 Aicardi syndrome. On ultrasound examination, the lens and vitreous are equally hypoechoic; however, the outline of the lens can be seen as a thin hyperechoic ovoid anteriorly within the globe. Typically, however, the only reflection from the lens is from the surfaces perpendicular to the insonating beam, and it can be difficult to see (Fig. 5-6). Figure 5-6 Sonographic appearances. On MRI, the entire lens has a low signal compared with the high signal of the vitreous (Fig. 5-7). By endovaginal ultrasound, the lens is visible by 14 weeks as a thin echogenic rim with an anechoic center. The hyaloid artery can be seen as an echogenic line bisecting the vitreous, which, during conversion of the primary vitreous to mature secondary vitreous, gradually becomes beaded as it involutes, a process that should be completed by 30 weeks menstrual age.10,11 The remnant channel through the vitreous is known as the Cloquet canal. Figure 5-7 Fetal magnetic resonance imaging orbital appearance. Failure of involution of the hyaloid artery results in a spectrum of abnormalities known as persistent hyperplastic primary vitreous, which is seen frequently with trisomy syndromes and other forms of abnormal brain development.12,13 It is usually unilateral. Clinically the presentation is variable and includes leukokoria, vitreous hemorrhage, retinal detachment, microphthalmos, and lens opacification. The diagnosis can be made antenatally or by ultrasound, computed tomography (CT), or MRI postnatally. Ultrasound can detect the hyaloid vessel. A cone-shaped retrolental density is the characteristic finding on CT and MRI. Findings described on CT include a small irregular lens with a shallow anterior chamber; intravitreal densities of variable shape, suggesting the persistence of fetal tissue in the Cloquet canal; and enhancement of abnormal intravitreal tissue after intravenous administration of contrast media. On MRI the appearance is that of low-signal intensity linear plaques extending from the posterior part of the lens to the optic nerve head. Calcification is unusual (Fig. 5-8 and e-Fig. 5-9). Figure 5-8 Persistent hyperplastic primary vitreous. e-Figure 5-9 Persistent hyperplastic primary vitreous. Cataracts are seen in a variety of metabolic, infectious, genetic, and chromosomal abnormalities that affect the fetus, including toxoplasmosis; X-irradiation; in-vitro fertilization; persistent hyperplastic primary vitreous; Nance-Horan, Adams-Oliver, Walker-Warburg, and Neu-Laxova syndromes; rhizomelic chondrodysplasia punctata; trisomy 17 mosaicism; and trisomy 21 (Fig. 5-10).5,14–23 Optic nerve hypoplasia is usually sporadic and difficult to detect prenatally; however, it has a number of associations that potentially can be diagnosed prenatally because of associated structural abnormalities, several of which are discussed in this chapter (Box 5-1 and Fig. 5-11). Box 5-1 Associations with Optic Nerve Hypoplasia
Prenatal, Congenital, and Neonatal Abnormalities
Presence or Absence of the Eyes
Primary Anophthalmia
Secondary Anophthalmia
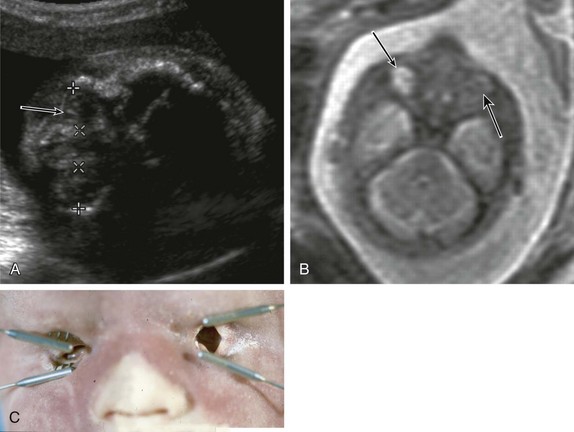
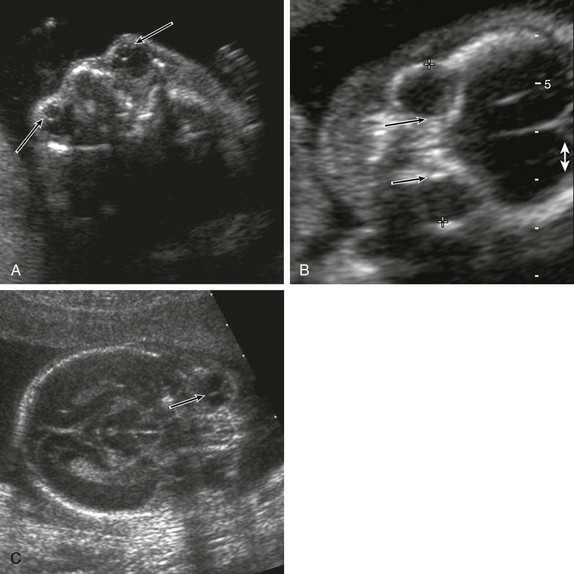
A, Fetal ultrasonography shows that biometry was delayed and the lens and globe have an abnormal appearance, appearing echogenic (arrow). B, Fetal magnetic resonance imaging shows apparent anophthalmia (large arrow) and microphthalmia (small arrow). C, A postmortem examination reveals that the globes are absent. (From Robinson AJ, Blaser S, Toi A, et al. Magnetic resonance imaging of the fetal eyes—morphologic and biometric assessment for abnormal development with ultrasonographic and clinicopathologic correlation. Pediatr Radiol. 2008;38:971-981.)

A fetal magnetic resonance image shows symmetric globes (arrows). (From Robinson AJ, Blaser S, Toi A, et al. Magnetic resonance imaging of the fetal eyes—morphologic and biometric assessment for abnormal development with ultrasonographic and clinicopathologic correlation. Pediatr Radiol. 2008;38:971-981.)
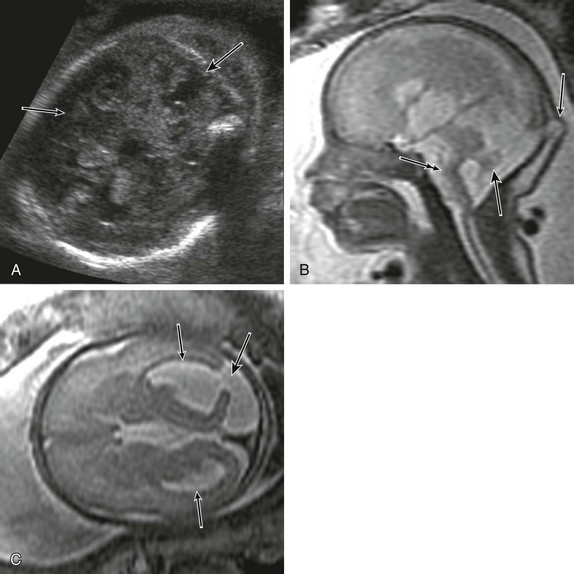
A, Prenatal ultrasound shows a defect in the cerebellar vermis (arrows). B, Fetal magnetic resonance imaging (MRI) shows a Z-shaped brainstem (double arrow), a small vermis (large arrow), and an occipital cephalocele (small arrow). C, Fetal MRI shows asymmetric ventriculomegaly (small arrows) plus a cortical defect (large arrow).

Fetal magnetic resonance imaging demonstrates unilateral microphthalmia (arrow).
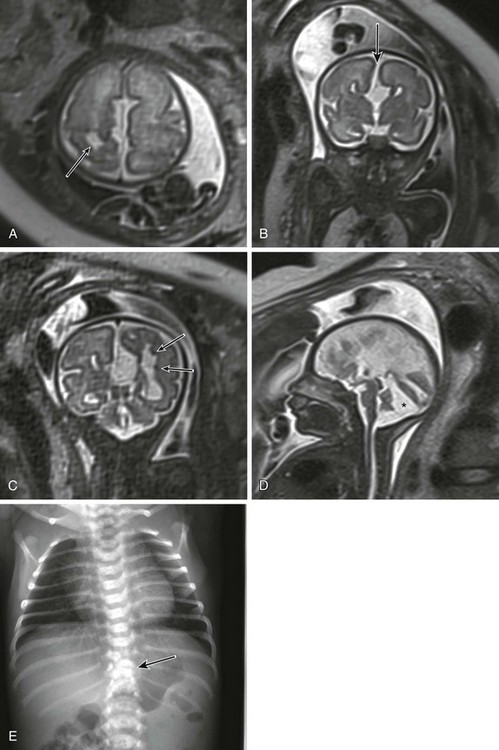
A, Fetal magnetic resonance imaging (MRI) shows a porencephalic cyst (arrow). B, Fetal MRI shows callosal dysgenesis with a “high-riding” third ventricle continuous with an interhemispheric fissure (arrow). C, Fetal MRI shows subependymal heterotopias (arrows). D, Fetal MRI shows a posterior fossa cyst with abnormal cerebellar vermis. E, A neonatal radiograph shows vertebral segmentation anomalies (arrow).
Morphology of the Lens and Vitreous
A, Lens and vitreous. The surfaces of the lenses are seen as faint curvilinear echoes in the anterior globe (arrows). B, A transorbital view of the fetal face shows the measurement of the binocular distance with the calipers on the malar margins of the orbit. The interocular distance is measured between the two ethmoidal margins (arrows). C, An ultrasound image shows the appearance of the hyaloid artery (arrow). (From Robinson AJ, Blaser S, Toi A, et al. Magnetic resonance imaging of the fetal eyes—morphologic and biometric assessment for abnormal development with ultrasonographic and clinicopathologic correlation. Pediatr Radiol. 2008;38:971-981.)

The entire lens has a low signal compared with the high signal of the vitreous. (From Robinson AJ, Blaser S, Toi A, et al. Magnetic resonance imaging of the fetal eyes—morphologic and biometric assessment for abnormal development with ultrasonographic and clinicopathologic correlation. Pediatr Radiol. 2008;38:971-981.)
Persistent Hyperplastic Primary Vitreous
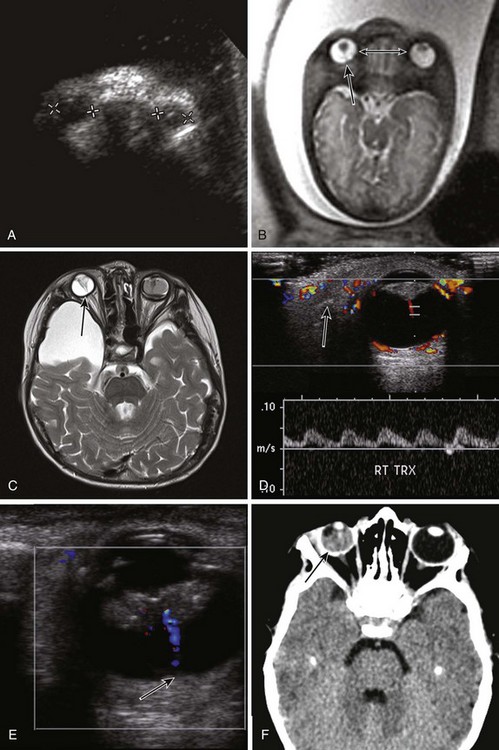
A, Fetal ultrasonography shows the absence of normal anatomy and ocular hyperechogenicity. B, Fetal magnetic resonance imaging (MRI) shows hypertelorism (double-headed arrow) plus a persistent hyaloid artery (large arrow) and a triangular-shaped lens. C, An axial T2-weighted MRI demonstrates a low funnel-like signal extending from the right posterior lens to the optic nerve head (arrow). A similar low signal is noted on the left with associated vitreous hemorrhage. Note the incidental right middle cranial fossa arachnoid cyst. D, Doppler ultrasound reveals an arterial waveform within the hyaloid artery (arrow). E, Ultrasound shows thickening of the soft tissues posterior to the lens and a hyaloid vessel (arrow). F, An axial noncontrast computed tomography image shows increased attenuation in the right posterior chamber in keeping with vitreous hemorrhage (arrow) with linear high density centrally in persistent hyperplastic primary vitreous.
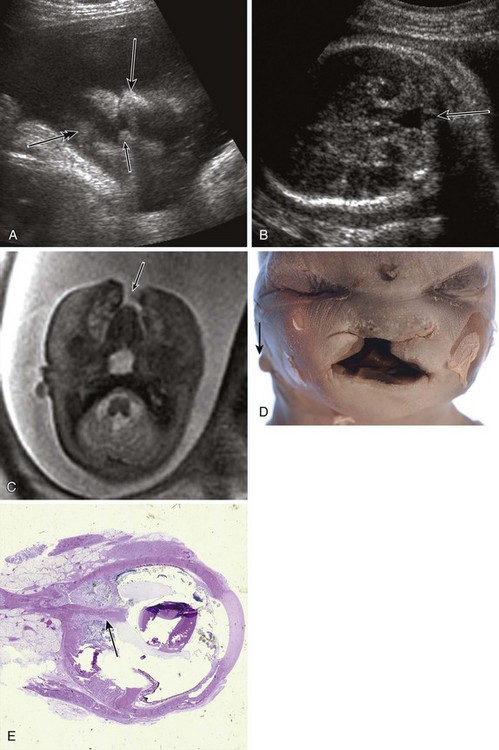
A, Fetal ultrasound shows midline facial clefting including maxillary processes (small arrow), the frontonasal process (large arrow), and the chin (double arrow). B, Fetal ultrasound shows a vermian defect (arrow). C, Fetal magnetic resonance imaging confirms midline facial clefting (arrow). D, A gross pathologic specimen demonstrates hypertelorism and additional microtia (arrow). E, A histopathologic specimen confirms persistence of the hyaloid artery (arrow). (D, From Robinson AJ, Blaser S, Toi A, et al. Magnetic resonance imaging of the fetal eyes—morphologic and biometric assessment for abnormal development with ultrasonographic and clinicopathologic correlation. Pediatr Radiol. 2008;38:971-981.)
Cataracts
Optic Nerve Hypoplasia
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Prenatal, Congenital, and Neonatal Abnormalities