Chapter 29 Central nervous system (CNS) anomalies occur in 1.4 to 1.6 per 1000 live births and 3% to 6% of still births.1 Whereas some anomalies can be detected as early as the first trimester (such as anencephaly), others may not develop until—or only become apparent—later in gestation.2 Ultrasound is the initial imaging modality used for the assessment of fetal CNS anomalies. When ultrasound is carefully performed using established guidelines, it can be very sensitive in evaluating the fetal brain.3 Axial images are important for the assessment of biparietal diameter and head circumference measurements, ventricular size, and cerebellar configuration. Coronal and sagittal images can confirm the presence of the cavum septum pellucidum and corpus callosum. However, because of limitations from skull shadowing, fetal lie, maternal obesity, and oligohydramnios, evaluation of the fetal brain by ultrasound may be incomplete. When a fetal CNS anomaly is being considered, magnetic resonance imaging (MRI) is an adjunct that provides additional information.4–7 Advanced techniques include diffusion-weighted imaging, diffusion tensor imaging, and magnetic resonance (MR) spectroscopy.8 The apparent diffusion coefficient normally decreases after 30 weeks’ gestation,9 but higher apparent diffusion coefficient values have been reported in high-risk fetuses.10 Diffusion-weighted imaging can help detect hemorrhage and acute ischemia (Fig. 29-1). Diffusion tensor imaging measures the magnitude and direction of diffusion (fractional anisotropy). Although intrinsic anisotropy is low in the fetal brain, imaging improvements will help understand the onset and timing of delayed white matter connectivity.11,12 Proton MR spectroscopy has advanced the investigation of fetal brain metabolism. Creatine and N-acetylaspartate peaks appear to have a progressive increase, whereas choline decreases in the third trimester.13 Alterations in these peaks may help identify conditions associated with fetal compromise. Figure 29-1 A fetus at 32 weeks’ gestation with periventricular hemorrhagic infarction. Ongoing enhancement of ultrafast MR sequences and postprocessing methodology has resulted in imaging techniques that can evaluate growth, organization, and remodeling processes that occur during fetal brain development.14,15 Three-dimensional volumetric studies have demonstrated the value of quantitative assessment of brain growth in healthy versus high-risk fetuses. Fetuses with congenital heart disease have been shown to have impaired third-trimester brain growth compared with control subjects, offering a method to evaluate timing and progression of abnormal fetal brain growth.16 Three-dimensional reconstruction of the fetal brain can provide cortical measures such as surface area and gyrification indices. Knowledge of normal fetal morphology and development is important when evaluating anomalies. From 18 to 24 weeks’ gestation, the brain is smooth, with minimal sulcation. The ventricles and extraaxial subarachnoid space, including the cisterna magna, are prominent until the third trimester17 (Fig. 29-2). Figure 29-2 Normal development. Neuronal migration patterns can be documented by MRI.18 Three layers are visualized, including the germinal matrix, cell sparse zone, and cortex. The germinal matrix has a low signal on T2-weighted images along the lateral ventricular walls and involutes from posterior to anterior after 28 weeks’ gestation. The cell sparse zone represents migrating glial cells and eventually becomes the white matter. In the second trimester, the cortical ribbon is intermediate in signal. The fetal cortical mantle follows a predictable course in maturation. Gyration progresses throughout the second and third gestation and can be used to assess gestational age (Box 29-1). By 32 weeks’ gestation, extensive gyration and sulcation is present (Fig. 29-3).17–19 The fetal ventricles are prominent in relation to the brain parenchyma until the third trimester. After 25 weeks’ gestation, the ventricles lose their colpocephalic configuration. Fetal ventriculomegaly is defined as an atrial measurement greater than 10 mm with separation of choroid from the medial wall (i.e., floating choroid). Ventriculomegaly can be due to obstruction, atrophy, maldevelopment, or, rarely, overproduction of cerebrospinal fluid. Ultrasound and MRI should be used to carefully assess for findings that suggest chromosomal anomalies (e.g., trisomy 13, 18, or 21), malformations (e.g., Chiari 2, Dandy-Walker, agenesis of the corpus callosum [ACC], or holoprosencephaly), or destructive lesions (e.g., infarction or infection).19–21 The degree of ventriculomegaly has been shown to be associated with the incidence of live birth and survival beyond the neonatal period. With mild to moderate ventriculomegaly (10 to 15 mm), a close search for other anomalies and chromosome evaluation is important for further assessment. When ventriculomegaly is isolated, abnormal outcome can range from 10% to 25%. If other anomalies are present, outcome is worse, with only 50% to 80% of fetuses having a normal neurodevelopmental outcome.22–24 In a large series evaluating fetal ventriculomegaly, motor outcomes were more severely affected than cognitive or adaptive outcomes, although prenatal atrial diameter was not consistently associated with postnatal developmental outcome.25 The corpus callosum forms between the eighth and twentieth week from genu to splenium. The rostrum forms last, between 18 to 20 weeks’ gestation. Anomalies can be complete (ACC) or partial (hypogenesis). The corpus callosum may be difficult to visualize sonographically, particularly in the early weeks of gestation and/or with hypogenesis.26 Sonographic and MR findings include colpocephaly of the occipital horns with parallel orientation of the lateral ventricles, an absent septum pellucidum, and a high-riding third ventricle (Fig. 29-4). Coronal images are particularly helpful in demonstrating the presence or absence of the cavum septum pellucidum and corpus callosum. With ACC, the frontal horns tend to be narrow with straight medial borders secondary to the bundles of Probst, which represent the callosal fibers that have not crossed the midline. The third ventricle may extend superiorly into an interhemispheric cyst. The cerebral convolutions have a radial arrangement on sagittal imaging. An associated lipoma may be present, which will be echogenic on ultrasound and isointense to gray matter on T2-weighted MRI (e-Fig. 29-5). If ACC is isolated, there is a 15% to 25% risk of a handicap and a 10% risk of aneuploidy. If associated anomalies are detected, such as Dandy-Walker malformation, cortical dysplasia, or encephalocele, the outcome is poorer.27–29 Figure 29-4 Agenesis of the corpus callosum. e-Figure 29-5 Corpus callosum lipoma.
Prenatal Imaging
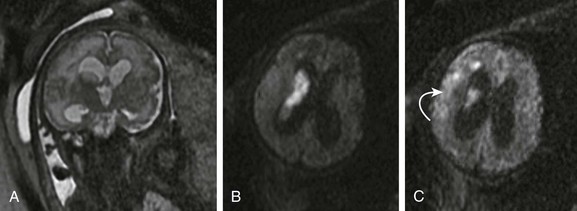
A, A coronal single shot fast spin-echo T2-weighted magnetic resonance image shows moderate ventriculomegaly, intraventricular material, and an abnormal high signal in the right periventricular white matter. An axial diffusion-weighted sequence demonstrates increased diffusion signal within the lateral ventricle (B) and deep frontal white matter (C, arrow) consistent with intraventricular hemorrhage and a periventricular hemorrhagic infarct.
Normal Development of the Fetal Brain
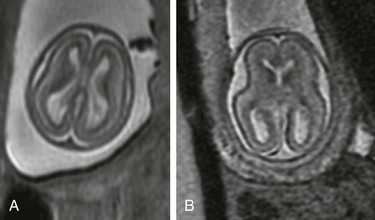
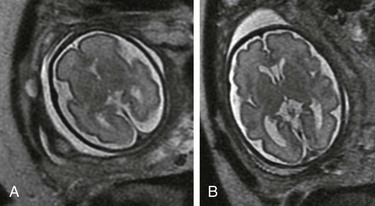
An axial single shot fast spin-echo T2-weighted magnetic resonance image at 19 weeks’ gestation (A) shows a smooth cortex, prominent ventricles, and subarachnoid space. Low-signal germinal matrix is present along the lateral ventricular walls. B, At 22 weeks’ gestation, mild infolding of the sylvian fissure has occurred.
Fetal Ventriculomegaly
Agenesis of the Corpus Callosum
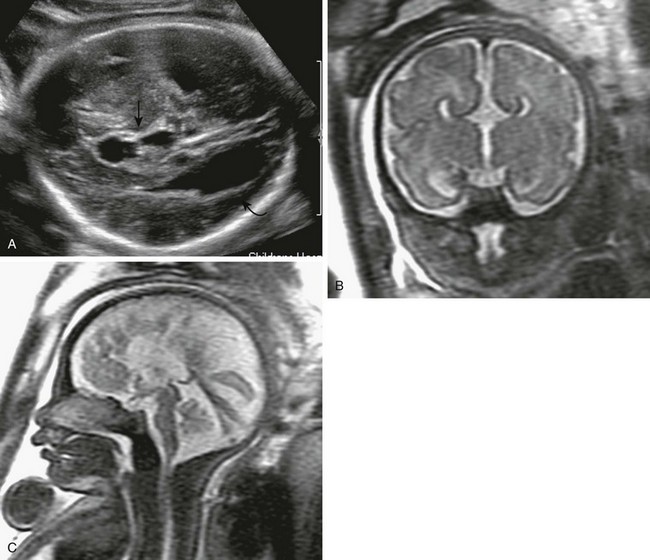
A, A transverse sonogram of the fetal brain shows dilatation of the occipital horns (curved arrow) and a high-riding third ventricle (arrow). B, A coronal T2-weighted image shows that the cavum septum pellucidum is absent, along with a high-riding third ventricle. The medial walls of the anterior horns are indented by the bundles of Probst. C, A sagittal T2-weighted image shows medial sulci radiating perpendicular to the expected course of the corpus callosum. The pericallosal sulcus is absent.
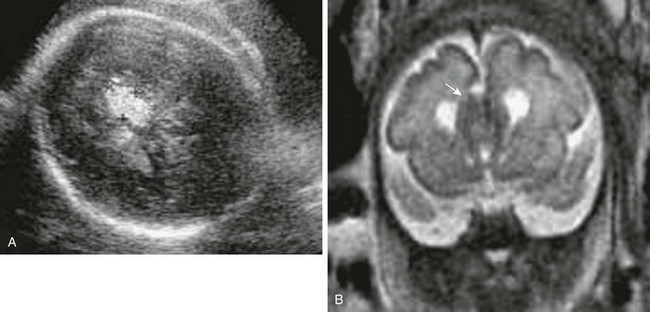
A, An axial sonogram shows a midline echogenic mass representing fat. B, A coronal single shot fast spin-echo T2-weighted magnetic resonance image shows an intermediate signal midline mass (arrow) in the vicinity of the corpus callosum.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


