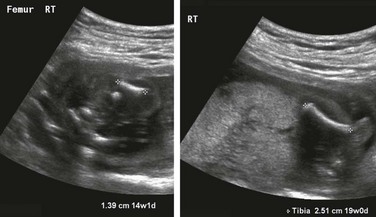
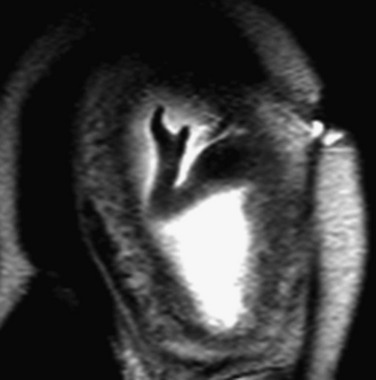
Chapter 131 Etiology: Dysplasias are often the result of genetic mutations that encode for proteins important to development of the growth plate.1,2 Current clinical application of “skeletal dysplasia testing panels” is, however, very limited. Both the range of included mutations and the sensitivities of their detection are expected to increase with time. In utero testing in sporadic cases remains controversial.3 Imaging: Over 450 dysplasias have been described in the literature. Only a small percentage is considered diagnosable in utero with imaging, the first investigation for which is ultrasonography.3,4 Because of the lack of specificity of many of the findings, which have generally to do with abnormal bone shape (formation) or length (growth), efforts at prenatal evaluation have focused on identification of cases in which the neonates are not expected to survive. Identification of these fetuses allows counseling and for the parents and appropriate care planning. To this end, various ultrasonography criteria have been suggested to separate those conditions that are thought to be lethal from those that are not, with very high reliability (Box 131-1).5–11 Most of these criteria correlate limb length with survival. Emphasis is also placed on measures predicting lethal pulmonary hypoplasia. For example, the thoracic circumference is measured in the axial plane at the level of the four-chamber view of the heart; a thoracic circumference at or below the lower limit of the 95% confidence interval for gestational age is considered predictive of lethality in the setting of a micromelic bone dysplasia.12,13 Other findings that may be detected in association with lethality and that increase diagnostic certainty are polyhydramnios and nonimmune hydrops fetalis. It is important to avoid making a diagnosis of lethality in borderline cases and to use the criteria in combination for the most accurate discrimination. The fetus with intrauterine growth retardation should not be assigned a diagnosis of generalized skeletal dysplasia on the basis of proportionate but short bones. Questionable cases in either category deserve follow-up ultrasonography for interval growth. The three most common lethal dysplasias are (1) thanatophoric dysplasia, (2) achondrogenesis, and (3) osteogenesis imperfecta type II. These three diagnoses together constitute the majority of cases. Therefore, a familiarity with their ultrasonographic features is essential (Box 131-2).14,15 Certain skeletal morphologic findings on ultrasonography suggest particular diagnoses in the setting of a suspected dysplasia. Long bone fractures, for example, are indicative of osteogenesis imperfecta or hypophosphatasia, and rib fractures are rarely seen with other diagnoses (Fig. 131-1). Kleeblattschadel, or cloverleaf skull, may be present in several of the acrocephalosyndactyly syndromes (Apert, Carpenter, Crouzon, and Pfeiffer syndromes), campomelic dysplasia, osteocraniostenosis, and thanatophoric dysplasia type II (Fig. 131-2). Hypoplastic scapular bodies are a feature of campomelic dysplasia and Antley-Bixler syndrome.16 However, many findings such as platyspondyly are not specific and must be considered in relation to other features (short ribs, abnormal mineralization, solid organ malformations) to arrive at a more narrow differential diagnosis (Fig. 131-3).17 Three-dimensional ultrasonography can be very helpful when an appropriate volume of fluid is present around the fetus to display the morphology of specific segments, including the face, hands, and feet.18 Figure 131-1 Long bone fractures in a fetus with severe micromelia. Figure 131-2 Kleeblattschadel, or cloverleaf skull (pancraniosynostosis). Figure 131-3 Platyspondyly. Fetal MRI, in general, has not been pursued routinely in the evaluation of fetal dysplasia because of the difficulty in imaging the signal-poor ossified skeleton. However, it may have a role in quantification of fetal lung volumes in cases in which ultrasonography has limitations.19 In addition, fetal MRI has been used successfully to make the diagnosis of dysplasias that primarily involve the epiphyses, taking advantage of the high water content and, therefore, the high T2-weighted signal characteristics of cartilage.20 The use of ionizing radiation is avoided during pregnancy unless the need to make a diagnosis is critical to patient care. In such a circumstance, low-dose computed tomography techniques have been used to reconstruct highly detailed three-dimensional models of the fetal skeleton (Fig. 131-4).21,22 The features described would be compared with an atlas of postmortem radiographs in identified syndromes to aid in diagnosis.23 This strategy can be offered at radiation doses of 3 to 5 millisievert with superb resolution of individual skeletal components.22 Treatment and Follow-up: When a lethal skeletal dysplasia is detected by using ultrasonography, the parents and fetal care team can make informed decisions about the continuation of the pregnancy and the circumstances of delivery. An opportunity exists for neonatal hospice care coordination, when appropriate. Even though ultrasonography is reliable at separating lethal dysplasias from nonlethal dysplasias, neonatal physical examination and radiographs, appropriate genetic testing, and autopsy, if relevant, are crucial in arriving at a specific diagnosis, which, in turn, is necessary for accurate family counseling. Etiology: Limb reductions may be caused by a variety of insults. Some of these are from amputation, such as in the amniotic band sequence spectrum. Although the initiating event in this sequence has not been incontrovertibly established, the most commonly supported theory is that a tear is made in the amnion, exposing the fetus to the more adhesive chorion, with subsequent loss of tissue or the development of a constrictive band.24 In other cases, primary vascular insults are blamed for segmental limb loss, and teratogens (e.g., thalidomide) are highly associated in some instances.25,26 Limb reduction abnormalities can be chromosomal, particularly with Trisomy 18.27 Proximal focal femoral deficiency is a particular form of reduction that affects the femoral head and neck and is associated with fibular aplasia or hypoplasia. It may be unilateral or bilateral (Fig. 131-5). Imaging: Limb reduction anomalies may be subtle in the case of isolated, very distal defects involving fingers or toes. Ultrasonography can characterize the shape of the affected limb well and is diagnostic, and MRI is usually not necessary (Fig. 131-6). Associated findings may include edema of the extremity distal to a constricting band (Fig. 131-7 and Video 131-1). Cine ultrasound sequences can capture the abnormal motion that is a consequence of subluxation or dislocation if the affected segment involves a joint. Random, multiple defects are more likely secondary to amniotic band sequence than are symmetric defects, which tend to be related to chromosomal abnormalities or syndromes (Fig. 131-8).28 As amniotic bands can cause defects in any body part, a thorough evaluation of the entire fetus and its umbilical cord is indicated. Umbilical cord involvement is often overlooked but has consequences because of the risk of cord occlusion.29 Figure 131-7 Amniotic band syndrome.
Prenatal Musculoskeletal Imaging
Skeletal Dysplasias

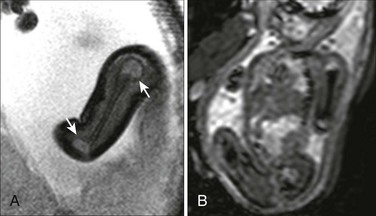
Diagnosis is osteogenesis imperfecta type II.

In the setting of a lethal bone dysplasia, the differential diagnosis includes thanatophoric dysplasia type II, campomelic dysplasia and osteocraniostenosis.
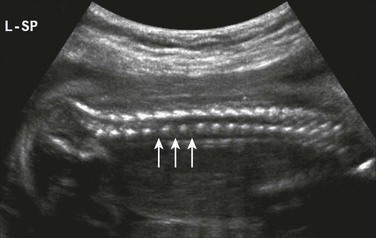
Disc spaces (arrows) are wider than the ossification centers for the vertebral bodies.
Amniotic Band Syndrome and Limb Reductions
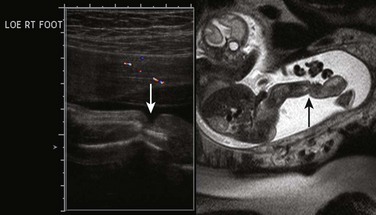
Ultrasound and sagittal T2-weighted single-shot fast spin echo images show focal constriction of both soft tissue and bone (arrows) at the distal leg, with edema of the ankle and foot.