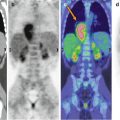
Fig. 28.1
An 8-year-old boy treated for Epstein–Barr-virus-associated hemophagocytic lympho-histiocytosis complicated by aspergillosis. Coronal (a–c) and axial (d–f) CT with lung window (a, d), PET (b, e), and PET/CT fusion (c, f) images show mild FDG accumulation corresponding to the aspergillosis lesion in the lower lobe of the right lung. On the coronal PET/CT fusion image (c), note the splenic and bone marrow activation
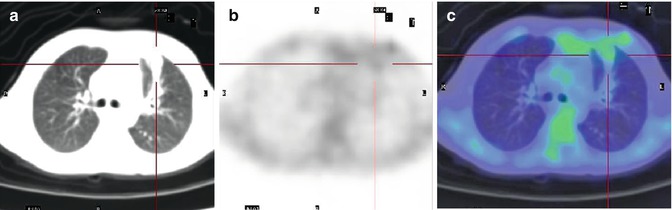
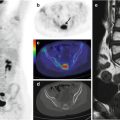
Fig. 28.2
A 5-year-old girl who underwent hematopoietic stem cell transplantation for T-cell immunodeficiency syndrome. Seven days after transplantation, she developed a fever. Axial CT (a), PET (b), and PET/CT fusion (c) images show mild inhomogeneous FDG uptake in the anterior segment of the upper lobe of the left lung. Aspergillus antigenemia was positive and therapy with amphotericin B was initiated
References
1.
Pagano L, Akova M, Dimopoulos G, Herbrecht R, Drgona L, Blijlevens N (2011) Risk assessment and prognostic factors for mould-related diseases in immunocompromised patients. J Antimicrob Chemother 66(1):5–14CrossRef
2.
Ramos ER, Jiang Y, Hachem R, Kassis C, Kontoyiannis DP, Raad I (2011) Outcome analysis of invasive aspergillosis in hematologic malignancy and hematopoietic stem cell transplant patients: the role of novel antimold azoles. Oncologist 16(7):1049–1060PubMedCrossRef
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


