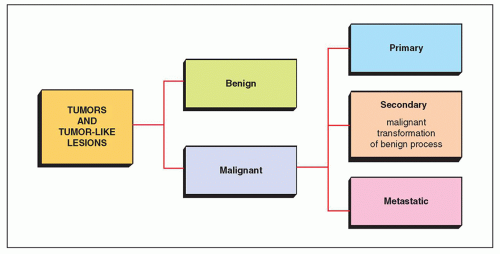
 FIGURE 16.1 Classification of tumors and tumor-like lesions. |
TABLE 16.1 Classification of Tumors and Tumor-like Lesions by Tissue of Origin | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 16.2 Benign Conditions with Potential for Malignant Transformation | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||
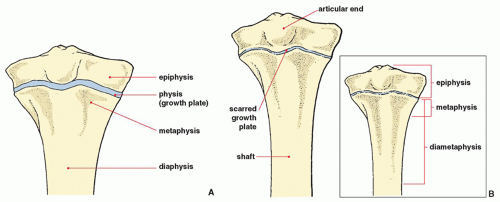 FIGURE 16.2 Parts of the bone. (A) In the maturing skeleton, the epiphysis, growth plate, metaphysis, and diaphysis are clearly recognizable areas. (B) With skeletal maturity, distinct epiphyseal and metaphyseal zones have ceased to exist. The terminology for describing the location of lesions should alter accordingly. The inset illustrates an alternate terminology. |
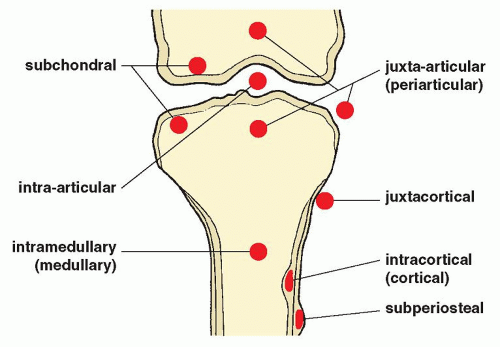 FIGURE 16.3 Terminology used to describe the location of lesions in the bone. |
and neurovascular structures is particularly important for planning limb-salvage surgery.
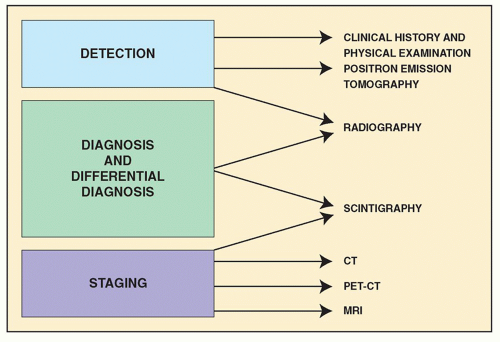 FIGURE 16.4 Imaging of tumors. Imaging of musculoskeletal neoplasms can be considered from three aspects: detection, diagnosis and differential diagnosis, and staging. (Modified from Greenspan A, Jundt G, Remagen W. Differential diagnosis in orthopaedic oncology, 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2007.) |
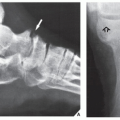
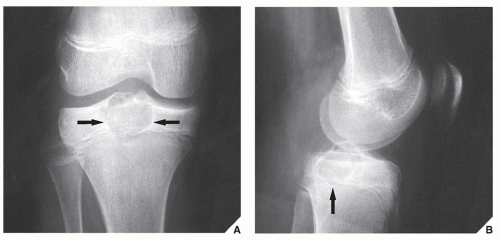 FIGURE 16.5 Specific location of a tumor. Anteroposterior (A) and lateral (B) radiographs of the right knee of a 13-year-old girl reveal a radiolucent lesion located eccentrically in the proximal epiphysis of the tibia, with sharply defined borders and a thin, sclerotic margin (arrows). Here, the lesion’s location and appearance on the standard radiographs led to the correct diagnosis of chondroblastoma. |
tumor vessels, corroborating findings with conventional radiography (Fig. 16.16). Arteriography is often useful in planning for limb-salvage procedures because it demonstrates the regional vascular anatomy and thus permits a plan to be drawn up for the resection procedure. It is also sometimes used to outline the major vessels before resection of a benign tumor (Fig. 16.17), and it can be combined with an interventional procedure, such as embolization of hypervascular tumors, before further treatment (Fig. 16.18). In selected cases, arteriography may help make a differential diagnosis, such as of osteoid osteoma versus a bone abscess.
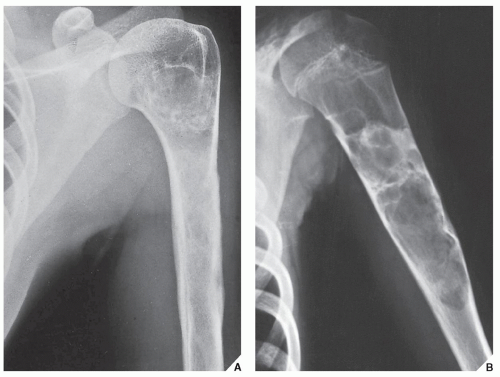 FIGURE 16.6 Comparison radiography: a simple bone cyst. (A) Anteroposterior radiograph of the left humerus in a 26-year-old woman with vague pain for 2 months shows an ill-defined lesion in the medullary region, with a periosteal reaction medially and laterally. There appear to be scattered calcifications in the proximal portion of the lesion. The possibility of a cartilage tumor such as chondrosarcoma was considered, but a radiograph taken 17 years earlier (B) shows an unquestionably benign lesion (a simple bone cyst) that had been treated by curettage and the application of bone chips. In view of this, the later findings were interpreted as representing a healed bone cyst. The patient’s pain was found to be related to muscle strain. |
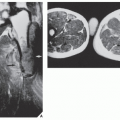
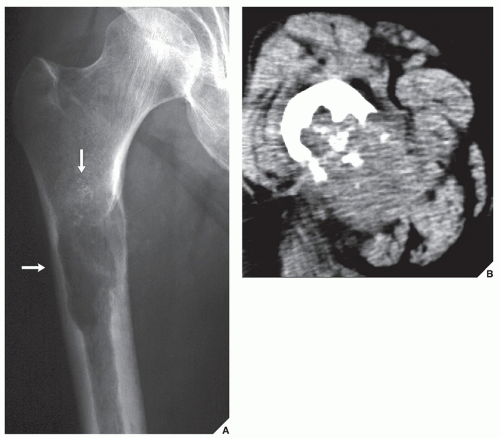 FIGURE 16.7 Soft-tissue extension of malignant tumor: effectiveness of CT. (A) Anteroposterior radiograph of the right proximal femur of a 70-year-old man shows a destructive lesion in the medullary portion of the bone (arrows) displaying focal chondroid calcifications. The soft-tissue extension of the tumor cannot be well evaluated. (B) Axial CT demonstrates a large soft-tissue mass, which on biopsy proved to be a chondrosarcoma. |
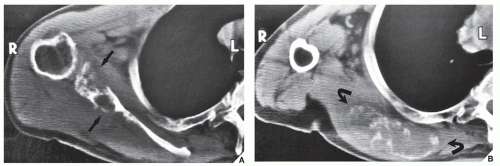 FIGURE 16.8 CT of chondrosarcoma. Standard radiographs were ambiguous in this 70-year-old man with a palpable mass over the right scapula. However, two CT sections demonstrate a destructive lesion of the glenoid portion and body of the scapula (arrows) (A), with a large soft-tissue mass extending to the rib cage and containing calcifications (curved arrows) (B). |
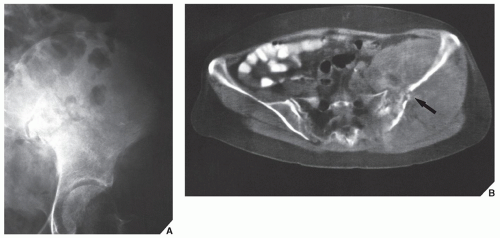 FIGURE 16.9 CT of osteosarcoma. (A) Standard anteroposterior radiograph of the pelvis was not sufficient to delineate the full extent of the destructive lesion of the iliac bone in this 66-year-old woman. (B) CT scan, however, showed a pathologic fracture of the ilium (arrow) and the full extent of soft-tissue involvement. The high Hounsfield values of the multiple soft-tissue densities suggested bone formation. Enhancement of the CT images with contrast agent showed an increased vascularity of the lesion. Collectively, the CT findings suggested a diagnosis of osteosarcoma that, although unusual for a person of this age, was confirmed by open biopsy. |
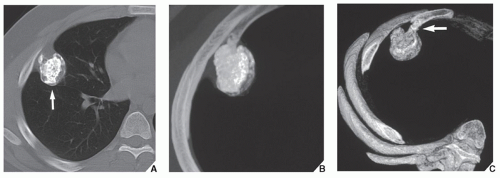 FIGURE 16.10 Osteochondroma: effectiveness of 3D CT. (A) Conventional CT section through the chest shows an osteochondroma at the site of the anteromedial portion of the right forth rib (arrow). It is difficult to determine if the lesion is sessile or pedunculated. (B) 3D CT reconstructed image in maximum intensity projection (MIP) delivers a much more informative image of osteochondroma and allows one to characterize the internal architecture of the lesion; note typical chondroid matrix of the tumor. (C) 3D CT reconstructed image in shaded surface display (SSD) renders better conspicuity of the lesion; the pedicle of osteochondroma (arrow) is now clearly demonstrated. (From Greenspan A, Jundt G, Remagen W. Differential diagnosis in orthopaedic oncology, 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2007.) |
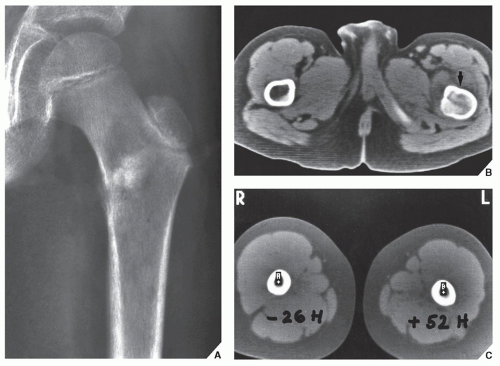 FIGURE 16.11 Osteosarcoma: effectiveness of CT. (A) Anteroposterior radiograph of the left proximal femur of a 12-year-old boy demonstrates an osteolytic lesion in the intertrochanteric region, with a poorly defined margin and amorphous densities in the center associated with a periosteal reaction medially—features suggesting osteosarcoma, which was confirmed on open biopsy. Because a limb-salvage procedure was contemplated, a CT scan was performed to determine the extent of marrow infiltration and the required level of bone resection. The most proximal section (B) shows obvious gross tumor involvement of the marrow cavity of the left femur (arrow). A more distal section (C) shows no gross marrow abnormality, but a positive Hounsfield value of 52 units indicates tumor involvement of the marrow, which was not shown on the standard radiographs. By comparison, the section of the right femur shows a normal Hounsfield value of -26 for bone marrow. |
 FIGURE 16.12 Osteosarcoma after chemotherapy: effectiveness of CT. Before surgery, this 14-year-old girl with an osteosarcoma of the left femur underwent a full course of chemotherapy. (A) CT section before the therapy was begun shows involvement of the bone and marrow cavity. Note the soft-tissue extension of the tumor, with heterogeneous, amorphous tumor bone formation. After combined treatment with doxorubicin hydrochloride, vincristine, methotrexate, and cisplatin, a repeat CT scan (B) shows calcifications and ossifications in the periphery of the lesion, which represents reactive rather than tumor bone and demonstrates the success of chemotherapy. Radical excision of the femur and a subsequent histopathologic examination showed almost complete eradication of malignant cells, confirming the CT findings. |
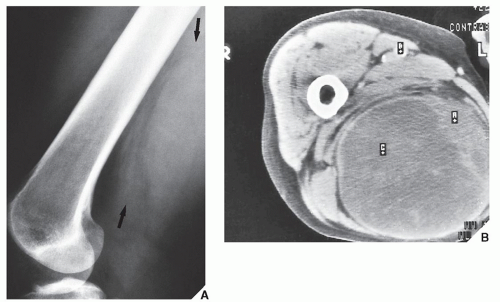 FIGURE 16.13 CT of malignant fibrous histiocytoma (MFH) of the soft tissue. A 56-year-old woman presented with a soft-tissue mass on the posteromedial aspect of the right thigh. (A) Lateral \ radiograph of the femur demonstrates only a soft-tissue prominence posteriorly (arrows). (B) CT section shows an axial image of the mass, which is contained by a fibrotic capsule. The overlying skin is not infiltrated. Despite the benign appearance, the mass proved on biopsy to be an MFH. |
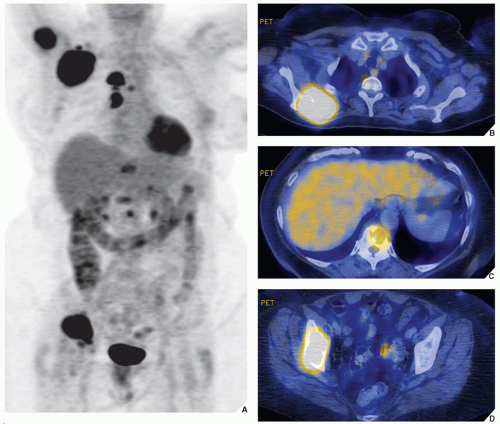 FIGURE 16.14 PET and PET-CT of metastases. A 61-year-old woman was diagnosed with lung carcinoma. (A) A whole-body PET scan shows several hypermetabolic foci in the internal organs, lymph nodes, and osseous structures, representing metastatic disease. The fused PET-CT images demonstrate metastatic lesions in the right scapula (B), thoracic vertebral body (C), and right ilium (D). |
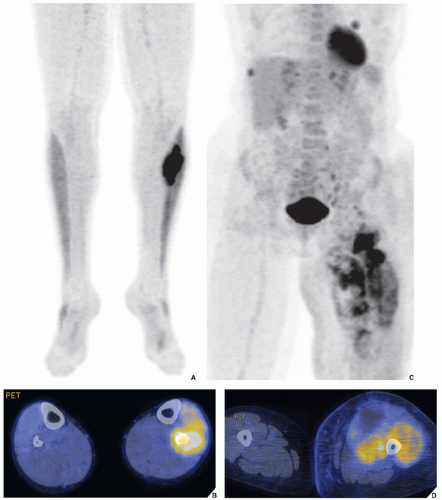 FIGURE 16.15 PET and PET-CT of primary bone and primary soft-tissue tumors. (A,B) A hypermetabolic focus in the proximal left fibula in a 23-year-old man proved to be an Ewing sarcoma. (C,D) A hypermetabolic lesion in the vastus lateralis and medialis in the proximal left thigh in a 58-year-old woman was diagnosed on histopathologic examination as MFH of the soft tissues. |
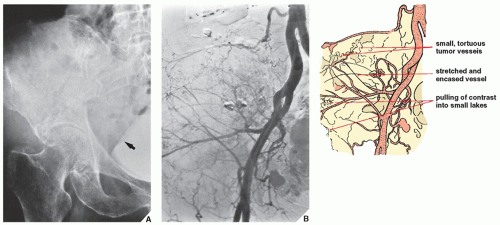 FIGURE 16.16 Arteriography of dedifferentiated chondrosarcoma. (A) Anteroposterior radiograph of the pelvis in a 79-year-old woman with an 8-month history of pain in the right buttock and weight loss demonstrates a poorly defined destructive lesion of the right iliac bone, with multiple small calcifications and a soft-tissue mass extending into the pelvic cavity. Note the effect of the mass on the urinary bladder filled with contrast (arrow). A chondrosarcoma was suspected, and a femoral arteriogram was performed as part of the diagnostic workup. (B) Subtraction study of an arteriogram demonstrates hypervascularity of the tumor. Note the abnormal tumor vessels, encasement and stretching of some vessels, and “pulling” of contrast medium into small “lakes”—all characteristic signs of a malignant lesion. Biopsy revealed a highly malignant, dedifferentiated chondrosarcoma. In this case, the vascular study corroborated the radiographic findings of a malignant bone tumor. |
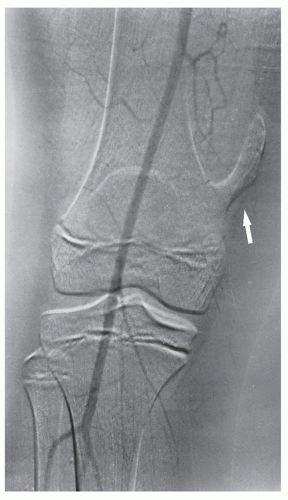 FIGURE 16.17 Arteriography of osteochondroma. A 12-year-old boy with osteochondroma of the distal femur (arrow) underwent arteriography to demonstrate the relationship of the distal superficial femoral artery to the lesion. This subtraction study shows no major vessels near the planned site of resection at the base of the lesion, important information for surgical planning. |
 FIGURE 16.18 Vertebral arteriography and embolization of hemangioma. A 73-year-old woman presented with a collapsed T11 vertebra, which showed a corduroy-like pattern suggestive of hemangioma. Vertebral angiography was performed. (A) Arteriogram of the 11th right intercostal artery outlines a vascular paraspinal mass associated with hemangioma and indicating extension of the lesion into the soft tissues. (B) After embolization, the lesion shows a marked decrease in vascularity. Subsequently, the patient underwent decompression laminectomy and anterior fusion at T10-11 using a fibular strut graft. |
images enhance tumor contrast with bone, bone marrow, and fatty tissue, whereas SE T2-weighted images enhance tumor contrast with muscle and accentuate peritumoral edema. Axial and coronal images have been used in determining the extent of soft-tissue invasion in relation to important vascular structures. However, in comparison with CT, MR images do not clearly demonstrate calcification in the tumor matrix; in fact, large amounts of calcification or ossification may be almost undetectable. Moreover, MRI has been shown to be less satisfactory than CT in the demonstration of cortical destruction. It is important to realize that both MRI and CT have advantages and disadvantages, and circumstances exist in which either can be the preferential or complementary study. But it is even more important that the surgeon tell the radiologist who is performing and interpreting the study what information is needed.
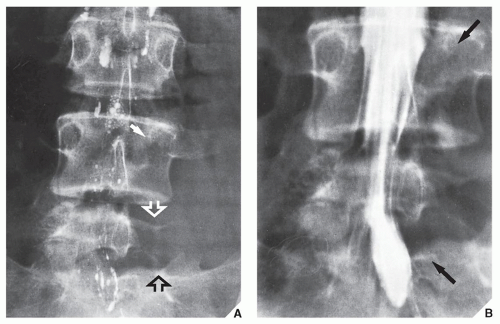 FIGURE 16.19 Myelography of aneurysmal bone cyst. Initial radiographic examination of the lumbar spine of this 14-year-old girl with an 18-month history of pain in the lower back and sciatica of the left leg did not disclose any abnormalities; myelography was performed because of suspected herniation of a lumbar disk, but it was inconclusive. A repeat study was requested when the symptoms became more severe after 3 months. (A) Posteroanterior radiograph of the lumbosacral spine shows destruction of the left pedicle of L4 (arrow) and the left part of the L5 body (open arrows). Note the residual contrast in the subarachnoid space. A repeat myelogram using a water-soluble contrast (metrizamide) shows, on the posteroanterior view (B), extradural compression of the thecal sac on the left side with displacement of the nerve roots (arrows). Biopsy confirmed the radiographic diagnosis of an aneurysmal bone cyst. |
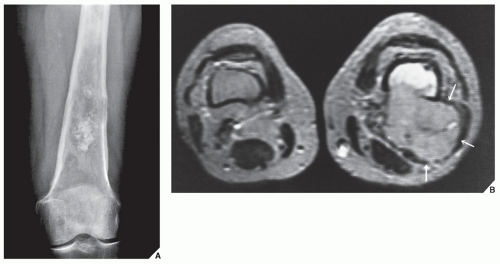 FIGURE 16.20 MRI of chondrosarcoma. (A) Conventional radiograph of the left femur in anteroposterior projection of a 67-year-old woman demonstrates a tumor in the distal shaft destroying the medullary portion of the bone and breaking through the cortex. The soft-tissue extension cannot be determined. (B) Axial T2-weighted MR image (SE; repitition time [TR] 2500/echo time [TE] 70 msec) demonstrates a tumor infiltrating bone marrow, destroying the posterolateral cortex, and breaking into the soft tissues with the formation of a large mass (arrows). Compare with a normal contralateral extremity. |
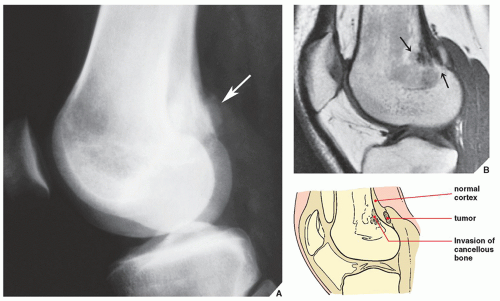 FIGURE 16.21 MRI of parosteal osteosarcoma. (A) From this lateral radiograph of the distal femur of a 22-year-old woman with parosteal osteosarcoma, it is difficult to evaluate if the tumor (arrow) is on the surface of the bone or already infiltrated through the cortex. (B) Sagittal T1-weighted MRI (SE; TR 500/TE 20 msec) demonstrates invasion of the cancellous portion of the bone, as represented by an area of low signal intensity (arrows). |
 FIGURE 16.22 MRI of MFH and osteosarcoma. (A) Coronal T1-weighted MRI (SE; TR 500/TE 20 msec) demonstrates involvement of the medullary cavity of the right femur in this 16-year-old girl with MFH (the entire tumor is not imaged on this study). Note the excellent demonstration of the interface between normal bone displaying high signal intensity and a tumor displaying intermediate signal intensity. (B) Coronal T1-weighted MRI in another patient with osteosarcoma of the distal femur demonstrates the intramedullary extension of the tumor. Again, note demonstration of sharp interface between tumor and not-affected bone. (C) Sagittal T2-weighted MRI shows a small focal area of cortical breakthrough in the anterior cortex of the distal femur (arrow) and posterior periosteal elevation (arrowhead). (D) Anteroposterior radiograph of the knee of another patient sows a sclerotic lesion within the medullary cavity of the proximal tibia (arrow). Note the subtle widening of the medial aspect of the physis (arrowhead), suspicious for trans-physeal extension of the tumor. (E) Coronal T1-weighted MRI of the proximal tibia outlines the intramedullary extent of osteosarcoma (long arrow), the extraosseous mass (short arrows), and confirms the extension of the tumor across the physis into the epiphysis (arrowhead). (F) Sagittal T2-weighted MR image demonstrates the intramedullary (long arrow) and extraosseous (arrowhead) extension of the tumor. Note the typical Codman triangle in the inferior aspect of the lesion (short arrow), and the surrounding bone marrow and soft-tissue edema. |
through an expanded interstitial space. The latest observation by Dewhirst and associates suggests that MR spectroscopy may also be useful in the evaluation of patients undergoing chemotherapy.
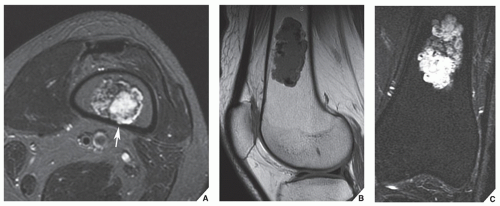 FIGURE 16.23 MRI of chondroid matrix. Axial T2-weighted (A), sagittal T1-weighted (B), and coronal short time inversion recovery (STIR) (C) images demonstrate a typical popcorn pattern of chondroid matrix in the bone marrow space of the distal femur. Note also the slight endosteal scalloping on the axial image (arrow). |
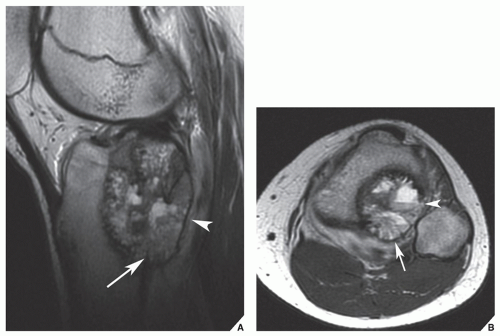 FIGURE 16.24 MRI of telangiectatic osteosarcoma. Sagittal T2-weighted MRI (A) shows the intramedullary extension of the tumor (arrow) and the invasion of the soft tissues posteriorly (arrowhead). Axial T2-weighted MR image (B) shows posterior extension of the tumor (arrow) and the presence of characteristic fluid-fluid levels (arrowhead). |
 FIGURE 16.25 Scintigraphy of the metastases. A radionuclide bone scan was performed on a 68-year-old woman with metastatic breast carcinoma to determine the distribution of metastases. After an intravenous injection of 15 mCi (555 MBq) of 99mTc diphosphonate, an increased uptake of the radiopharmaceutical agent is seen in the skull and cervical spine (A) and lumbar spine and pelvis (B), localizing the site of the multiple metastases. |
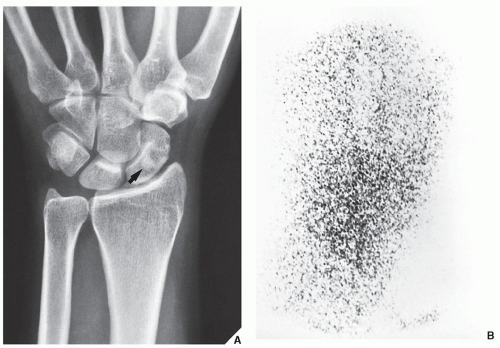 FIGURE 16.26 Scintigraphy of enostosis. A 32-year-old woman presented with pain localized in the wrist area. (A) Dorsovolar radiograph of the wrist demonstrates a sclerotic round lesion in the scaphoid (arrow), and a diagnosis of osteoid osteoma was considered. (B) Radionuclide bone scan reveals normal isotope uptake, ruling out osteoid osteoma, which is invariably associated with an increased uptake of radiopharmaceutical. The lesion instead proved to be a bone island (enostosis), an asymptomatic developmental error of endochondral ossification without any consequence to the patient. The pain was unrelated to the island, coming instead from tenosynovitis; it disappeared after the patient was treated for the latter condition. |
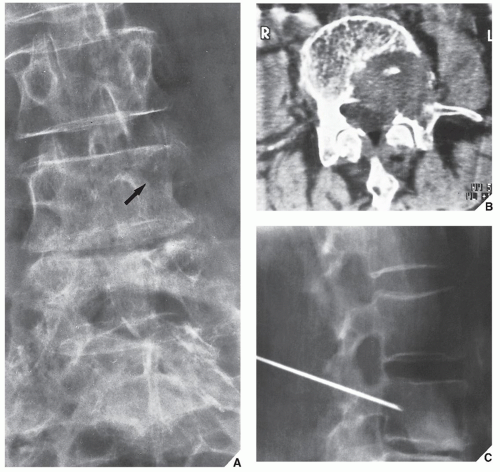 FIGURE 16.27 Percutaneous bone biopsy. (A) Anteroposterior radiograph of the lumbar spine in a 67-year-old woman with lower back pain for 4 months demonstrates destruction of the left pedicle of the L4 vertebra (arrow). (B) CT section shows, in addition, involvement of the vertebral body by the tumor. (C) Percutaneous biopsy of the lesion, performed in the radiology suite for the purpose of rapid histopathologic diagnosis, revealed a metastatic adenocarcinoma from the colon. |
 FIGURE 16.28 Diagnosis of bone lesion. Analytic approach to evaluation of the bone neoplasm must include patient age, multiplicity of a lesion, location in the skeleton and in the particular bone, and radiographic morphology. (From Greenspan A, Remagen W. Differential diagnosis of tumors and tumor-like lesions. Philadelphia: Lippincott-Raven Publishers; 1998.) |
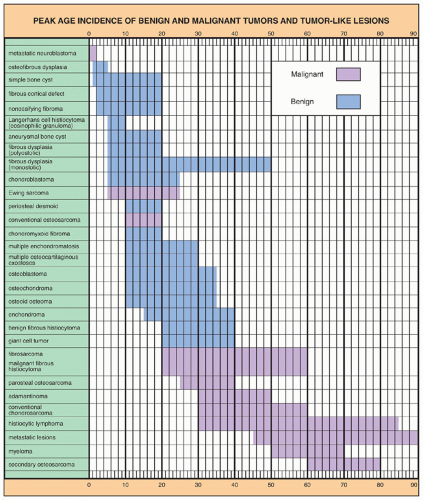 FIGURE 16.29 Peak age incidence of benign and malignant tumors and tumor-like lesions. (Data from Dahlin DC, 1986; Dorfman HD, Czerniak B, 1998; Fechner RE, Mills SE, 1993; Huvos AG, 1979; Jaffe HL, 1968; Mirra JM, 1989; Moser RP, 1990; Schajowicz F, 1994; Unni KK, 1988; Wilner D, 1982.) |
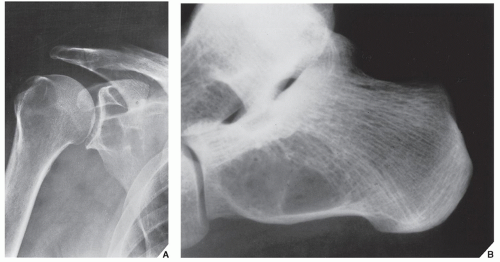 FIGURE 16.30 Simple bone cyst. (A) Anteroposterior radiograph of the right shoulder of a 69-year-old man with shoulder pain for 8 months demonstrates a welldefined radiolucent lesion with a sclerotic border in the glenoid portion of the scapula. Because the patient had a history of gout, the lesion was thought to represent an intraosseous tophus. In the differential diagnosis, an intraosseous ganglion and even a cartilage tumor were also considered. An excision biopsy, however, revealed a simple bone cyst, which is very unusual in the glenoid part of the scapula. (B) Lateral radiograph of the left hindfoot of a 50-year-old woman shows a radiolucent lesion in the calcaneus proven on the excision biopsy to be a simple bone cyst.
Related posts: Radiologic Evaluation of Skeletal Anomalies Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Anomalies of the Upper and Lower Limbs Anomalies of the Upper and Lower Limbs
 Upper Limb III: Distal Forearm, Wrist, and Hand Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|