Chapter 118 Overview: Acute renal failure is defined as a sudden loss of renal function that may be due to inadequate renal perfusion, renal cell injury, or obstruction to urine flow. Recently, the term “acute kidney injury” (AKI) has been proposed to replace the term acute renal failure and is gaining wide acceptance.1 AKI usually develops in hospitalized children as a result of systemic illness or its treatment and not from primary renal disease. The most common causes of AKI in children are renal ischemia, nephrotoxic drugs, and sepsis.2 Other important causes are listed in Box 118-1. AKI from any cause can lead to chronic kidney disease.3–7 Recovery of renal function depends on the underlying events leading to injury. Imaging: In general, sonography should be the first diagnostic imaging study performed in the workup of persons with AKI, and in most cases, it is the only imaging required. The role of sonography is to determine renal size and exclude anatomic abnormalities as the cause of AKI. The renal cortex, medulla, and collecting system have different acoustic properties, and pathologic changes are readily detected and correlate well with histologic findings. Doppler techniques provide information about renal perfusion and vascular abnormalities. Sonography also is used to localize the kidneys for percutaneous biopsy. More precise functional information may be obtained with nuclear medicine studies that can aid in differentiating between prerenal, renal, and postrenal causes of AKI. Prerenal Injury: In persons with prerenal injury, the kidney is intrinsically normal, and renal function is diminished as a result of decreased renal perfusion. Sonographic examination of the kidneys is normal. Restoration of renal perfusion results in a prompt return of renal function. Intrinsic Renal Disease: Renal ischemia due to a prolonged prerenal injury or a severe hypoxic/ischemic insult can lead to acute tubular necrosis. Imaging findings depend on the severity of parenchymal injury. A generalized increase in renal cortical echogenicity indicates intrinsic renal disease (Fig. 118-1). In mild cases, the kidneys may appear normal or may demonstrate slightly increased renal cortical echogenicity. Decreased corticomedullary differentiation may be noted. Doppler flow may be normal in mild disease, whereas poor peripheral perfusion and diminished arterial diastolic flow due to increased peripheral vascular resistance occur in more severe cases. Figure 118-1 Hemolytic-uremic syndrome. Nephrotoxic drugs commonly associated with AKI include antibiotics, chemotherapeutic agents, and nonsteroidal antiinflammatory medications.8 Some agents such as aminoglycoside antibiotics cause tubular injury. Methicillin and other penicillin analogues, cimetidine, sulfonamides, rifampin, and nonsteroidal antiinflammatory drugs may cause acute interstitial nephritis, which is thought to be related to a hypersensitivity reaction with development of antitubular basement membrane antibodies in some cases. Children with acute lymphocytic leukemia and B-cell lymphoma are at risk for the development of uric acid nephropathy and tumor lysis syndrome. One mechanism of injury believed to be of importance in uric acid nephropathy is precipitation of uric acid crystals in the renal microvasculature leading to obstruction of renal blood flow, or precipitation in the renal tubules leading to obstruction of urine flow. Tumor lysis syndrome is a constellation of metabolic abnormalities resulting from spontaneous or treatment-related tumor necrosis. As tumor cells are lysed, rapid increases in serum potassium, uric acid, and phosphorus occur, with a decrease in serum calcium. Patients who are treated with allopurinol, a purine analog used to diminish the excretion of uric acid, instead excrete large quantities of the uric acid precursors xanthine and hypoxanthine. Precipitation of these compounds is thought to play a role in the development of AKI. In patients who are in septic shock, AKI can develop from hypotension, leading to renal ischemia and acute tubular necrosis, or AKI can develop as a result of the use of nephrotoxic medications. Obstructive Uropathy and Lower Tract Lesions: A urinary tract obstruction can develop in persons with AKI if the obstruction affects a solitary kidney, both ureters, or the urethra. Congenital causes include ureteropelvic junction obstruction, ureterovesical junction obstruction, and posterior urethral valves. Acquired urinary tract obstruction can be caused by urinary tract stones or, rarely, tumors. Bladder rupture is another rare cause of AKI associated with ascites. Bladder rupture in children usually is due to trauma; it also can occur as a complication of infection, chemotherapy, and radiotherapy.9,10 Overview: The terms “chronic renal failure” and “chronic renal insufficiency” have been used historically to describe varying degrees of renal dysfunction. Currently, the term chronic kidney disease (CKD) is used by both adult and pediatric nephrology communities throughout the world.11 The classification of CKD published by the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative is based on the estimated glomerular filtration rate and is applicable to children older than 2 years and to adults.12 The classification categorizes CKD into five different stages and is widely used in clinical practice (Table 118-1). Recently it has been recognized that most patients with CKD (estimated to be one in eight adults) never reach end-stage renal disease and the need for renal replacement therapy because they are at risk for accelerated cardiovascular disease and are more likely to die prematurely from cerebrovascular or cardiovascular disease.13 Therefore clinical management requires measures to diminish cardiovascular risk factors in both adult and pediatric patients. According to the North American Pediatric Renal Trials and Collaborative Studies 2007 report,14 the most common causes of pediatric CKD in North America are congenital disorders such as obstructive uropathy, renal dysplasia, and reflux nephropathy (Fig. 118-2; Table 118-2). In contrast, in Japan, 34% of pediatric CKD is due to glomerulonephritis, primary focal segmental glomerulosclerosis, and immunoglobulin A nephropathy.15 In Jordan16 and Iran,17 where consanguinity is more common, heritable disorders such as cystic kidney disease, primary hyperoxaluria, cystinosis, Alport syndrome, and congenital nephrotic syndrome represent a greater proportion of cases of CKD. In the developing world, acquired causes of CKD predominate, particularly infection-related glomerulopathies.18,19 The worldwide incidence and prevalence of CKD is greater for boys than for girls because of the higher incidence of congenital causes of CKD in boys.14–21 Table 118-1 Kidney Disease Outcomes Quality Initiative Stages of Chronic Kidney Disease GFR, Glomerular filtration rate. From VanDeVoorde RG, Warady BA. Management of chronic kidney disease. In: Avner ED, ed. Pediatric nephrology. 6th ed. Berlin: Springer-Verlag; 2009. Table 118-2
Renal Failure and Transplantation
Acute Renal Failure
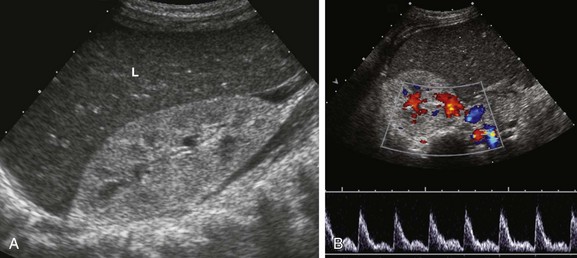
A, A sonogram of an 18-month-old boy with impaired renal function shows an enlarged right kidney with parenchymal echogenicity greater than that of the adjacent liver (L) and decreased corticomedullary differentiation. B, A pulsed Doppler waveform from the main renal artery shows diminished diastolic flow.
Chronic Renal Failure
Stage
Description
GFR (mL/min/1.73 m2)
1
Kidney damage with normal or increased GFR
≥90
2
Kidney damage with mild decrease in GFR
60-89
3
Moderate decrease in GFR
30-59
4
Severe decrease in GFR
15-29
5
Kidney failure
<15 (or dialysis)
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







