George M. Bridgeforth and Kris Alden
A 63-year-old woman complains of right-sided rib pain after falling on the street. She reports moderate soreness that worsens when she tries to take a deep breath. She notes marked tenderness of the right chest wall as well.
CLINICAL POINTS
- The cause of rib fractures is usually direct trauma or falls.
- The middle ribs are the most likely to be fractured.
- Decreased breath sounds with hyperresonance to percussion may be a sign of a pneumothorax.
Clinical Presentation
Fracture of one or more ribs is a common chest injury. Generally, rib fractures result from direct trauma or falls sustained in sports activities or motor vehicle accidents. Most often, the middle ribs (4th through the 8th ribs) are fractured (Fig. 50.1). Fractures of the first rib are uncommon but may be associated with serious injuries to the mediastinum (aortic transection), brain, or cervical spinal cord. Although rib fractures occur in both adults and children, children seem to be less vulnerable because their bones are somewhat more flexible. Nontraumatic rib fractures occur more often in older women who have osteoporosis.
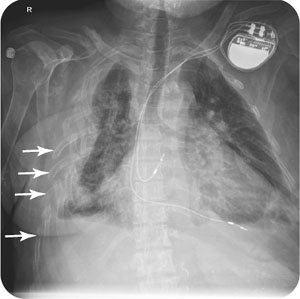
Patients with acute rib fractures may present with bruising, swelling, marked focal tenderness of the fractured ribs. There is diminished chest wall expansion due to pain and guarding. Decreased breath sounds (from diminished lung expansion) are a common finding with severe chest wall contusions and rib fractures. Absent breath sounds may be secondary to an associated pneumothorax or a traumatic effusion in the lower lung fields. A pneumothorax may occur with or without a rib fracture. Therefore, it is imperative to order a chest radiograph and rib films (see section, “Radiographic Evaluation”). Although some experts would argue that chest radiographs alone are sufficient.
Decreased breath sounds with dullness to percussion at the base may represent an effusion.
It is necessary to check for respiratory distress (decreased or absent breath sounds, rapid heart rate, rapid respiratory rate with shallow breathing). In addition, the examiner should verify that there are no effusions (dullness at the base with absent breath sounds) or pneumothorax (hyperresonance with percussion, decreased breath sounds). Tension pneumothoraces with flail chests are rare but are serious emergencies. It is also important to check for tension pneumothorax (deviated trachea directed away from the pneumothorax with marked respiratory distress). Patients with displaced rib fractures affecting three or more adjacent ribs may have a flail chest. A flail chest may be accompanied by a sucking or a whistling noise.
PATIENT ASSESSMENT 
- Pain when breathing or with movement
- Bruising and focal tenderness of the chest wall
- Decreased breath sounds on the affected side
- Possible associated cervical and abdominal injuries
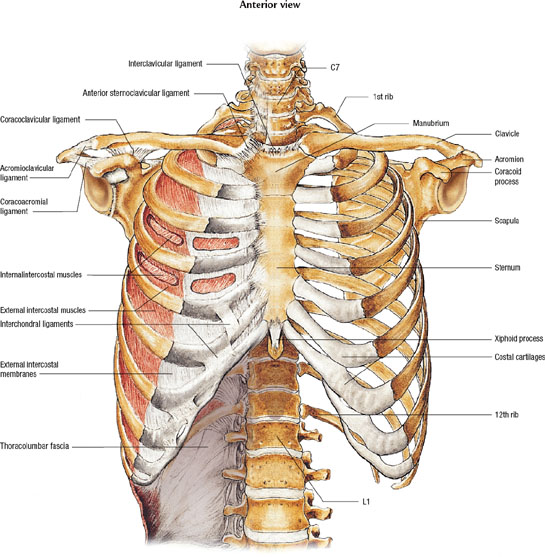
FIGURE 50.1 Most rib fractures affect the middle ribs (4th to 8th). Fractures involving the upper ribs may be associated with cervical spinal cord or traumatic head injuries. Fractures involving the lower chest wall may be associated with abdominal trauma (lacerations of the liver, acute pancreatitis, or a ruptured spleen). Asset provided by Anatomical Chart Co.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


