Target volumes
Definition and description
GTV70 a (the subscript 70 denotes radiation dose delivered)
Parotid or submandibular primary: all gross disease on physical examination and imaging
Neck nodes: all nodes ≥ 1 cm in short axis diameter or nodes with necrotic center
CTV70
Add 5 mm so that GTV70 + 5 mm = CTV70
For nodes that are small but suspicious for disease (i.e., <1 cm), can consider a lower dose of 63–66 Gy
PTV70
Margin specific to treatment center and less if image guidance available
Typically CTV70 + 3 to 5 mm = PTV70
Table 2
Suggested target volumes at the high-risk subclinical region
Target volumes | Definition and description |
|---|---|
CTV60 | Parotid or submandibular CTV60 should encompass the entire GTV or the surgical bed for postoperative patients |
Landmarks for the parotid surgical bed | |
Superior: zygomatic arch | |
Anterior: masseter muscle | |
Lateral: soft tissue of neck | |
Medial and inferior: styloid process at depth | |
Posterior: mastoid bone | |
Landmarks for the submandibular surgical bed: include the entire surgical bed, all postoperative changes, and use the contralateral submandibular gland as a guide | |
Highly consider a boost of 6–10 Gy to residual disease or positive margins. The surgeon should be encouraged to leave clips where possible for localization | |
CTV50 | Clinically node-positive tumors |
Electively irradiate rest of the ipsilateral neck (levels Ib–V) to 50 Gy | |
Clinically node-negative tumors | |
Ipsilateral neck: include at least levels Ib–III for high-grade or large (T3–T4) tumors. Adenoid cystic or acinic cell cancers typically do not require elective nodal irradiation because of the low risk of lymphatic spread | |
Contralateral neck | |
Parotid tumors: consider treating when clinically concerned, e.g., multiple nodes <1 cm | |
Submandibular tumors: treat contralateral levels I–III for tumors close to midline | |
PTV60 | Margin specific to treatment center and less if image guidance available |
Typically CTV60 + 3 to 5 mm = PTV60 |
5 Plan Assessment
For superficial tumors or tumors with skin infiltration, a bolus of 0.5 to 1 cm should be applied to ensure adequate surface coverage.
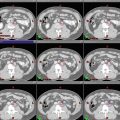
Intensity-modulated radiation therapy (IMRT) planning parameters follow the standard head and neck radiation therapy norms. Normal tissue constraints follow the Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC) recommendations. Of note, for unilateral radiation, we recommend a stricter dose constraint for the contralateral parotid gland (<20 Gy mean dose) compared to <25 Gy mean dose if there is bilateral irradiation (Figs. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, and 12).