• 3 well-recognized, but uncommon, hepatic syndromes: Chronic intrahepatic cholestasis, portal hypertension, and Budd-Chiari syndrome
• Angiotensin-converting enzyme elevated in 60% of patients with sarcoidosis; nonspecific and generally not useful in following course of disease
DIAGNOSTIC CHECKLIST
• Both lung disease and nodes may be FDG avid and mimic malignancy
• Do not assume that heterogeneous hepatomegaly and abdominal lymphadenopathy are always malignant
(Left) Axial NECT shows bilateral hilar lymphadenopathy in the thorax, including some calcification.
(Right) The lung windows in the same case show micronodularity along the bronchial tree, characteristic of pulmonary sarcoid.
(Left) Axial CECT in the same case shows a nodular liver with widened fissures; this appearance might be mistaken for cirrhosis. Subtle hypodense foci in the liver and spleen indicate the granulomatous nature of the pathology.
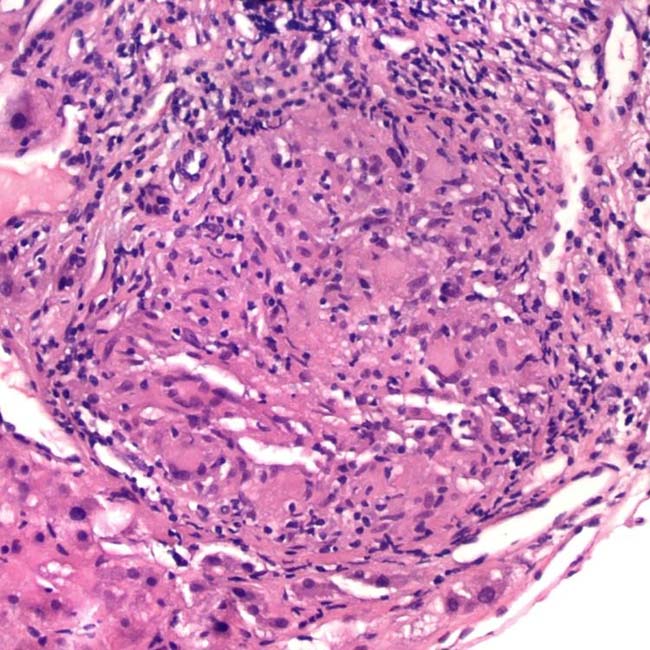
(Right) In H&E stain of a photomicrograph, a large epithelioid, noncaseating granuloma is seen in a liver biopsy from a case of sarcoidosis with ductopenia. (Courtesy J. Misdraji, MD.)
TERMINOLOGY
Synonyms
• Boeck sarcoid
Definitions
• Relatively common, chronic, multisystem disease of unknown origin characterized by presence of noncaseating epithelioid granulomas
IMAGING
General Features
• Best diagnostic clue
Multifocal small hypodense lesions (granulomas) in liver and spleen in young patient with lymphadenopathy






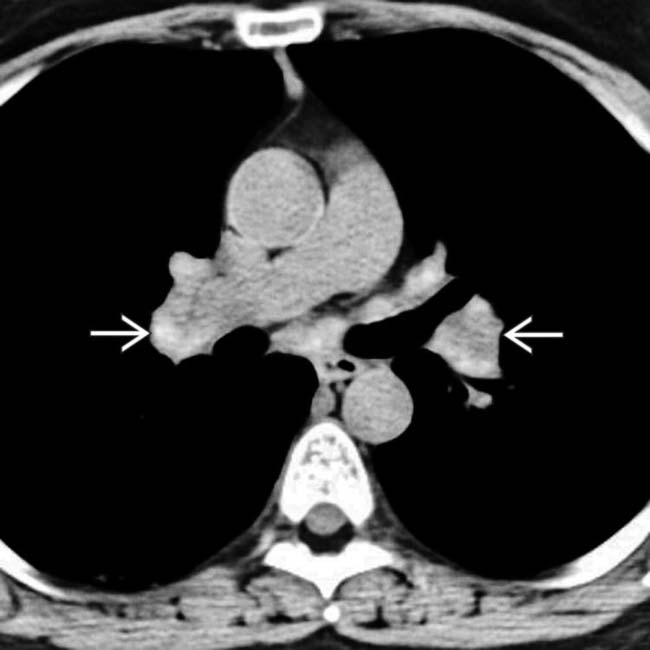
 in the thorax, including some calcification.
in the thorax, including some calcification.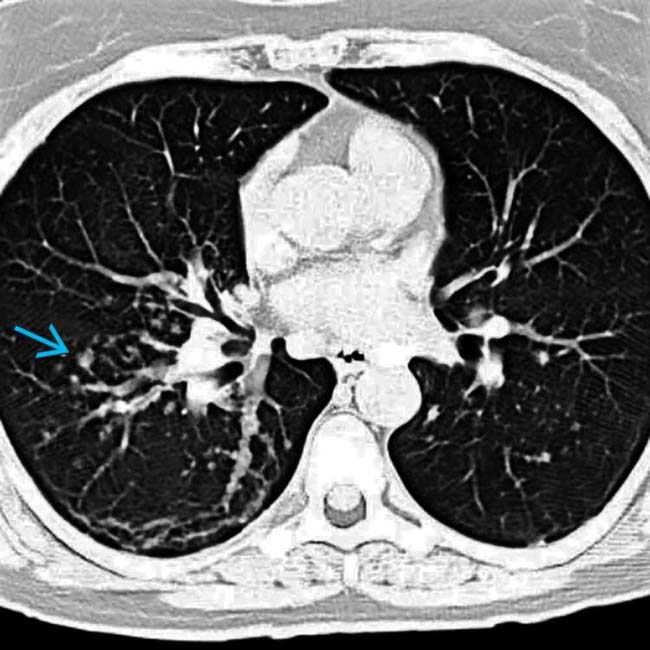
 along the bronchial tree, characteristic of pulmonary sarcoid.
along the bronchial tree, characteristic of pulmonary sarcoid.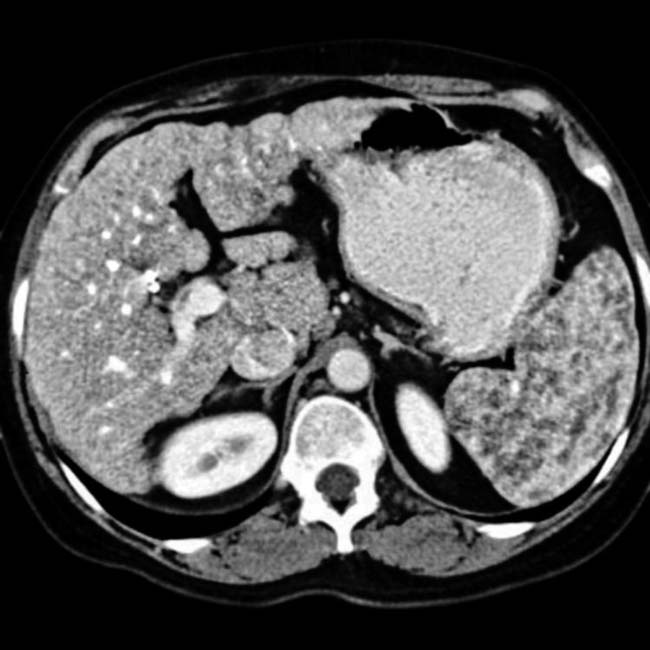






























 CT and MR are more sensitive than US
CT and MR are more sensitive than US





