(1)
Department of Radiation Oncology, University of Colorado Denver, Aurora, CO, USA
(2)
Department of Radiation Oncology, MD Anderson Cancer Center, Houston, TX, USA
Pediatric sarcomas are a diverse group of diagnoses. The three most common types that involve radiation therapy for local control are Ewing sarcoma (EWS), rhabdomyosarcoma (RMS), and non-rhabdomyosarcoma soft tissue sarcoma (NRSTS). In this chapter, we will discuss the treatment of EWS and RMS which are predominantly seen in the pediatric and young adult population.
1 Anatomy and Patterns of Spread
EWS and RMS can occur in essentially any location of the body. EWS is most commonly located in the extremity followed by the pelvis, while RMS is most commonly seen in the head and neck region followed by the extremity and genitourinary sites. As such, a general description of relevant normal anatomy is beyond the scope of this chapter.
There are some general guidelines regarding patterns of spread for these two tumors. Uninvolved bone and intraosseous membranes typically provide boundaries for microscopic spread. Also, the margin to create the clinical target volume (CTV) is less compared to the typical adult NRSTS, secondary to the inherent sensitivity of most of these tumors to the combination of chemotherapy and radiotherapy.
Volume reduction is performed for “pushing” rather than invasive such as tumors that displace the lung, intestine, or bladder that show clear return to a more normal anatomic position after chemotherapy.
Nodal regions are not electively treated for EWS or RMS. While the nodal metastasis is uncommon in EWS, it is seen in approximately 15–50 % of RMS arising in the extremity and genitourinary sites. It is believed that subclinical involvement of nodal regions is appropriately addressed by chemotherapy, and only gross or microscopic nodal disease receives additional treatment in the form of radiotherapy.
2 Diagnostic Imaging for Target Volume Definition
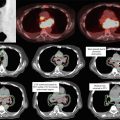
Both CT scans and MRI scans are helpful for definition of the gross tumor volume (GTV) and the CTV.
CT scan provides better definition of bony involvement, while MRI provides better definition of soft tissue involvement.
The role of positron emission tomography (PET) scans in pediatric sarcomas is still unclear, but increasingly is used to help delineate the gross tumor volume.
3 Target Volume Delineation and Treatment Planning
For EWS, target volumes include an initial target volume defined at presentation prior to chemotherapy or surgery (GTV1, CTV1) and a volume reduction defined after chemotherapy and surgery (GTV2, CTV2). An additional margin is added to the CTV to account for treatment setup uncertainty to create the PTV (PTV1 for the initial volume and PTV2 for the boost volume). See Table 1 for additional target definitions. Suggested doses (based on the Children’s Oncology Group protocol AEWS1031) are given in Table 2.
Table 1
Ewing sarcoma volume definitions
Initial target volumes
Definition and description
GTV1
Gross disease (including unresected enlarged lymph nodes) at presentation, prior to chemotherapy or surgery. GTV1 can be modified for tumors that extend into body cavities, such as the pelvis or thorax that regress with chemotherapy. In these cases, the edge of GTV1 can be defined as the post-chemotherapy volume
CTV1
GTV1 + 1 cm. CTV1 includes involved (pathologically or clinically) nodal regions
PTV 1
CTV1 + institutional setup margin
Volume reduction
GTV2
Residual tumor after induction chemotherapy. For definitive radiation therapy, include all initial areas of bony involvement
CTV2
GTV2 + 1 cm
PTV2
CTV2 + institutional setup margin
Table 2
Ewing sarcoma doses in 1.8 Gy per fraction
PTV1 (Gy)
PTV2 (Gy)
Definitive radiotherapy (all sites except vertebra)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access