Chapter 135 The term scoliosis is defined as a structural lateral curvature of the spine in a coronal plane greater than 10 degrees, as measured by the Cobb method on a standing radiograph.1 Curves less than 10 degrees are termed spinal asymmetry. The lateral curvature is often accompanied by abnormalities in the axial and the sagittal planes rendering it a three-dimensional abnormality, an important concept that influences assessment and management. Scoliosis is classified into various categories, according to etiology, curve location, age at onset, and curve type. The Scoliosis Research Society has classified scoliosis into the following broad subcategories:2 1. Idiopathic (infantile, juvenile, and adolescent) 2. Congenital (osteogenic and neuropathic) 3. Neuromuscular (neuropathic and myopathic) 4. Developmental syndromes (dysplasias and dysostosis) Scoliosis is a three-dimensional deformity involving the coronal, sagittal, and axial planes. The initiation and progression of the scoliotic curve is commonly thought to result from the effect of Hueter-Volkmann law, which states that epiphyseal growth (ring apophysis of the vertebral body) in the skeletally immature is inhibited when a compressive force acts on it and stimulated when a distraction force is applied.1,3 An initial abnormality in the axial plane leads to more compressive forces on the ventral aspect of vertebral body or disc and less on the posterior aspect. This discrepant growth of the anterior part versus the posterior part of the spine is accentuated over time, particularly during rapid skeletal growth, leading to eventual differential growth of the left and right sides of the spine, with suppression of growth on the concave side and excessive growth on the convex side eventually leading to scoliosis.3 This asymmetric growth not only forms the genesis of the curve but may also have significant surgical implications, as the pedicles on the concave side become asymmetrically smaller, posing a surgical challenge in pedicle screw for spinal fixation.4 An understanding of the nomenclature and methods of measurement used to describe scoliosis on radiographs is essential for radiologists (Fig. 135-1). Identification of the curve apex or the apical vertebra, significant vertebrae, and central sacral vertebral line (CSVL) is not only crucial for denoting the curve type, assessing curve stability, and selecting the surgical approach and instrumentation system but also for determining the optimal level for fusion.5,6 Figure 135-1 Nomenclature. • CSVL: CSVL is a vertical line that is drawn perpendicular to an imaginary tangential line drawn across the top of the iliac crests bisecting the sacrum. This is used to identify the stable vertebrae, evaluate coronal balance, and determine the curve type, independent of the curve classification system applied.5–7 • Apex: Apex is defined as the vertebra or the disc that is farthest from the CSVL and the most rotated and horizontal vertebra. • End vertebrae: The vertebrae with the maximum tilt or angulation toward the apex or concavity of the curve. They usually demarcate the proximal and distal vertebral bodies of the curve and are used to measure the Cobb angle. • Stable vertebra: The vertebral body at the distal and proximal aspect of the curve that is bisected or nearly bisected by the CSVL. • Neutral vertebrae: These represent the most nonrotated vertebrae and may be at the same level as end vertebrae or proximal or distally within the curve. • Plumb line: This represents the vertical line drawn downward on standing radiographs from the center of the C7 vertebral body to assess coronal and sagittal balance. Measuring the distance between the CSVL and the plumb line assesses coronal balance. Sagittal balance is evaluated by measuring the distance between the posterosuperior aspect of the S1 vertebral body and the plumb line. An abnormal coronal and sagittal balance is defined if the distance is greater than 2 cm. A plumb line located to the right of the CSVL reflects positive coronal balance and a line located to the left of the CSVL reflects negative coronal balance. Similarly, a plumb line that is anterior to the posterosuperior aspect of the S1 body is considered positive sagittal balance, whereas a plumb line that is posterior to the posterosuperior aspect of the S1 body is considered negative sagittal balance.5–8 • Sagittal balance: The primary sagittal curves, which are present since birth, include the thoracic and sacral kyphoses. The secondary curves, which are acquired to assume bipedal stance, include the cervical and lumbar lordoses. This normal mature pattern of sagittal alignment is established by age 6 years.9,10 Thoracic kyphosis ranges between 10 and 50 degrees and is measured from T5 to T12 with apex usually at T6-T8. Lumbar lordosis ranges from 35 to 80 degrees when measured from L1 to L5, with apex between L3 and L4.1,11,12 In scoliosis, the thoracic kyphosis is mainly influenced by the spinal deformity, whereas lumbar lordosis is mainly influenced by pelvic configuration.13 Most thoracic idiopathic scoliosis is associated with a decrease in normal thoracic kyphosis. A true kyphotic component may indicate a congenital or neuromuscular origin; however, some idiopathic cases may have a true kyphotic component.1,6,13 Positive sagittal balance is more significantly associated with pain and disability than curve magnitude, curve location, or coronal imbalance.13,14 • Curve location: This is defined on the basis of the location of the apical vertebra and is classified as cervical (apex between C2 and C6), cervicothoracic (C7–T1), thoracic (T2–T11), thoracolumbar (T12–L1), lumbar (L2–L4), or lumbosacral (L5 and below).1,6,13 • Curve types: The curve is classified broadly as primary (major) or secondary (minor) curves, or structural or nonstructural curves. Primary curves are the first to appear and are the largest abnormal curves. Secondary curves usually develop later to stabilize the position of the head and pelvis.6,13–15 A structural curve is a curve that is not correctable on side-bending views or on traction and is accompanied by vertebral rotational abnormalities. A nonstructural curve usually corrects on bending views and may be secondary curves or functional curves (curves related to posture, secondary to leg length discrepancy, muscle spasm, etc.).13 Curves that are 25 degrees or greater on the standing anteroposterior radiograph and do not decrease to less than 25 degrees on the side-bending radiographs should be considered structural.16 A curve less than 25 degrees on the standing anteroposterior radiograph may be deemed structural if the regional sagittal profile reveals a kyphosis +20 degrees or greater.16 If a curve is considered structural, it should be included in the fusion surgery. • Classification of curves: Various different classification systems exist describing the curve types preoperatively. The importance of classification systems is that they help guide the surgical approach and help compare the efficacy of different treatment methods.6,13 The Lenke classification system is the most recent and widely used classification system, replacing the established King-Moe classification system. The Lenke system is considered more comprehensive, complete, and reliable and takes into account the three-dimensional nature of scoliosis as opposed to the two-dimensional approach of the King-Moe classification.6,13,16,17 The Lenke system divides curves on the basis of location and type, differentiates structural from nonstructural curves, includes lumbar and sagittal modifiers, and proposes that only major curves and minor structural curves should be included in spinal arthrodesis.16,17 For unknown reasons, the typical curve in adolescent idiopathic scoliosis is usually a thoracic curve with right-sided convexity. Idiopathic scoliosis constitutes 80% of the patients with spinal deformity and is a diagnosis of exclusion.1 A judicious use of various imaging is a necessary prerequisite to exclude other underlying causes of scoliosis before labeling any case as idiopathic. Etiologies, Pathophysiology, and Clinical Presentation: The reported prevalence of idiopathic scoliosis in children and adolescents ranges from 0.5 to 3 per 100.1,18,19 In the mild curves (<20 degrees), the female-to-male ratio is 1 : 1, but, when greater and progressive curves are evaluated (>30 degrees), females predominate with a 5 : 1 to 7 : 1 ratio. Only 0.2% of children have severe curves (>30 degrees).1,19,20 Idiopathic scoliosis is further divided into the following types based on age at diagnosis: infantile (0-3 years); juvenile (4-10 years); adolescent (11-17 years); and adult (≥18 years). Age at onset has prognostic significance both in terms of underlying neuraxis abnormality as a cause of scoliosis and the natural history of the curve. Whether juvenile scoliosis is truly a separate entity, is debatable because of the high prevalence of associated abnormalities in preadolescent scoliosis by magnetic resonance imaging (MRI).2 Moreover, the demarcation is further obscured by the possibility of early existence of the established adolescent curve. Hence the terms early onset and late onset are increasingly being used to classify scoliosis after the age of 5 years.2,21 The rationale behind this distinction is the increased risk of cardiopulmonary compromise in children before age 5 years with larger curves.2,22 Imaging: The role of imaging in scoliosis is early detection and characterization of the type of curve and its severity, assessment of disease progression, definition of the need and timing of the surgery, monitoring of changes related to treatment, and identification of those cases in which an underlying structural anomaly is present.23 The extent and type of imaging is also governed by the category of scoliosis. Cross-sectional imaging is extensively used in congenital scoliosis to identify and characterize structural anomalies, whereas radiography is principally utilized in idiopathic scoliosis to monitor curve progression.2 Screening: Upright, standing, posteroanterior radiograph of the entire spine is the standard initial screening examination, once the deformity is suspected clinically. The radiograph should include the cervicothoracic junction, enough of the pelvis to show the iliac crest in full extent, and the triradiate cartilage to enable assessment of skeletal maturity. Although standing radiography is preferred, sitting or supine radiography may be the only alternative in young patients, patients with congenital scoliosis, or patients with severe neuromuscular disorders. The rationale behind standing radiography is that treatment methods are based on standing views and the magnitude of the curve is greatest in the standing position. This is an important consideration in congenital and infantile scoliosis when young patients with scoliosis start to ambulate. It is easy to mistake change in curvature as curve progression if the upright radiograph is compared with a prior supine radiograph.1 The patient should stand with the feet placed shoulder width apart, looking straight ahead with the elbows bent and knuckles in the supraclavicular fossa bilaterally, allowing visualization of the upper thoracic region on the lateral radiographs.24 A lateral radiograph is not required at the time of screening but should be obtained in patients with documented scoliosis to assess sagittal balance. Radiographic techniques should minimize radiation exposure, especially to sensitive organs (e.g., breast, thyroid, and lens of eyes). A posteroanterior technique involves less radiation to the breast compared with an anteroposterior technique. The image may have a grid that helps identify deviations of the spine from the plumb line. When surgical treatment is considered, side-bending radiographs are acquired to differentiate between structural and nonstructural minor curves to help guide the optimal level of fusion. Various techniques used to obtain side-bending radiographs include supine bending, standing bending, and bending over a bolster. Curve Magnitude: The Cobb angle is the accepted standard for assessing the magnitude of the scoliotic curve. It is defined as the angle formed by the intersection of two lines, one parallel to the end plate of the superior end vertebra and the other parallel to the end plate of the inferior end vertebra. Alternatively, pedicles may be used to calculate the Cobb angle when the end plates are poorly defined because of radiographic technique or obscured because of the severity of the curve. Although the Cobb angle provides limited assessment of the deformity and does not take rotation into account, it is still the foundation for diagnosis, follow-up, and treatment.1 The angle may be plotted manually or digitally with equal reliability.25 It is important to note that multiple factors, including patient positioning, radiographic techniques, known diurnal variation of 5 degrees, and interobserver and intraobserver variability, may affect the reproducibility of the angle.26–30 A progressive curve is usually defined by a Cobb angle increase of 5 degrees or more between consecutive radiographic examinations.1,2,6 The Cobb angle may decrease because of prone positioning and anesthesia during surgery, which sometimes leads to a postoperative rebound effect, with loss of correction when the patient returns to the standing position.6,13 Despite multiple caveats, measurements of the Cobb angle are usually considered reproducible, particularly when measuring end plates, patient positioning and techniques are kept constant. Assessing Curve Progression: Prognosis and management in scoliosis is highly specific to the case and the surgeon but is usually governed by three important factors: (1) etiology, (2) magnitude and the type of the curve at presentation, and (3) speed of curve progression. The risk of progression is directly related to the spinal growth remaining, the severity of the curve at presentation, and the gender of the patient.1,10,19,31,32 Various clinical tools to assess residual growth potential include chronologic age, menarche in girls, serial height measurements, and Tanner staging.10,19,33–37 In general, the onset of the adolescent growth spurt occurs at 13 years in boys and 11 years in girls, with menarche indicating the declining phase of the growing peak and a low risk of progression for idiopathic curves under 30 degrees.1,10,33,35 Various radiographic parameters may indicate remaining potential growth. Development of the iliac bone apophysis, quantified by Risser, has become a universally accepted sign (Fig. 135-2). Despite the wide use of the Risser grade as a measure of maturity, the appearance of the iliac apophysis generally occurs after the most important period of rapid growth.1,33,34 Given the inaccuracies related to the Risser grade, other radiographic parameters are used to assess bone maturation. Bone age may be assessed from a hand and wrist radiograph; however, use of bone age becomes less accurate in the juvenile age group secondary to the larger standard deviation and suffers from interobserver variability.1,38 Assessment of pelvic triradiate cartilage is considered more accurate than the Risser grade. The triradiate cartilage closes around age 11 years in girls at the time of peak growth velocity.1,23 The physis of the olecranon of the elbow closes at age 13 years, shortly before menarche and may also be used to assess remaining skeletal growth.23 Unfortunately, many of the above-mentioned markers of maturity are quite variable and may be difficult to put in proper context without an accurate record of prior growth performance. Sometime, more than one imaging parameter is taken into consideration for accurately assessing skeletal maturation. Figure 135-2 Risser grade. With regard to curve patterns, curves with an apex above T-12 are more likely to progress compared with isolated lumbar curves.1 With regard to curve magnitude
Scoliosis
Biomechanics and Pathogenesis
Terminology
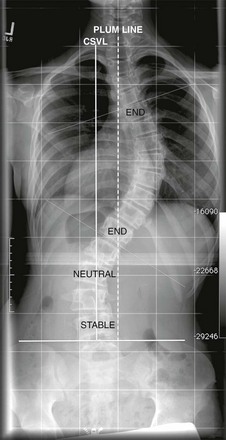
Standing posteroanterior radiograph from a patient with scoliosis: central sacral vertebral line (CSVL) (solid line) is a line that is perpendicular to a tangent across the iliac crest, bisecting the sacrum. The stable vertebra is the vertebra that is bisected or nearly bisected by the CSVL. The end vertebrae are the vertebra that are most tilted along the curve. Tangents (thin dotted-dash line) are drawn along the superior end plate of superior end vertebra and inferior end plate of inferior end vertebra to calculate the Cobb angle. A neutral vertebra is one that is not rotated. The plumb line is a line that is drawn from the center of the C7 vertebral body and is parallel to the edge of the image. If the distance between the CSVL and the plumb line is 2 cm or greater, it indicates coronal imbalance.
Idiopathic Scoliosis
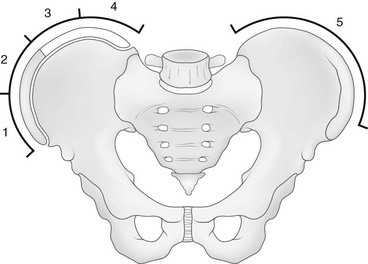
The Risser grade proceeds from grade 0 (no ossification) to grade 4 (all four quadrants show ossification of the iliac apophysis). When the ossified apophysis fuses completely to the ilium (Risser grade 5), the patient is skeletally mature. (From Herring JA, ed. Scoliosis. In: Herring JA, ed. Tachdjian’s pediatric orthopedics. vol 1. 3rd ed. Philadelphia: WB Saunders; 2002:213-321.)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







