Lippman-Cobb method. The latter method, which has been adopted and standardized by the Scoliosis Research Society, classifies the severity of scoliotic curvature into seven groups (Table 33.2).
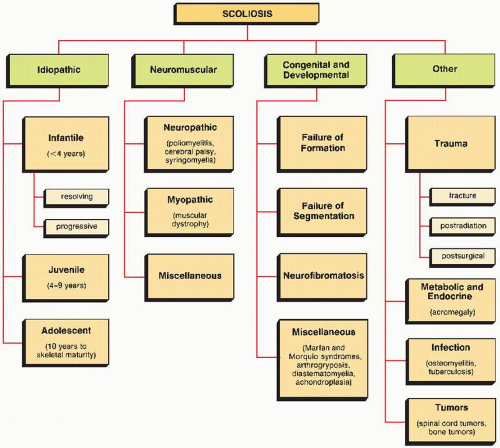 FIGURE 33.1 General classification of scoliosis on the basis of cause. |
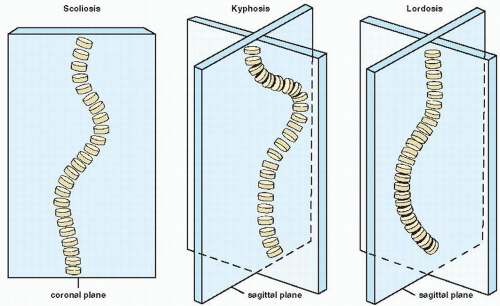 FIGURE 33.2 Definitions. Scoliosis is a lateral curvature of the spine in the coronal (frontal) plane. Kyphosis is a posterior curvature of the spine and lordosis an anterior curvature, both occurring in the sagittal (lateral) plane. |
 FIGURE 33.3 Idiopathic scoliosis. Anteroposterior radiograph of the spine of a 15-year-old girl shows the typical features of idiopathic scoliosis involving the thoracolumbar segment. The convexity of the curve is to the right; a compensatory curve in the lumbar segment has its convexity to the left. |
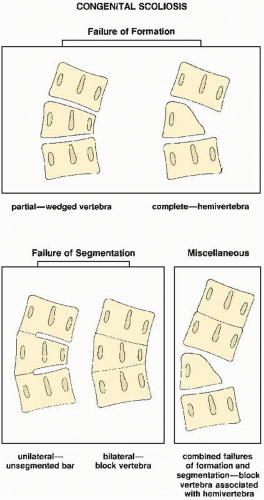 FIGURE 33.4 Classification of congenital scoliosis on the basis of cause. (Modified from MacEwen GD et al., 1968; Winter RB et al., 1968.) |
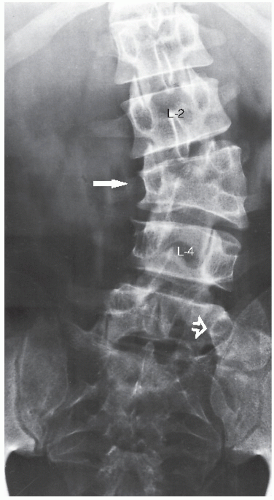 FIGURE 33.5 Congenital scoliosis. Anteroposterior radiograph of the lumbosacral spine of a 22-year-old man demonstrates scoliosis caused by hemivertebra, a complete unilateral failure of formation. Note the deformed L3 vertebra (arrow) secondary to the faulty fusion of the hemivertebra on the left side, where two pedicles are evident. The resulting scoliosis has its convex border to the left. An associated anomaly is also apparent from the presence of the so-called transitional lumbosacral vertebra (open arrow). |
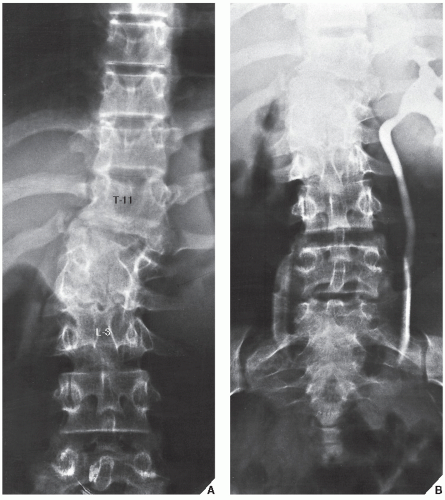 FIGURE 33.6 Congenital scoliosis. (A) Supine anteroposterior radiograph of the thoracolumbar spine of a 13-year-old girl shows congenital scoliosis secondary to block vertebrae consisting of a fusion of T12-L2. (B) IVP demonstrates only the left kidney, an example of renal agenesis. Congenital scoliosis is frequently associated with urinary tract anomalies. |
TABLE 33.1 Standard Radiographic Projections and Radiologic Techniques for Evaluating Scoliosis | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
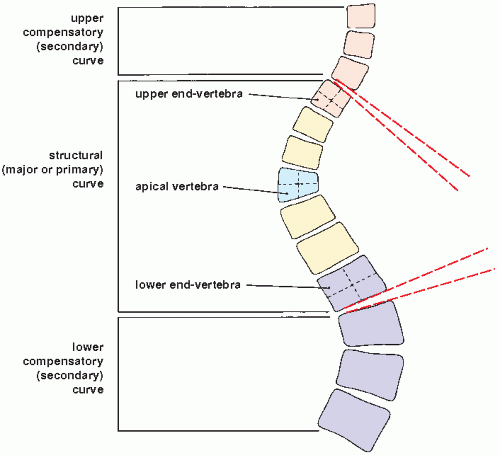 FIGURE 33.7 Terminology used in describing the scoliotic curve. The end vertebrae of the curve are defined as those that tilt maximally into the concavity of the structural curve. The apical vertebra, which shows the most severe rotation and wedging, is the one whose center is most laterally displaced from the central line. The center of the apical vertebra is determined by the intersection of two lines, one drawn from the center of the upper and lower end plates and the other from the center of the lateral margins of the vertebral body. The center should not be determined by diagonal lines through the corners of the vertebral body. |
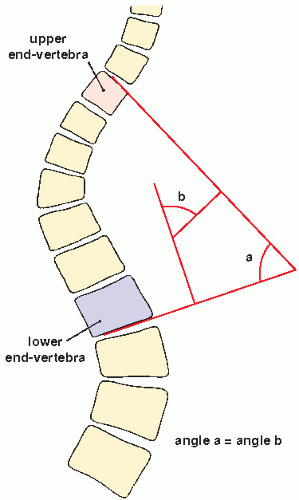 FIGURE 33.8 Lippman-Cobb method. In the Lippman-Cobb method of measuring the degree of scoliotic curvature, two angles are formed by the intersection of two sets of lines. The first set of lines, one drawn tangent to the superior surface of the upper end vertebra and the other tangent to the inferior surface of the lower end vertebra, intersects to form angle (a). The intersection of the other set of lines, each drawn perpendicular to the tangential lines, forms angle (b). These angles are equal, and either may serve as the measurement of the degree of scoliosis. |
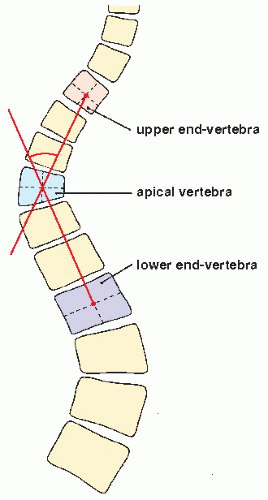 FIGURE 33.9 Risser-Ferguson method. In the Risser-Ferguson method, the degree of scoliotic curvature is determined by the angle formed by the intersection of two lines at the center of the apical vertebra, the first line originating at the center of the upper end vertebra and the other at the center of the lower end vertebra. |
TABLE 33.2 Lippman-Cobb Classification of Scoliotic Curvature | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
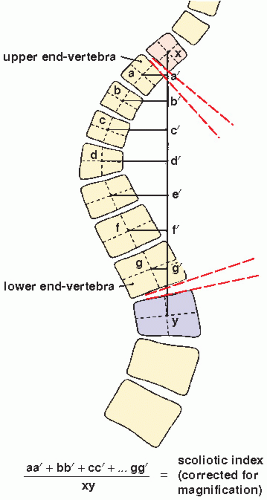 FIGURE 33.10 Scoliotic index. In the measurement of scoliosis using the scoliotic index, each vertebra (a-g) is considered an integral part of the curve. A vertical spinal line (xy) is first determined whose endpoints are the centers of the vertebrae immediately above and below the upper and lower end-vertebrae of the curve. Lines are then drawn from the center of each vertebral body perpendicular to the vertical spinal line (aa′, bb′,… gg′). The values yielded by these lines represent the linear deviation of each vertebra; their sum, divided by the length of the vertical line (xy) to correct for radiographic magnification, yields the scoliotic index. A value of zero denotes a straight spine; the higher the scoliotic index, the more severe the scoliosis. |
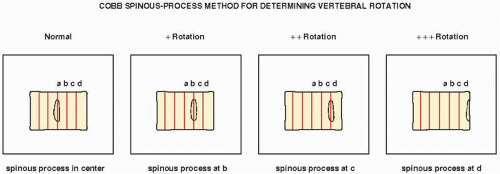 FIGURE 33.11 Cobb spinous-process method. In the Cobb spinous-process method for determining rotation, the vertebra is divided into six equal parts. Normally, the spinous process appears at the center. Its migration to certain points toward the convexity of the curve marks the degree of rotation. |
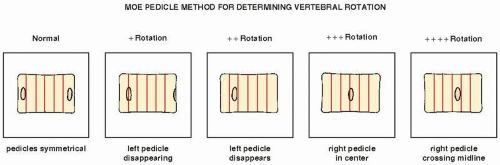 FIGURE 33.12 Moe pedicle method. The Moe pedicle method for determining rotation divides the vertebra into six equal parts. Normally, the pedicles appear in the outer parts. Migration of a pedicle to certain points toward the convexity of the curve determines the degree of rotation. |
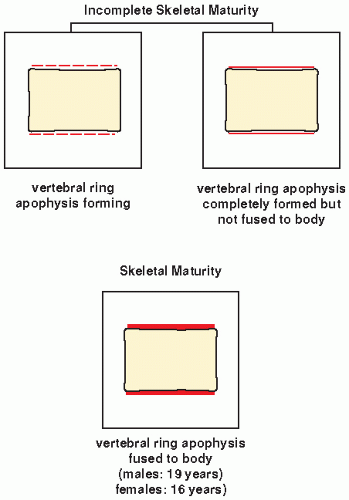 FIGURE 33.13 Skeletal maturity. Determination of skeletal maturity from ossification of the vertebral ring apophysis. |
 FIGURE 33.14 Skeletal maturity. The ossification of the iliac apophysis is helpful in determining skeletal age. Progression of the apophysis in this 14-year-old girl with idiopathic scoliosis has been completed, but the lack of fusion with the iliac crest (arrows) indicates continuing skeletal maturation. |
then fixed to the L-rods. Variations in this technique have been used with L-rod instrumentation alone, which involves the use of sublaminar wires fixed to the rods, or a combination of Harrington distractors and wires fixed to them. Cotrel-Dubousset spinal instrumentation using knurled rods has also gained popularity. Fixation is achieved via pediculotransverse double-hook purchase at several levels. The two knurled rods are additionally stabilized by two transverse traction devices. The Dwyer technique, involving anterior fixation of the spine and obliteration of the intervertebral disks, is also used in the surgical treatment of scoliosis but more often in the paralytic types of the deformity.
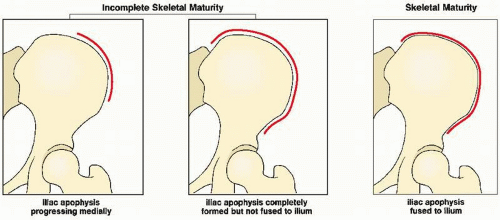 FIGURE 33.15 Skeletal maturity. Determination of skeletal maturity from the status of ossification of the iliac apophysis. |
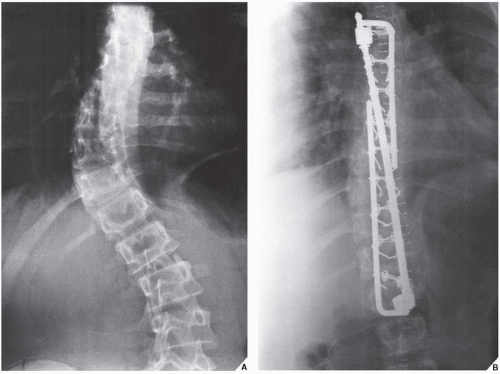 FIGURE 33.16 Treatment of scoliosis. (A) Preoperative anteroposterior radiograph of the lumbar spine in a 15-year-old girl shows idiopathic dextroscoliosis. (B) Postoperative film shows the placement of the Harrington distractor and two Luque rods. Note the multiple sublaminar wires fixed into the prebent L-rods. |
birth or may appear over time, occur in more than 90% of patients. The latter lesions have a smooth border that has been likened to the coast of California; this distinguishes them from the café-au-lait spots seen in fibrous dysplasia, which have rugged “coast of Maine” borders. These spots increase in size and number as the person grows older. Axillary or inguinal freckles are rare at birth, but appear throughout childhood and adolescence. Plexiform neurofibromatosis is a diffuse involvement of the nerves, associated with elephantoid masses of soft tissue (elephantiasis neuromatosa) and localized or generalized enlargement of a part or all of a limb. Patients with these manifestations are particularly prone to malignant tumors (see Fig. 22.35).
TABLE 33.3 Most Effective Radiographic Projections and Radiologic Techniques for Evaluating Common Anomalies with General Affliction of the Skeleton | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
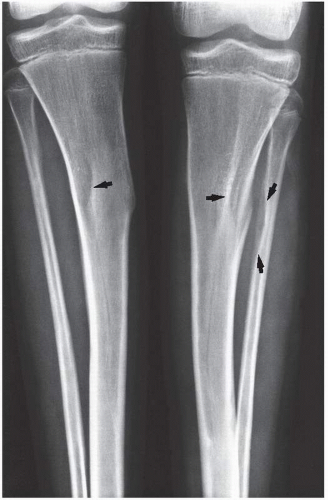 FIGURE 33.17 Neurofibromatosis. Anteroposterior radiograph of the lower legs of an 11-year-old girl shows pit-like erosions in the proximal tibiae and fibulae (arrows), a common finding in this condition. |
vertebral bodies; with the introduction of MRI, this modality became more prevalent in investigation of the aforementioned abnormalities.
 FIGURE 33.18 Neurofibromatosis. Lateral radiograph of the right lower leg of an 11-year-old boy with generalized disease demonstrates anterior bowing of the distal tibia and fibula, associated with pseudoarthrosis. Note the pressure erosions in the middle third of the tibial diaphysis. |
 FIGURE 33.19 Plexiform neurofibromatosis. Lateral radiograph of the lower leg and foot of a 37-year-old woman shows whittling of the calcaneus and marked hypertrophy of the soft tissues (elephantiasis). |
 FIGURE 33.20 Neurofibromatosis. Oblique radiograph of the cervical spine of a 26-year-old man demonstrates widening of the upper neural foramina (arrows) secondary to “dumbbell” neurofibromas arising in the spinal nerve roots. |
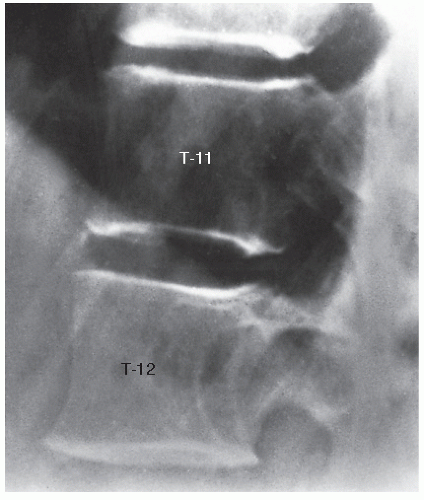 FIGURE 33.21 Neurofibromatosis. Lateral spot-film of the lower thoracic spine in a 29-year-old woman shows scalloping of the posterior border of the T12 vertebra, a common manifestation of this condition. |
birth, but these more often appear later in infancy. This condition is also associated with other manifestations, such as deformities of the extremities, blue sclerae, laxity of ligaments, and dental abnormalities.
Type I | This most common type of the disorder is a relatively mild form, with autosomal-dominant inheritance. Bone fragility is mild to moderate and osteoporosis is invariably present. Sclera are distinctly blue and hearing loss or impairment is a common feature. Stature is normal or near normal. Wormian bones are present. The two subtypes are distinguished by the presence of normal teeth (subtype IA) or dentinogenesis imperfecta (subtype IB). |
Type II | This is the fetal or perinatal lethal form of the disorder. This form demonstrates an autosomal-dominant inheritance with new mutation. The very severe nature of generalized osteoporosis, bone fragility, and severe intrauterine growth retardation results in death in the fetal or early perinatal period. Of those infants who survive, 80% to 90% die by 4 weeks of age. All patients in this group have radiologic features typical of OI. In addition, the sclera are blue and the face has a triangle shape caused by soft craniofacial bones and a beaked nose. The calvarium is large relative to the face, and the skull shows a marked lack of mineralization as well as wormian bones. Limbs are short, broad, and angulated. Three subtypes, A, B, and C, are marked by differences in the appearance of the ribs and the long bones. In subtype A, the long bones are broad and crumpled and the ribs are broad, with continuous beading. In subtype B, the long bones also are broad and crumpled, but the ribs show either discontinuous beading or no beading. Subtype C is characterized by thin fractured long bones and ribs that are thin and beaded. |
Type III | This is a severe progressive form and represents a rare autosomal-dominant inheritance with new mutations. Bone fragility and osteopenia are considerable, leading with age to multiple fractures and severe progressive deformity of the long bones and spine. Bone abnormalities are generally less severe than in type II and more severe than in types I or IV. Sclera are normal, although pale blue or gray at birth, but the color changes through infancy and early childhood until it is normal by adolescence or adulthood. The calvarium is large, thin, and poorly ossified; wormian bones are present. |
Type IV | This is also a rare type of OI and is inherited as an autosomal-dominant trait. Characteristically, osteoporosis, bone fragility, and deformity are present, but they are very mild. Sclera are usually normal. The incidence of hearing impairment is low and is even lower than in type I. |
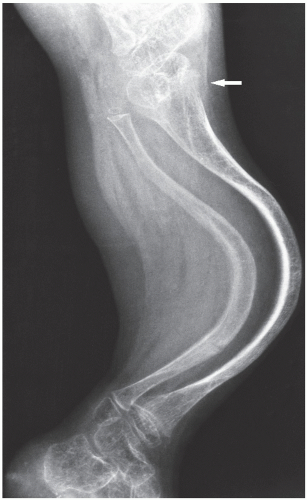 FIGURE 33.22 Osteogenesis imperfecta. Lateral radiograph of the leg of a 12-year-old boy with type III disease demonstrates thinning of the cortices and anterior bowing of the tibia and fibula. Note the trumpet-shaped appearance of the tibial metaphysis (arrow). |
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


