SECTION II CARDIAC IMAGING
Essentials 1
Case
A 35-year-old male patient presents for a cardiac magnetic resonance (CMR) examination and is found to have a left ventricle (LV) end-diastolic volume (EDV) 90 mL/m2, left ventricular ejection fraction 58%, right ventricle (RV) EDV 85 mL/m2, and right ventricular ejection fraction 56%.

Questions
1. Regarding the CMR images shown, which ONE of the following is TRUE? See videos for cines.
* Videos in this chapter can be accessed at MediaCenter.Thieme.com. Please follow the instructions found on the MediaCenter page at the front of this book.
A. Cine images of this nature to evaluate morphology and function require contrast administration.
B. Imaging was performed using a spin echo technique.
C. The RV and LV are dilated.
D. A two-chamber imaging plane is shown in A, and three-chamber and left ventricular outflow tract imaging planes are shown in B.
E. Quantification of LV and RV size and function is performed using the images in A.
2. Which ONE of the following is NOT an advantage of cardiac CMR?
A. Higher spatial and contrast resolution compared to echocardiography
B. Imaging is not affected by patient body habitus.
C. It is the test of choice for detection of diastolic dysfunction.
D. Allows accurate noninvasive quantification of large vessel flow
E. Provides superior evaluation of biventricular size and systolic function compared to echocardiography
3. Which ONE of the following is NOT a contraindication for CMR?
A. Implantable cardioverter defibrillator (ICD)
B. Pacemaker
C. Cochlear implant
D. Coronary stent
E. Intracranial shrapnel
Answers and Explanations
Question 1
E. Correct! Ventricular volumes and function are calculated from sequential short axis cine images covering the entire ventricle by contour tracing.
Other choices and discussion
A. Cine CMR is performed using a gradient echo sequence (GRE), which provides a “bright blood effect” without the need for intravenous contrast. Cine CMR uses a special form of GRE imaging called steady state free precession (SSFP), a family of sequences that are currently the backbone of cine CMR imaging. Members of the SSFP family include balanced fast field echo, fast imaging employing steady-state acquisition, and true fast imaging with SSFP. SSFP produces bright blood images with excellent contrast between myocardium and blood within the heart (blood pool).
B. Spin echo imaging produces static black blood images that are used for evaluation of cardiac anatomy and morphology.
C. The LV and RV volumes are within normal limits. Normal limits for LV EDV in a 35-year-old male are 53 to 97 mL/m2 and 67 to 111 mL/m2 for RV EDV.
D. A short-axis view of the heart is shown in A, and four- and two-chamber views of the heart are shown in B.
Question 2
C. Correct! Echocardiography is the test of choice for detection of diastolic dysfunction due to its higher temporal resolution and real-time nature as compared to cardiac CMR.
Other choices and discussion
A. Image quality of CMR is superior to echocardiography with notably higher spatial resolution and contrast resolution.
B. Unlike echocardiography, a large body habitus is not a disadvantage for cardiac CMR.
D. CMR, using the phase contrast technique, allows accurate noninvasive determination of flow in large vessels.
E. CMR measures of ventricular size and function do not depend on geometric assumptions, are unaffected by body habitus, and are accurate and reproducible. CMR is the reference standard for biventricular size and systolic function.
Question 3
D. Correct! CMR can be safely performed with coronary stents. Most coronary stents are non-ferromagnetic and labeled as “magnetic resonance (MR) safe.” The remainder have been labeled as “MR conditional.”
Other choices and discussion
A. ICD is a relative contraindication to CMR. Potential hazards include device dislodgement, programming changes, asynchronous pacing, activation of anti-tachycardiac therapies, inhibition of pacing output, and induced lead currents. An increasing number of patients have an implanted “MR-conditional” device, allowing them to safely undergo MR scanning (provided the manufacturer’s guidance is adhered to). In addition, some patients with non-MR-conditional devices may undergo MR scanning if no other imaging modality is deemed suitable and there is a clear clinical indication for scanning that outweighs the potential risk.
B. A pacemaker is a relative contraindication to CMR. Potential hazards are similar to ICDs. MR imaging may be performed under specific circumstances in nonconditional devices if benefits outweigh the risks. MR-conditional pacemakers are now available.
C. Cochlear implants are electronically activated devices. Consequently, an MR procedure may be contraindicated for a patient with this type of implant because of the possibility of injuring the patient and/or altering or damaging the function of the device. Recently, some cochlear implants have received approval designating them as “MR conditional.”
E. Intracranial shrapnel is a contraindication to CMR.
Suggested Reading
Herzog B, Greenwood J, Plein S. Cardiovascular Magnetic Resonance Pocket Guide. Version 1.2. Updated 2016. http://www.cmr-guide.comTop Tips
Cine CMR is performed using a special form of GRE imaging called SSFP imaging.
CMR is the reference standard for LV and RV size and systolic function, which are calculated by planimetry of a series of short axis slices.
Major indications for CMR in clinical practice include evaluation of myocardial viability in ischemic heart disease, assessment of cardiomyopathies, comprehensive evaluation of adult congenital heart disease, and identification and characterization of cardiac masses including thrombi.
Essentials 2
Case
A 50-year-old man presents with chest pain.

Questions
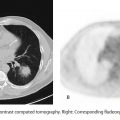
1. What is the abnormality present on the coronary computed tomography angiography (CCTA) images shown?
A. Minimal (< 25%) non-flow-limiting disease in the left anterior descending coronary artery
B. Mild (25 to 49%) non-flow-limiting disease in the left anterior descending coronary artery
C. Moderate (50 to 69%) possible flow-limiting disease in the left anterior descending coronary artery
D. Left anterior descending coronary artery occlusion
E. Moderate (50 to 69%) possible flow-limiting disease in the left circumflex artery
2. Mark the FALSE statement regarding the benefits and applications of CCTA.
A. Coronary artery calcium (CAC) scoring may be used for risk stratification and reclassification in asymptomatic patients with intermediate probability of coronary artery disease (CAD).
B. The use of CCTA is appropriate for detection of obstructive CAD in symptomatic patients when functional stress testing cannot be performed or is nondiagnostic.
C. The use of CCTA in the emergency department in patients with chest pain and negative cardiac enzymes allows safe discharge, reduces length of stay, and is cost saving.
D. The use of CCTA is appropriate for preoperative evaluation in patients undergoing heart surgery for noncoronary indications when the risk of CAD is low to intermediate.
E. A major advantage of CCTA is its high positive predictive value for detection of obstructive CAD.
3. Which of the following methods is NOT a radiation dose-lowering method in CCTA?
A. Lowering the heart rate with beta blockers
B. Use of prospective ECG triggering
C. 100 kvp tube potential
D. Use of an iterative reconstruction method
E. Use of a high spatial frequency reconstruction filter
Answers and Explanations
Question 1
C. Correct! The CCTA images show moderate (50 to 69%) possible flow-limiting disease in the LAD. The LAD arises from the left main coronary artery and travels in the anterior interventricular groove, giving rise to diagonal branches and septal perforators. The left circumflex artery arises from the left main coronary artery and travels posteriorly into the left atrioventricular groove. CCTA quantification of lesion severity in clinical practice is visually evaluated and reported in terms of percent maximal diameter stenosis using the stenosis grading scheme below:
0—Normal: absence of plaque and no luminal stenosis
1—Minimal: plaque with < 25% stenosis
2—Mild: 25 to 49% stenosis
3—Moderate: 50 to 69% stenosis
4—Severe: 70 to 99% stenosis
5—Occluded
Question 2
E. Correct! CCTA is an excellent test to rule out CAD in selected low- to intermediate-risk patients due to its high negative predictive value for exclusion of obstructive CAD (90–99%). The positive predictive value of CCTA for obstructive CAD is moderate, and it should be a rule-out test rather than a rule-in test for obstructive CAD.
Other choices and discussion
A. CAC scoring is most useful for risk stratification of asymptomatic patients with an intermediate Framingham risk of future cardiovascular events (10 to 20%, 10-year risk), in whom a high-risk CAC score may prompt an increase in aggressive medical therapy.
B. The use of CCTA is appropriate and guideline-supported for detection of obstructive CAD in symptomatic patients with intermediate probability of CAD when functional stress testing such as stress electrocardiogram (ECG), myocardial perfusion scintigraphy, or dobutamine stress echo cannot be performed or is nondiagnostic.
C. Multiple studies have shown that the use of CCTA in the emergency department in patients with chest pain and negative cardiac enzymes allows safe discharge, reduces length of stay, and is a cost-saving measure compared to the usual standard of care, including functional testing for detection of CAD.
D. As part of the preoperative evaluation, CCTA is viewed as a potential option among patients undergoing heart surgery for noncoronary indications (e.g., valve replacement surgery or atrial septal defect closure) when the pretest CAD risk is intermediate.
Question 3
E. Correct! A high spatial resolution reconstruction filter can be used to decrease blooming artifact from stents and calcium in CCTA and DOES NOT lead to a reduction in radiation dose.
Other choices and discussion
A. Vigorous heart rate-lowering (≤ 60 bpm) with beta blockers will allow the use of prospective ECG triggering, which leads to substantial radiation dose reduction (~40 to 50%) as compared to retrospective ECG gating needed at higher heart rates.
B. Prospective ECG-gated CCTA acquisition mode refers to an acquisition triggered by the ECG signal. The table moves periodically in “steps,” and the X-ray tube is on intermittent (“shoot”)—the so-called step-and-shoot mode. The user selects the phase in which to acquire the images (usually diastole). The major advantage of this technique is substantial radiation dose reduction, as the X-ray tube is on for only 20 to 25% of the cardiac cycle in diastole and is completely off for the majority of the remaining cardiac cycle.
C. A relatively small change in peak voltage of 20 kVp (from 120 to 100 kVp) results in a decrease in radiation dose of 30 to 40%. Multiple studies support 100-kV imaging for patients weighing up to 90 kg or with a body mass index of up to 30 kg/m2.
D. Iterative reconstruction methods can reduce the impact of X-ray quantum noise on computed tomography images and allow a lower radiation dose while preserving clinical diagnostic utility.
Suggested Readings
Litmanovich DE, Tack DM, Shahrzad M, et al. Dose reduction in cardiothoracic CT: review of currently available methods. RadioGraphics 2014;34:1469–1489 Taylor AJ, Cerqueira M, Hodgson J, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. J Cardiovasc Comput Tomogr 2010;4:e1–407.e33Top Tips
CCTA is appropriate for detection of obstructive CAD in low- to intermediate-risk symptomatic patients.
The negative predictive value of CCTA for obstructive CAD is high (~90 to 99%).
With proper attention to technique, including lowering of heart rate with beta blockers, prospective ECG triggering, optimization of imaging parameters (including kVp and scan range), and use of modern computed tomography scanners, the radiation dose of CCTA is low (in the range of 1 to 3 mSv with sub-mSv doses possible in select cases).
Essentials 3
Case
A 25-year-old male patient presents with chest pain. Physical examination is remarkable for ectopia lentis.

Questions
1. The CORRECT diagnosis is:
A. Marfan syndrome
B. Bicuspid aortic valve disease
C. Loeys-Deitz syndrome
D. Turner syndrome
E. Noonan syndrome
2. Which of the following statements is FALSE regarding prophylactic surgical repair of thoracic aortic aneurysms?
A. Surgical repair in Marfan syndrome is recommended when the aorta reaches 5.0 cm (unless there is a family history of aortic dissection), a rapidly expanding aneurysm, or the presence of significant aortic valve regurgitation.
B. In Loeys-Dietz syndrome, surgical repair is recommended at an aortic diameter of 4.4 to 4.6 cm by computed tomography and/or magnetic resonance imaging.
C. Surgical treatment of asymptomatic patients with degenerative ascending aortic aneurysms should be considered when the diameter ≥ 5.5 cm.
D. Patients undergoing aortic valve repair or replacement and who have an ascending aorta or aortic root > 4.5 cm should be considered for concomitant repair of the aortic root or replacement of the ascending aorta.
E. Operative intervention to repair the aortic sinuses or replace the ascending aorta is indicated in patients with a bicuspid aortic valve if the diameter of the aortic sinuses or ascending aorta is ≥ 4.5 cm.
3. All of the following genetic conditions are associated with thoracic aortic aneurysms and/or dissection EXCEPT:
A. Loeys-Dietz syndrome
B. Autosomal dominant polycystic kidney disease
C. Bicuspid aortic valve
D. Ehlers-Danlos syndrome
E. Williams syndrome
* Videos in this chapter can be accessed at MediaCenter.Thieme.com. Please follow the instructions found on the MediaCenter page at the front of this book.
Answers and Explanations
Question 1
A. Correct! Marfan syndrome is an inheritable disorder of the connective tissue with a prevalence of 1 in 3000 to 5000 individuals. The condition is inherited in an autosomal dominant manner and results from mutations in the FBN1 gene. The ocular manifestation that is both sensitive and fairly specific for Marfan syndrome is ectopia lentis (lens displacement). The most common cardiovascular complication is progressive aortic root enlargement initially occurring at the sinuses of Valsalva and leading to effacement of the sinotubular junction. Note the dilatation of the aortic root at the sinuses (annulo-aortic ectasia), effacement of the sinotubular junction, mitral valve prolapse, and regurgitation in this case.
Other choices and discussion
B. The aortic valve is tricuspid in this case as shown on the short axis enface view. The most common pattern of aortic dilatation in bicuspid aortic valves is a tubular dilatation of the ascending aorta followed by dilatation of the sinuses of Valsalva.
C. Loeys-Deitz syndrome is characterized by the triad of arterial tortuosity and aneurysms, hypertelorism, and bifid uvula or cleft palate (or a uvula with a wide base or prominent ridge on it). Although Loeys-Deitz syndrome and Marfan syndrome have some overlapping features, the presence of ectopia lentis is distinct for Marfan syndrome.
D. Cardiovascular manifestations of Turner syndrome include aortic dilatation, bicuspid aortic valves, aortic coarctation, and aortic dissection.
E. The most common cardiovascular lesions in Noonan syndrome are pulmonic valve stenosis and hypertrophic cardiomyopathy.
Question 2
E. Correct! This statement is FALSE. Operative intervention to repair the aortic sinuses or replace the ascending aorta is indicated in patients with a bicuspid aortic valve if the diameter of the aortic sinuses or ascending aorta is > 5.5 cm. Replacement of the ascending aorta is reasonable in patients with a bicuspid aortic valve if the diameter of the ascending aorta is > 4.5 cm only if they are undergoing aortic valve surgery because of severe AS or AR.
Other choices and discussion
A. Surgical repair is recommended in Marfan syndrome when the diameter of the aortic root or other parts of the thoracic aorta is 5.0 cm or more.
B. There is a higher risk of dissection in patients with Loeys-Dietz syndrome, and hence, thresholds for surgical replacement are lower: > 4.2 cm by time of flight and 4.4 to 4.6 cm by computed tomography or magnetic resonance imaging.
C. Surgical or endovascular treatment of degenerative ascending aortic aneurysms in the absence of genetic syndromes and valve disease is recommended when the diameter exceeds 5.5 cm or when the growth rate exceeds 0.5 cm/year.
D. Patients undergoing aortic valve repair or replacement and who have an ascending aorta or aortic root > 4.5 cm should be considered for concomitant repair of the aortic root or replacement of the ascending aorta.
Question 3
E. Correct! Williams syndrome is a congenital, multisystem disorder involving the cardiovascular, connective tissue, and central nervous systems. Supravalvular aortic stenosis, either in the form of an hourglass discrete narrowing at the sinotubular junction or long segment stenosis of the thoracic aorta, is the most common cardiovascular lesion followed by pulmonary arterial stenosis.
Other choices and discussion
A. Loeys-Dietz syndrome is an autosomal dominant aortic aneurysm syndrome with involvement of many other systems. The vascular disease in these patients is particularly aggressive, and most patients have aortic root aneurysms (98%) that lead to aortic dissection.
B. There is an association of arterial dissections, including thoracic aortic dissections, in patients with autosomal dominant polycystic kidney disease.
C. Aortic aneurysms are found in 20% of patients undergoing surgery for a bicuspid aortic valve, and 15% of patients with acute aortic dissection have bicuspid valves.
D. Most of the fatal complications in the Ehlers-Danlos syndrome are caused by arterial rupture with most deaths attributable to arterial dissections or ruptures involving primarily the thoracic or abdominal arteries.
Top Tips
Marfan syndrome is an inherited (autosomal dominant) connective tissue disorder with the most common cardiovascular complication being progressive aortic root enlargement initially occurring at the sinuses of Valsalva and leading to effacement of the sinotubular junction (annulo-aortic ectasia).
Surgical repair is recommended when the diameter of the aortic root or other parts of the thoracic aorta is 5.0 cm. A lower diameter of 4.5 to 5 cm is considered for surgical repair in the presence of a family history of aortic dissection, rapid diameter change (> 0.5 cm/year), significant valvular regurgitation, or a desire for pregnancy.
Surgical treatment of degenerative ascending aortic aneurysms in the absence of genetic syndromes and valve disease is recommended when the diameter exceeds 5.5 cm or when the growth rate exceeds 0.5 cm/year.
Essentials 4
Case
A 55-year-old man is admitted with acute chest pain.

Questions
1. Based on the provided cardiac magnetic resonance (CMR) images, which ONE of the following statements is CORRECT?
A. The patient has had a myocardial infarction in the right coronary artery distribution and will likely improve function by revascularization.
B. The patient has had a myocardial infarction in the left anterior descending coronary artery distribution and is best managed medically.
C. The patient has had a myocardial infarction in the left circumflex artery distribution and is best managed medically.
D. Images indicate acute myocarditis, and treatment should be supportive.
E. If the measured left ventricular ejection fraction (LVEF) is 30%, implantable cardioverter defibrillator placement is recommended before discharge from the hospital.
2. Which of the following sequences is used for viability imaging in routine clinical practice?
A. T1-weighted postcontrast turbo spin echo
B. T2-weighted noncontrast turbo spin echo
C. T1-weighted postcontrast inversion recovery gradient echo
D. T1 mapping precontrast
E. Steady state free precession noncontrast cine
3. Which of the following statements is FALSE regarding the applications of CMR in ischemic heart disease (IHD)?
A. Late gadolinium enhancement (LGE) has a higher spatial resolution and accuracy than cardiac single-photon emission computed tomography (SPECT) for detection of MI and viability.
B. CMR myocardial stress perfusion imaging has a higher sensitivity and specificity than cardiac SPECT for detection of obstructive coronary artery disease.
C. CMR is appropriate for evaluation of ventricular size and function in IHD when echo windows are unsatisfactory.
D. CMR is the test of choice for direct anatomical evaluation of coronary stenosis.
E. The identification of microvascular obstruction on CMR is an adverse prognostic finding in IHD.
* Videos in this chapter can be accessed at MediaCenter.Thieme.com. Please follow the instructions found on the MediaCenter page at the front of this book.
Answers and Explanations
Question 1
B. Correct! The left anterior descending coronary artery (LAD) supplies the anterior wall, anterior septum, and anterior lateral wall of the left ventricle. The delayed enhancement (right image) is in the LAD territory affecting the subendocardium and is nearly transmural (> 75% thickness of myocardium enhanced). The transmural extent of delayed enhancement is a marker of myocardial viability. Myocardium with > 50% enhancement is considered nonviable and unlikely to improve function following revascularization. Such patients are best managed medically.
Other choices and discussion
A. The right coronary artery supplies the inferior septum and inferior wall of the left ventricle.
C. The left circumflex artery supplies the inferior lateral wall of the left ventricle.
D. Myocarditis causes subepicardial or mid-wall enhancement in a noncoronary distribution.
E. In patients with ischemic heart disease, an implantable cardioverter defibrillator should be considered if indications (LVEF ≤ 35%, New York Heart Association II/III, or LVEF ≤ 30%, New York Heart Association I or asymptomatic) exist at least 40 days after MI. A possible exception to this rule is in post-MI patients (> 48 hours) who develop sustained ventricular tachycardia/ventricular fibrillation not due to transient or reversible causes.
Question 2
C. Correct! Viability imaging uses a segmented (imaging performed over multiple heart beats) T1-weighted inversion recovery (180-degree inversion pulse to increase conspicuity between normal and contrast-enhanced abnormal myocardium) fast gradient echo sequence 10 to 15 minutes post gadolinium administration.
Other choices and discussion
A. T1-weighted postcontrast turbo spin echo imaging may be used for tissue characterization such as in the evaluation of cardiac masses. However, it does not provide adequate contrast resolution to accurately detect MI.
B. T2-weighted noncontrast spin echo imaging may be used for detection of myocardial edema and inflammation. However, it is does not provide adequate contrast for detection of MI and viability.
D. T1 mapping of the myocardium is a novel and expanding application of CMR imaging and has the potential to depict diffuse interstitial fibrosis in a variety of cardiac diseases. Precontrast T1 mapping can detect MI without intravenous contrast. However, further validation of the technique is required, and it is not a routine clinical application at this time.
E. Steady state free precession noncontrast cine imaging is used for evaluation of cardiac anatomy and function.
Question 3
D. Correct! This statement is FALSE. CMR for direct anatomic evaluation of coronary stenosis is limited by spatial resolution and long imaging times. Computed tomography and direct catheter angiography are the preferred modalities for direct visualization of coronary stenosis.
Other choices and discussion
A. The in-plane spatial resolution of LGE CMR is in the range of 1.4 × 1.8 mm and allows detection of MI including small subendocardial infarctions with higher accuracy than SPECT.
B. Myocardial vasodilator stress perfusion magnetic resonance imaging allows detection of obstructive coronary artery disease with higher accuracy than SPECT due to superior image quality independent of body habitus and higher spatial resolution.
C. The use of CMR is considered appropriate for evaluation of ventricular function in IHD when echo windows are unsatisfactory, such as due to obesity.
E. Microvascular obstruction in acute MI identified as low-signal intensity regions with hyperenhancing myocardium is an indicator of adverse prognosis including negative remodeling and arrhythmias.
Suggested Reading
Hundley WG, Bluemke DA, Finn JP, et al. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation task force on expert consensus documents. J Am Coll Cardiol 2010;55:2614–2662Top Tips
Late gadolinium imaging is appropriate for determining the extent of myocardial necrosis and viability in ischemic heart disease.
LGE in a coronary artery distribution involving the subendocardium is indicative of MI.
The transmural extent of LGE is a marker of myocardial viability: subendocardial to < 25% enhancement = viable; 25 to 50% = mixed and likely viable; 50 to 75% = mixed and likely nonviable; > 75% enhancement = nonviable.
Essentials 5
Case
A 54-year-old man has increasing shortness of breath for which a cardiac magnetic resonance (CMR) examination was performed.

Questions
1. In conjunction with the provided images, the CORRECT diagnosis is:
A. Double outlet right ventricle
B. D-Transposition of the great arteries
C. Isolated pulmonary valve stenosis
D. Truncus arteriosus
E. Tetralogy of Fallot
2. Following primary anatomic repair of the condition presented, the most common/major hemodynamic complication is which of the following?
A. Residual pulmonic stenosis
B. Tricuspid insufficiency
C. Residual VSD
D. Pulmonary regurgitation
E. Aortic root dilatation
3. Pulmonic valve replacement (PVR) in repaired tetralogy of Fallot is generally performed when the magnetic resonance–measured RV end-diastolic volume (EDV) reaches which of the following values?
A. 90 to 110 mL/m2
B. 110 to 130 mL/m2
C. 150 to 170 mL/m2
D. 170 to 200 mL/m2
E. 200 to 250 mL/m2
* Videos in this chapter can be accessed at MediaCenter.Thieme.com. Please follow the instructions found on the MediaCenter page at the front of this book.
Answers and Explanations
Question 1
E. Correct! TOF is characterized by ventricular septal defect (VSD), overriding aorta, right ventricular outflow tract (RVOT) obstruction, and right ventricular hypertrophy (RVH). Note the aorta overriding the right ventricle (RV) and the subaortic VSD in A. In the RVOT view (B), a dephasing jet from subpulmonic stenosis in systole is shown along with RVH (and incidental note of a left superior vena cava draining to the coronary sinus).
Other choices and discussion
A. Double outlet RV is a type of abnormal ventriculo-arterial connection where both the aorta (> 50% of circumference) and the pulmonary artery arise entirely or predominantly from the RV.
B. In D-transposition of the great arteries, the aorta arises entirely from the RV and the pulmonary artery from the left ventricle. There is atrioventricular concordance and ventriculo-arterial discordance.
C. Isolated pulmonary valve stenosis can be due to a dome-shaped valve with commissural fusion or a dysplastic valve. There are other associated anomalies in this case.
D. Truncus arteriosus consists of a single arterial trunk giving origin to the pulmonary arteries, the coronary arteries, and the aorta.
Question 2
D. Correct! Pulmonic regurgitation is the most common/major complication following anatomic repair. Complete anatomic repair of TOF consists of closure of the VSD and relief of RVOT obstruction by resection of obstructing muscle bundles and pulmonary valvotomy (with or without an annular or RVOT patch). Relief of RVOT obstruction in TOF often involves disruption of pulmonary valve integrity, which leads to PR in the majority of patients. Without intervention, PR results in RV dilation and may lead to a cascade of other complications, including biventricular dysfunction, tachyarrhythmias, exercise intolerance, heart failure, and death.
Other choices and discussion
A. Residual pulmonic stenosis may exist at the subvalvular, valvular, or supravalvular level in repaired TOF. However, it is not the most common residual defect.
B. Tricuspid insufficiency is usually secondary to annular dilatation from RV dilatation and PR. While it has been associated with supraventricular arrhythmias, it is not the most common hemodynamic abnormality.
C. Residual VSD may be present in repaired TOF leading to a left-to-right shunt. However, it is not the most common or major hemodynamic lesion.
E. Aortic root dilation is seen in approximately 15% of adults late after repair and relates to both intrinsic abnormalities of the aorta (cystic medial necrosis) and increased flow (i.e., patients with pulmonary atresia). It may lead to aortic regurgitation, and rarely, to aortic dissection.
Question 3
C. Correct! PVR in survivors of primary TOF repair with PVR improves symptoms, the New York Heart Association class, and can lead to reduction and normalization of RV volumes when properly timed. Normalization of RV dimensions have been documented when preoperative CMR-measured RV EDVs are in the range of 150 170 mL/m2, and this number is usually used as a guide in conjunction with patient symptoms, electrocardiogram, and exercise testing when deciding on PVR.
Other choices and discussion
A. The upper limits of normal for RV size is 90 to 110 mL/m2, and PVR is not performed at this value. Annual echocardiography and CMR at three-year intervals is generally performed for surveillance.
B. An RV EDV in the 110 to 130 mL/m2 range indicates a mildly dilated RV. In the absence of other significant lesions and symptoms, CMR should be repeated in three years in a stable patient.
D and E. An RV EDV > 170 mL/m2 indicates a severely dilated RV that may not normalize in volume after PVR. PVR is recommended before the RV dilates to this value.
Suggested Reading
Bhatt AB, Foster E, Kuehl K, et al. Congenital heart disease in the older adult. A scientific statement from the American Heart Association. Circulation 2015;131:1884–1931Top Tips
TOF: VSD, overriding aorta, right ventricular outflow obstruction, RVH
Anatomic repair of TOF consists of VSD patch repair and relief of RVOT obstruction. The primary hemodynamic defect/complication in adult survivors after repair is residual PVR.
CMR is used to guide the timing of PVR, which is performed before the RV is severely dilated to a value of > 150 mL/m2 for EDV, as larger RVs may not return to a normal size following PVR.
Essentials 6
Case
A 45-year-old woman presents with syncope.

Questions
1. The CORRECT diagnosis is:
A. Hypertrophic cardiomyopathy
B. Hypertensive cardiomyopathy
C. Athlete’s heart
D. Cardiac amyloidosis
E. Fabry disease
2. The following are advantages of cardiac magnetic resonance (CMR) in the evaluation of the diagnosis in the case EXCEPT:
A. Accurate measurement of wall thickness and LV mass
B. Accurate evaluation of the LV apex and basal segments
C. Detection of myocardial fibrosis
D. Differentiation of HCM from phenocopies
E. Measurement of outflow tract gradients
3. Which ONE of the following is NOT a major risk factor for sudden cardiac death (SCD) in HCM?
A. Wall thickness > 30 mm
B. Family history of SCD
C. Sustained VT/resuscitated VF
D. Unexplained syncope
E. Atrial fibrillation
* Videos in this chapter can be accessed at MediaCenter.Thieme.com. Please follow the instructions found on the MediaCenter page at the front of this book.
Answers and Explanations
Question 1
A. Correct! There is asymmetric septal hypertrophy, which represents the most common form of hypertrophic cardiomyopathy (HCM). Patchy mid-wall enhancement is seen in the septum at the junction points of the right ventricle and left ventricle (LV) and is a typical enhancement pattern in HCM.
Other choices and discussion
B. Hypertensive cardiomyopathy may lead to cardiac hypertrophy, which is usually concentric and rarely asymmetric with greater involvement of the septum. Usually the hypertrophy does not exceed 15 mm.
C. Athlete’s heart may lead to concentric hypertrophy that usually does not exceed 13 mm and may be accompanied by LV dilatation. Delayed enhancement is negative.
D. Cardiac amyloidosis manifests as concentric LV hypertrophy with diffuse global subendocardial myocardial enhancement.
E. Fabry disease may present with concentric hypertrophy or asymmetric hypertrophy and is characteristically associated with mid-wall enhancement in the inferior lateral wall of the LV.
Question 2
E. Correct! Magnetic resonance imaging does not accurately determine left ventricular outflow tract gradients in obstructive HCM, due to its lower temporal resolution and lack of real-time data compared with echocardiography.
Other choices and discussion
A. This is an advantage. Compared with echocardiography, CMR allows more accurate estimation of wall thickness and LV mass.
B. Evaluation of the LV apex and basal segments (particularly the basal anterior wall) may challenging with echocardiography, but is straightforward with CMR.
C. Using the late gadolinium enhancement (LGE) technique with magnetic resonance imaging can detect myocardial fibrosis.
D. Phenocopies (including hypertensive cardiomyopathy, infiltrative pathology, storage diseases, and athlete’s heart) can be differentiated from HCM by magnetic resonance imaging, using a combination of morphologic features and tissue characterization by LGE.
Question 3
E. Correct! Atrial fibrillation may be a finding in HCM. However, it is NOT considered a major risk factor for SCD. The fifth major risk factor for SCD in HCM, in addition to those mentioned above, is a hypotensive response to exercise.
Other choices and discussion
A. This is a risk factor. Massive hypertrophy defined as wall thickness > 30 mm is a major risk factor for SCD in HCM.
B. A family history of SCD, known or presumed to be due to HCM, is a major risk factor.
C. Sustained VT or resuscitated VF is a risk factor for SCD in HCM.
D. Unexplained syncope, presumed to be due to nonneurohumoral causes, is a major risk factor for SCD.
Suggested Reading
Baxi AJ, Restrepo CS, Vargas D, et al. Hypertrophic cardiomyopathy from A to Z: genetics, pathophysiology, imaging, and management. Radiographics 2016;36(2):335–354Top Tips
HCM is characterized by thickening of the LV wall involving one or more segments ≥ 15 mm in the absence of LV loading conditions or other causes of hypertrophy.
The asymmetric septal form is the most common phenotype of HCM.
LGE CMR detects fibrosis in HCM and is useful for risk stratification for SCD. HCM is the most common cause of SCD in young people. Major risk factors for SCD in HCM include family history of SCD, syncope, massive wall thickness > 30 mm, nonsustained ventricular tachycardia, and an abnormal hypotensive response to exercise. Implantable cardioverter defibrillator placement by current guideline is recommended when one or more major risk factors are present. LGE on CMR, which appears to reflect fibrosis, is being proposed as a possible risk factor for SCD in HCM. LGE has shown to be predictive of arrhythmias, SCD, and heart failure in HCM. Extensive LGE may be used as an arbitrator for implantable cardioverter defibrillator placement in HCM when risk stratification by conventional methods using the major risk factors is unclear.
Essentials 7
Case
A 30-year-old man with acute chest pain presents for cardiac magnetic resonance (CMR).

Questions
1. The CORRECT diagnosis is:
A. Acute myocardial infarction
B. Acute myocarditis
C. Hypertrophic cardiomyopathy
D. Stress cardiomyopathy
E. Idiopathic dilated cardiomyopathy
2. The MOST COMMON etiology in patients presenting with chest pain, elevated troponin, and normal coronary arteries is which of the following?
A. Acute myocardial infarction
B. Acute myocarditis
C. Hypertrophic cardiomyopathy
D. Stress cardiomyopathy
E. Kawasaki disease
3. Linear mid-wall enhancement in the septum is a feature of which of the following conditions?
A. Idiopathic dilated cardiomyopathy
B. Hypertrophic cardiomyopathy
C. Ischemic cardiomyopathy
D. Cardiac amyloidosis
E. Eosinophilic myocarditis
Answers and Explanations
Question 1
B. Correct! There is subepicardial enhancement in the lateral wall. There is corresponding mild hypokinesis in this segment in the midventricular level (see cine images). These are features of acute myocarditis.
Other choices and discussion
A. Myocardial infarction is characterized by enhancement in a coronary artery distribution involving the subendocardium.
C. HCM is characterized by hypertrophy involving one or more segment > 15 mm. Late gadolinium enhancement typically shows enhancement in a patchy mid-wall distribution at the junction points of the right ventricle and left ventricle (LV) and elsewhere in a thickened myocardium.
D. Stress cardiomyopathy is characterized by apical wall motion abnormality, myocardial edema, and no delayed enhancement.
E. Idiopathic DCM shows LV dilatation and reduced global wall motion. The majority of patients do not show delayed enhancement.
Question 2
B. Correct! Acute myocarditis is usually due to a viral infection of the myocardium with normal coronary arteries. Several studies have shown that the most common underlying etiology of patients presenting with suspected acute coronary syndrome and unobstructed coronary arteries is myocarditis.
Other choices and discussion
A. AMI is usually due to rupture of an unstable plaque in the presence of preexisting coronary artery disease. A total of 7 to 10% of patients presenting with ST-elevation myocardial infarction and 10 to 15% of patients presenting with non-ST-elevation myocardial infarction have unobstructed coronary artery disease on urgent angiography. AMI with unobstructed coronary arteries is the second most common etiology in this cohort of patients. Several different pathophysiologic mechanisms have been proposed to explain this phenomenon (e.g., rupture or erosion of a vulnerable plaque causing transitory occlusion that resolves spontaneously without leaving any residual visible intracoronary lesion) and distal vessel or small-caliber sidebranch disease. Other mechanisms include distal embolization, coronary vasospasm, and inflammation.
C. HCM may present with acute chest pain, elevated troponins, and normal large epicardial coronary arteries, due to a mismatch between oxygen demands of the hypertrophied myocardium and blood supply in the presence of small vessel disease. However, this is a rare presentation of the disease and an uncommon diagnosis in this cohort of patients.
D. Stress cardiomyopathy is the third most common cause of chest pain, elevated troponins, and normal coronary arteries. It is characterized by reversible wall motion abnormalities involving the LV apex in the presence of unobstructed large epicardial coronary arteries.
E. Chest pain in Kawasaki disease is due to coronary aneurysms, thromboembolic disease, and myocardial infarction. Overall, it is an uncommon cause of chest pain in this cohort of patients.
Question 3
A. Correct! The majority of patients with idiopathic DCM do not show enhancement. However, approximately 40% can show mid-wall linear enhancement in the septum.
Other choices and discussion
B. The majority of patients with HCM show patchy mid-wall enhancement in the hypertrophied segments.
C. Ischemic cardiomyopathy is characterized by subendocardial enhancement in a coronary artery distribution.
D. In cardiac amyloidosis, there is global subendocardial enhancement or diffuse enhancement throughout the myocardium.
E. Eosinophilic myocarditis is characterized by global subendocardial enhancement in the apical regions, and apical LV thrombus may also be present.
Suggested Reading
Dastidar AG, Rodrigues JCL, Ahmed N, et al. The role of cardiac MRI in patients with troponin-positive chest pain and unobstructed coronary arteries. Curr Cardiovasc Imaging Rep 2015;8:28Top Tips
Acute myocarditis is usually due to a viral infection of the myocardium and may present with acute chest pain in the presence of normal coronary arteries.
CMR is useful for noninvasive diagnosis and risk stratification in acute myocarditis.
CMR features of acute myocarditis include wall motion abnormalities, pericardial effusion, myocardial edema, and typically subepicardial delayed enhancement, particularly in the lateral wall of the LV.
Essentials 8
Case
A 35-year-old woman presents with heart failure and monocular blindness.

Questions
1. The CORRECT diagnosis is:
A. Multivessel coronary artery disease
B. Cardiac sarcoidosis
C. Arrhythmogenic right ventricular dysplasia/cardiomyopathy
D. Idiopathic dilated cardiomyopathy
E. Hypertrophic cardiomyopathy
2. Which of the following statements BEST characterizes the case diagnosis?
A. A majority of patients are symptomatic.
B. Histologic confirmation is needed before treatment.
C. Conduction disturbances may be evident on electrocardiogram.
D. Corticosteroid treatment is contraindicated.
E. Pathognomonic findings are seen on echocardiography.
3. The most common area of scarring/late gadolinium enhancement in cardiac sarcoidosis is:
A. Basal interventricular septum
B. Inferior left ventricle
C. Lateral left ventricle
D. Anterior left ventricle
E. Anterior right ventricle
* Videos in this chapter can be accessed at MediaCenter.Thieme.com. Please follow the instructions found on the MediaCenter page at the front of this book.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


