11 Spinal Trauma in the Elderly
Background
The aged population is increasing in most industrialized countries. In Japan, low birth and death rates have contributed to a significant increase in the aged population. Between 2005 and 2010, those aged 65 years or older will comprise 20% of the population, and in 2015 that Figure will reach 25%.1 Such an increase in the aged population will also be observed in North America and Europe.2 The increased physically active aged population also has a higher chance of major trauma including traffic accidents, and falling at home also contributes to the increased chance of injury to the spine.
Injury to the spine due to major trauma is considered to be common among the young and physically active population, but another peak is present in the older age group of the late 50s and 60s.3 In our institution, approximately 2/3 of spinal injury patients are older than 50 years, and the mean age is the mid 50s. Although fractures of the spine and dislocations due to major trauma are common in the young age groups, elderly people are more likely to sustain significant injury through minor trauma.
In general, the clinical manifestations of spinal injury in the elderly are more complicated and the diagnosis is more difficult and may be delayed due to variation in associated mental, social, and morphological states. In elderly patients, injury in the cervical spine is less common, and the injuries tend to be less severe; however, mortality rates are relatively high.4 In addition, the imaging evaluation is more difficult due to associated age-related processes, including spondylosis deformans and paravertebral ligamentous ossification, accentuated kyphosis, compression fractures, and degenerative scoliosis. Detecting traumatic change in the associated degenerative process is important for diagnosing spinal injury in the aged population.
Cervical Spine
Biomechanical Characteristics
Flexion, extension, and axial loading are all causes of injury to the spine, and susceptibility to trauma depends on age, gender, and loading rate. Decreased bone mineral content makes the spine vulnerable to axial loading, but it is more significant in the thoracolumbar vertebrae. Hyperflexion and hyperextension are common mechanisms of cervical spine injury. Cervical spine injury in young patients is usually caused by a high loading rate, but in the elderly, injury also occurs with low loading rates.5
The range of motion of the cervical spine decreases with age, due to development of spondylosis deformans, including ligamentous degeneration and ossification.6 Cervical spine injury with rigid segments most often occurs through or adjacent to such a segment. Increased rigidity may be the reason for the high frequency of upper cervical spine injury in the elderly.7 Hyperextension injury is often seen in the upper cervical spine in the younger population; however, such injury commonly occurs in the mid and lower cervical levels in the elderly,8 probably because of decreased tensile strength of the ligaments.
Clinical Features
Clinical evaluation of injured elderly patients is often difficult due to altered physiological and mental states. Cervical spine injury occurs often under the influence of alcohol, or physical or mental disorders, and this may make clinical assessment difficult. Neck pain is still the most significant initial symptom, but other symptoms often conceal neck complaints.
Although traffic accidents are by far the most common cause of injury in the general population, falling is the most common cause of cervical spine injury in most studies of spine injury in the elderly. In the elderly, falling causes 2/3 to 3/4 of cervical spine injury: 78% in Lieberman and Webb’s study of patients older than 65 years.9 Falling down the stairs is the most common injury at home, and it is often associated with loss of consciousness. The cause of the loss of consciousness may be a sign of more serious disorders.
The injury pattern in the elderly may be more complicated than in the younger population. In previous reports on cervical spine injury in the elderly, upper cervical spine injury, particularly dens fractures, is frequent, whereas lower cervical spine injury is more frequent in the younger population.7,10,11
On the other hand, the spondylotic spine tends to be injured in the lower cervical spine, which is particularly associated with degenerative changes.8 This is due to the high frequency of hyperextension injury of the spondylotic lower cervical spine caused by falling. Hyperextension injury is typically common in older people, whereas hyperflexion and compression injury are relatively common in younger people.12 There are two mechanisms of hyperextension injury: direct anterior craniofacial trauma, where people typically fall and hit their foreheads, and forced hyperextension in rear-end motor vehicle collisions, which is more common in younger and active people.
In hyperextension injury, central cord syndrome is the most common spinal cord injury, in which the pinching of the spinal cord may be caused by the bulged ligamentum flavum during hyperextension.13 The central cord syndrome tends to occur at more than one level, based on MR imaging.14 The prognosis of spinal cord injury is generally worse than in younger people.10,15
Hyperflexion injury, a common type of injury, is also seen in elderly patients. No specific type of injury is reported to be common in the elderly, but interfacetal fracture-dislocation is a typical injury in the mid and lower cervical spine.
Imaging Techniques
Imaging techniques are essentially the same as in the younger age group.16 Plain radiography, particularly a high-quality lateral view, is of prime importance as in the younger age group, but associated degenerative or other disorders make the assessment of traumatic change more difficult. Adequately including the lower cervical spine is particularly important in elderly patients.
Although routine use of helical CT for vertebral trauma is controversial, multi-detector row CT (MDCT) makes evaluation of the wide zones of the spinal column easy. When fracture or dislocation is suspected by clinical data, a volume scan with multi-planar reconstruction by MDCT needs to be performed without delay.17 In multi-trauma patients, evaluation of the whole spine by MDCT is particularly useful to assess multiple levels of traumatic lesions.
MR imaging is indicated whenever there is discrepancy between imaging features and neurological findings.16 We routinely obtain sagittal T1W spin-echo, sagittal T2W (fast) spin-echo, and axial T2W (fast) spin-echo (or gradient-echo) images after a localizing scan with no contrast medium. Among them, the midsagittal T2W images are the most important screening method for the presence or absence of edema or hematoma in the paravertebral soft tissue and spinal cord.18 Sagittal T1W images are sensitive to the detection of bone marrow trabecular bone fractures and highsignal cord hematoma. Axial T2W images are used to confirm and determine the localization of spinal cord injury, since artifacts often overlie the cord on sagittal images.
Radiological Features
There are no specific types of injury in elderly people, but a dens fracture and hyperextension injury due to falling is relatively common. Associated degenerative changes often modify traumatic change.19
SCIWORA (Spinal Cord Injury Without Radiographic Abnormalities)
The lack of findings of trauma is one of the characteristic imaging features of cervical spine injury in old people. Different from SCIWORA in children, trauma findings are hidden by degenerative changes. Senescent and pathological changes overlap, particularly in degenerative changes in the endplate and osteophyte formation, and the differentiation is often difficult. In Bryson et al’s study of 174 patients older than 40 years, only 8 patients had findings of acute injury.20 In Regenbogen et al’s study of 88 patients older than 40 years, no bone abnormalities were seen in 28%, and minimal abnormalities were seen in 20%.8 Another cause of this low sensitivity of plain radiography is probably related to the high frequency of hyperextension injury.
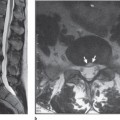
Hyperextension Injury
Hyperextension injury is usually a stable injury, and bone changes on plain radiography are frequently absent (Fig. 11.1).21 Widening of the disk space is often the only finding. Prevertebral hematoma is frequently associated with this injury. In the study of EdeikenMonroe et al, the combination of diffuse prevertebral soft tissue swelling and normal alignment of the cervical spine were the only findings in 30% of their cases.22 MR imaging is particularly useful for evaluation of hyperextension injury in demonstrating injuries in the anterior longitudinal ligament and the anterior annulus, and occult endplate fractures.14 In addition, hemorrhagic necrosis in the spinal cord caused by impaction is only seen on MR imaging.23 The cord edema tends to extend to multiple levels,14 but the degree of signal abnormalities varies.
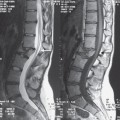
Dens Fracture
The dens fracture has been reported to be the most common spinal injury in the elderly. It can be detected on plain radiography without MR imaging, but the diagnosis is often delayed, as seen in the younger age group (Fig. 11.2).24 The pattern of dens fracture in elderly patients is controversial. An impaction fracture at the base of the dens (type III) may be characteristic in elderly patients with osteoporosis.25 Posterior displacement of the dens may occur due to hyperextension. Anderson-D’Alonzo type III fractures were commonly seen in one study,26 but in another study, the type II injury was more common.27
Fractures and Dislocations Associated with Rigid Segments
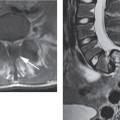
Spondylosis Deformans
Spondylosis deformans is an aging process characterized by degeneration of the intervertebral disks and a degenerative process of the diskovertebral and zygapophyseal joints. The degenerative process is evident in the majority of spine injury cases.8,20 The loss of flexibility contributes to the increased risk of trauma. The injury tends to occur at or adjacent to the rigid segment, where the stress due to trauma concentrates (Fig. 11.3
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


