 FIGURE 11.1 Topographic anatomy of the C1 and C2 vertebrae. |
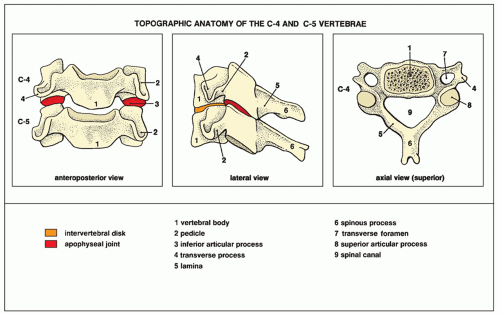 FIGURE 11.2 Topographic anatomy of the C4 and C5 vertebrae, representing the midcervical and lower cervical vertebrae. |
 FIGURE 11.3 Lateral view. (A) For the erect lateral view of the cervical spine, the patient is standing or seated, with the head straight in the neutral position. The central beam (red broken line) is directed horizontally to the center of the C4 vertebra (at the level of the chin). (B) For the cross-table lateral view, the patient is supine on the radiographic table. The radiographic cassette (a grid cassette to obtain a clearer image) is adjusted to the side of the neck, and the central beam is directed horizontally to a point (red dot) approximately 2.5 to 3 cm caudal to the mastoid tip. (C) The radiograph in this projection clearly shows the vertebral bodies, apophyseal (facet) joints, spinous processes, and intervertebral disk spaces. It is mandatory to demonstrate the C7 vertebra. (Continued) |
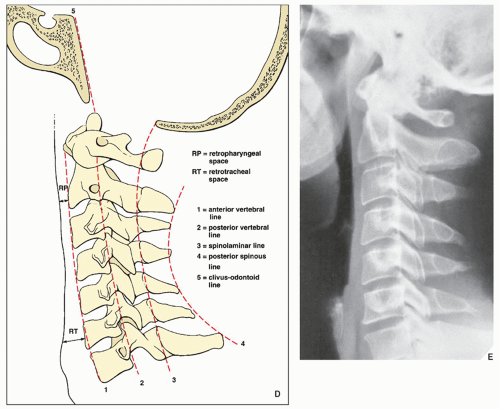 FIGURE 11.3 Lateral view. Continued (D) With this view, the five contour lines of the normal cervical spine can be demonstrated: anterior vertebral line drawn along anterior margins of the vertebral bodies; posterior vertebral line (outlines anterior margin of spinal canal), drawn along posterior margins of the vertebral bodies; spinolaminar line (outlines posterior margin of the spinal canal), drawn along the anterior margins of the bases of the spinous processes at the junction with lamina; posterior spinous line drawn along the tips of the spinous processes from C2-7, which should be running smoothly, without angulation or interruption; and the clivus-odontoid line, drawn from the dorsum sellae along the clivus to the anterior margin of the foramen magnum should point to the tip of the odontoid process at the junction of the anterior and middle thirds. The retropharyngeal space (distance from the posterior pharyngeal wall to the anteroinferior aspect of C2) should measure 7 mm or less; the retrotracheal space (distance from the posterior wall of the trachea to the anteroinferior aspect of C6) should measure no more than 22 mm in adults and 14 mm in children. (E) Radiograph obtained with low-kilovoltage technique demonstrates prevertebral soft tissues to better advantage. |
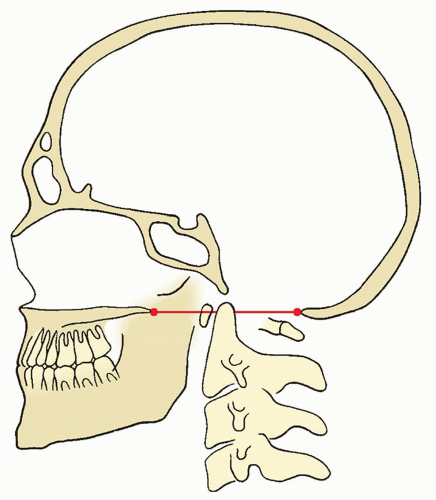 FIGURE 11.4 The Chamberlain line. This line is drawn from the posterior margin of the foramen magnum (opisthion) to the dorsal (posterior) margin of the hard palate. The odontoid process should not project above this line more than 3 mm; a projection of 6.6 mm (±2 standard deviation [SD]) above this line strongly indicates cranial settling. |
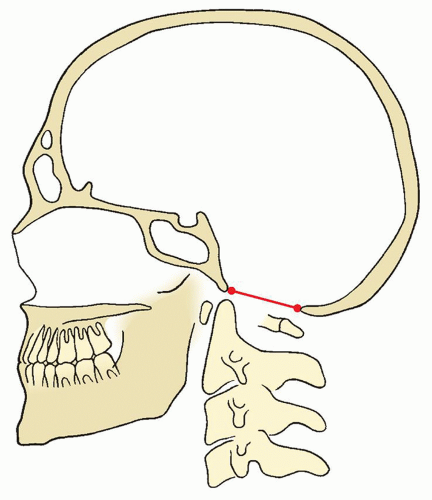 FIGURE 11.5 The McRae line. This line defines the opening of the foramen magnum and connects the anterior margin (basion) with posterior margin (opisthion) of the foramen magnum. The odontoid process should be just below this line or the line may intersect only at the tip of the odontoid process. In addition, a perpendicular line drawn from the apex of the odontoid to this line should intersect it in its ventral quarter. |
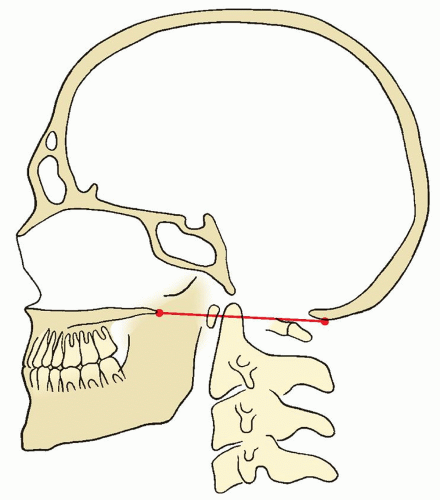 FIGURE 11.6 The McGregor line. This line connects the posterosuperior margin of the hard palate to the most caudal part of the occipital curve of the skull. The tip of the odontoid normally does not extend more than 4.5 mm above the line. |
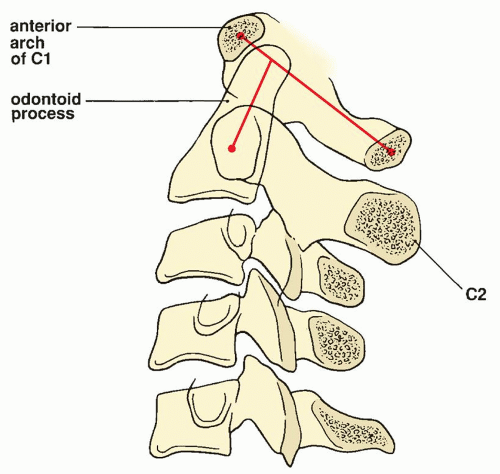 FIGURE 11.7 Ranawat method. Ranawat and associates developed a method for determining the extent of the superior margin of the odontoid process, since the hard palate often is not identifiable on radiographs of the cervical spine. The coronal axis of C1 is determined by connecting the center of the anterior arch of the first cervical vertebra with its posterior ring. The center of the sclerotic ring in C2, representing the pedicles, is marked. The line is drawn along the axis of the odontoid process to the first line. The normal distance between C1 and C2 in men averages 17 mm (±2 mm SD), and in women, 15 mm (±2 mm SD). A decrease in this distance indicates cephalad migration of C2. |
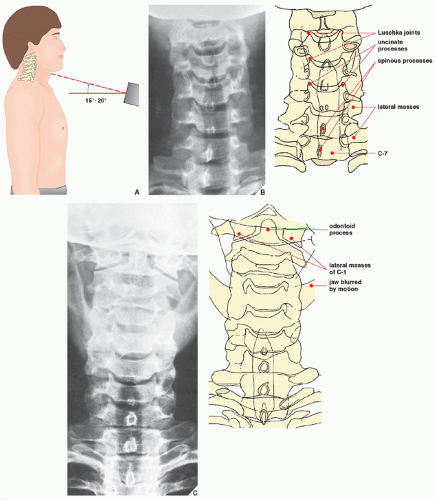 FIGURE 11.8 Anteroposterior view. (A) For the anteroposterior view of the cervical spine, the patient is either erect or supine. The central beam is directed toward the C4 vertebra (at the point of the Adam’s apple) at an angle of 15 to 20 degrees cephalad. (B) The radiograph in this projection demonstrates the C3-7 vertebral bodies and the intervertebral disk spaces. The spinous processes are seen superimposed on the bodies, resembling teardrops. The C1 and C2 vertebrae are not adequately seen. For their visualization, the patient is instructed to open and close the mouth rapidly. Motion of the mandible blurs this structure, and C1 and C2 become visible (C). |
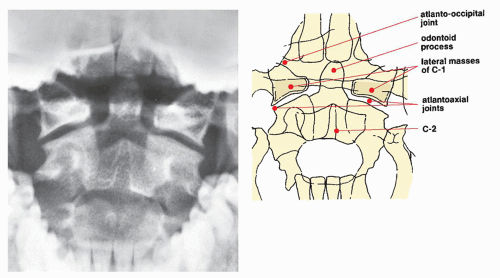 FIGURE 11.9 Open-mouth view. For the open-mouth view, the patient is positioned in the same manner as for the supine anteroposterior projection; the head is straight, in the neutral position. With the patient’s mouth open as widely as possible, the central beam is directed perpendicular to the midpoint of the open mouth. During the exposure, the patient should softly phonate “ah” to affix the tongue to the floor of the mouth so that its shadow is not projected over C1 and C2. On the radiograph obtained in this projection, the odontoid process, the body of C2, and the lateral masses of the atlas are well demonstrated; the atlantoaxial joints are seen to best advantage. |
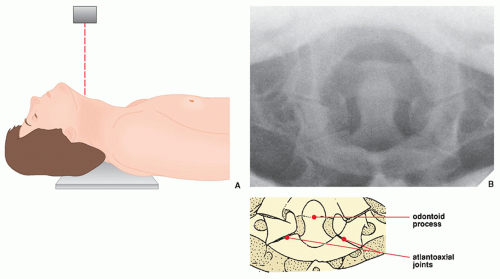 FIGURE 11.10 Fuchs view. (A) For the Fuchs views of the odontoid process, the patient is supine on the table, with the neck hyperextended. The central beam is directed vertically to the neck just below the tip of the chin. (B) On the radiograph obtained in this projection, the odontoid, especially its upper half, is clearly visualized. |
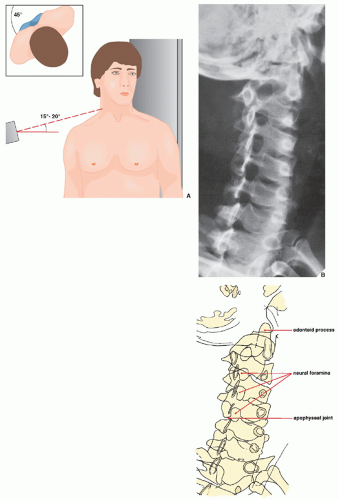 FIGURE 11.11 Oblique view. (A) An oblique view of the cervical spine may be obtained in the anteroposterior (as shown here) or posteroanterior projection. The patient may be erect or recumbent, but the erect position (seated or standing) is more comfortable. The patient is rotated 45 degrees to one side—to the left, as shown here, to demonstrate the right-sided neural foramina and to the right to demonstrate the left-sided neural foramina. The central beam is directed to the C4 vertebra with 15- to 20-degree cephalad angulation. (B) The radiograph obtained in this projection is effective primarily for demonstrating the intervertebral neural foramina. |
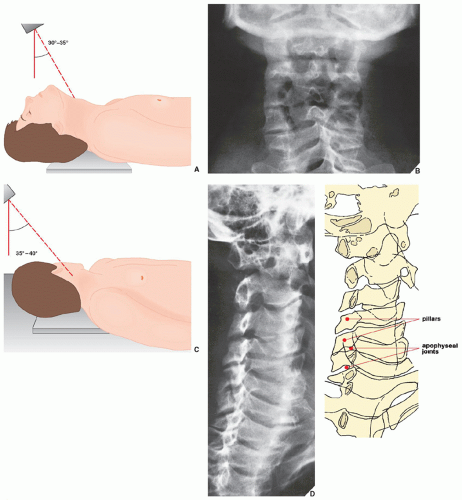 FIGURE 11.12 Pillar view. (A) For the pillar view of the cervical spine, the patient is supine on the table, with the neck hyperextended. The central beam is directed to the center of the neck in the region of the thyroid cartilage at a caudal angulation of 30 to 35 degrees. (B) On the radiograph obtained in this projection, the lateral masses (pillars) of the cervical vertebrae are well demonstrated. (C) The pillar view can also be obtained in the oblique projection. The patient is supine on the table, with the neck hyperextended and the head rotated 45 degrees toward the unaffected side. The central beam is directed with about 35- to 40-degree caudal angulation to the lateral side of the neck about 3 cm below the earlobe. (D) On the radiograph obtained with leftward rotation of the head, an oblique view of the right pillars is achieved. |
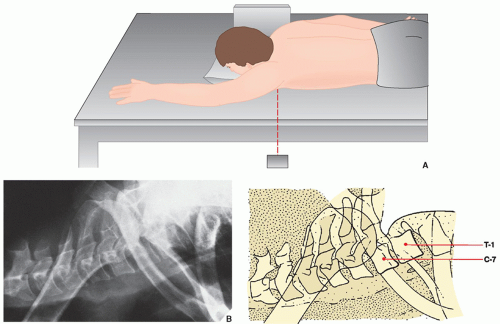 FIGURE 11.13 Swimmer’s view. (A) For the swimmer’s view of the cervical spine, the patient is placed prone on the table with the left arm abducted 180 degrees and the right arm by the side, as if swimming the crawl. The central beam is directed horizontally toward the left axilla. The radiographic cassette is against the right side of the neck, as for the standard cross-table lateral view. (B) The radiograph obtained in this projection provides adequate visualization of the C7, T1, and T2 vertebrae, which would otherwise be obscured by the shoulders. |
satisfactory “myelographic effect” between cerebrospinal fluid and adjacent structures (Fig. 11.16C,D).
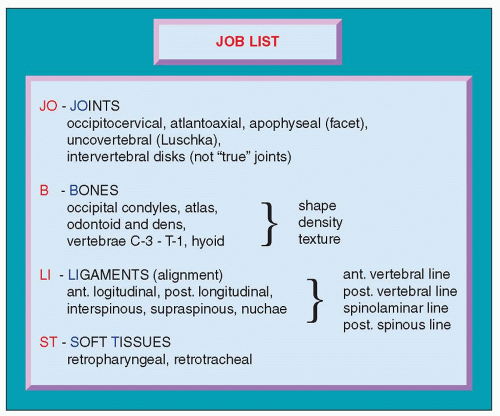 FIGURE 11.14 JOB LIST for evaluation of the cervical spine. |
 FIGURE 11.15 CT of the cervical spine. CT sections through the body of C6 (A), C7 (B), and the C6-7 intervertebral space (C) show the normal appearance of these structures. |
and “minor” injuries. The former are defined as having either radiographic or CT evidence of instability, with or without associated localized or central neurologic findings. The latter injuries have no radiographic or CT evidence of instability and do not produce or have no potential to cause neurologic findings. According to these authors, cervical injury should be classified as major if the following radiographic and CT criteria are present: displacement of more than 2 mm in any plane, widening of the vertebral body in any plane, widening of the interspinous or interlaminar space, widening of the facet joints, disruption of the posterior vertebral body line, widening of the disk space, vertebral burst, locked or perched facets either unilateral or bilateral, “hanged man” fracture of C2, fracture of the odontoid process, and type III occipital condyle fracture. All other types of fractures are considered to be minor.
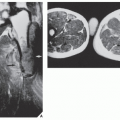
 FIGURE 11.16 MRI of normal cervical spine. (A) T1-weighted spin echo sagittal midline section demonstrates anatomic details of the bones and soft tissues. The craniocervical junction is well outlined. The foramen magnum is defined by the fat within the occipital bone and clivus. The anterior and posterior arches of C1 appear as small oval marrow-containing structures at the upper cervical spine. The spinal cord is of an intermediate signal intensity outlined by lower signal of cerebrospinal fluid. The intervertebral disks are imaged with low signal intensity. (B) Parasagittal T2-weighted section demonstrates the apophyseal joints. (C) Short time inversion recovery (STIR) sagittal image shows vertebral bodies and spinous processes to be of low signal intensity. The high water content of the intervertebral disks produces a very high signal similar to that of cerebrospinal fluid. The cord is imaged as an intermediate-signal intensity structure. (D) Axial gradient recalled echo (GRE) section demonstrates neural foramina and nerve roots. The cervical cord is well outlined. |
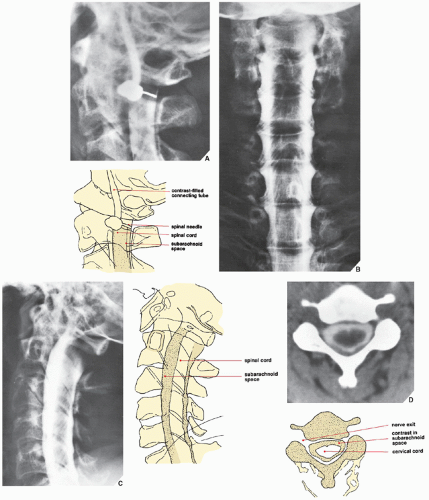 FIGURE 11.17 Myelography of the cervical spine. For myelographic examination of the cervical spine, the patient is recumbent on the table, lying on the left side. Using fluoroscopy, the point of entrance of the needle is marked at the C1-2 level, and a 22-gauge needle is inserted vertically, the tip being directed to the dorsal aspect of the subarachnoid space, above the lamina of C2. Free flow of spinal fluid indicates the correct position of the needle. (A) Approximately 10 mL of iohexol or iopamidol, watersoluble nonionic iodinated contrast agents, at a concentration of 240 mg iodine per mL, is slowly injected. Radiographs are obtained in the posteroanterior (B), cross-table lateral (C), and oblique projections. (Oblique projections, however, are obtained not by rotating the patient but by angling the radiographic tube 45 degrees.) If the lower segment of the cervical spine is not satisfactorily demonstrated or if the upper thoracic segment needs to be visualized, a radiograph may also be obtained in the swimmer’s position. Myelography demonstrates the thecal sac filled with contrast and the outline of the normal nerve roots and nerve root sleeves. (D) CT section at the level C3-4 obtained following myelography demonstrates the normal appearance of contrast in the subarachnoid space. |
TABLE 11.1 Tissue Magnetic Resonance Imaging Signal Characteristics | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
TABLE 11.2 Standard and Special Radiographic Projections for Evaluating Injury to the Cervical Spine | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 11.3 Ancillary Imaging Techniques for Evaluating Injury to the Cervical, Thoracic, and Lumbar Spine | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||
TABLE 11.4 Classification of Injuries to the Cervical Spine by Mechanism of Injury and Stability | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 FIGURE 11.18 Anatomy of the principal ligaments of the cervical spine. |
Biomechanical studies have demonstrated that for this injury to occur, all major structures (alar ligaments, tectorial membrane, and occipital atlantal facet joint capsules) crossing the occipitocervical junction must be ruptured. This type of injury is seen more commonly in patients who survive transport to the hospital.
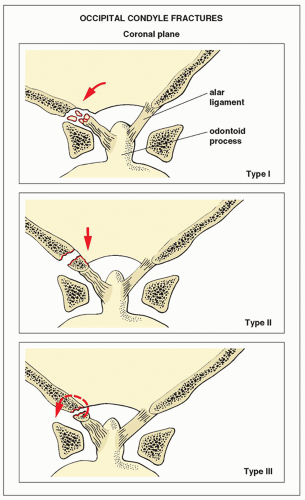 FIGURE 11.19 Anderson and Montesano classification of the occipital condyle fractures. (Modified from Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine 1988;13:731-736.) |
CT may also be required in the evaluation of complex fractures (Fig. 11.25C,D). MRI only occasionally is performed (Fig. 11.26).
 FIGURE 11.20 Fracture of the occipital condyle. A 23-year-old woman was injured in a motorcycle accident. (A) Coronal reformatted CT image shows a comminuted fracture of the right occipital condyle (arrows) and a fracture of the right lateral mass of the atlas (curved arrow). (B) 3D CT reconstructed image (bird’s eye view) shows no displacement of the fractured fragments (arrows) into the foramen magnum, classifying this injury as a type I. |
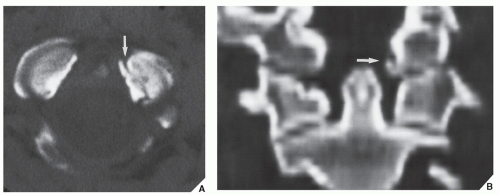 FIGURE 11.21 Fracture of the occipital condyle. A 16-year-old girl was assaulted and sustained a blow injury to the head. Conventional radiographs of the skull and upper cervical spine were interpreted as normal. (A) Axial CT section through the base of the skull shows a type III fracture of the left occipital condyle (arrow). (B) Coronal reformatted CT image confirms the presence of an evulsion fracture (arrow). |
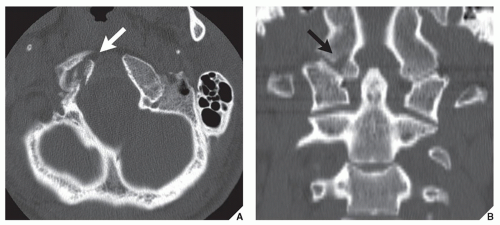 FIGURE 11.22 Fracture of the occipital condyle. An 18-year-old man was ejected from the convertible car during the accident. (A) Axial CT section through the base of the skull and (B) coronal reformatted CT image show a type III fracture of the right occipital condyle (arrows). Note displaced fragment of the occipital condyle toward the odontoid process. |
 FIGURE 11.23 Occipitocervical dislocation. (A) Lateral radiograph of the cervical spine in a 24-year-old man, who injured his head and neck in a motorcycle accident that resulted in complete quadriplegia, shows type I of occipitocervical dislocation: The occipital condyles are anteriorly displaced in relation to C1 vertebra. (B) In another patient, lateral radiograph demonstrates a type IIA vertical occipitocervical dislocation. (A, From Greenspan A, Montesano PX. Imaging of the spine in clinical practice. London, UK: Wolfe-Mosby-Gower Publishers; 1993, p. 2.19, Fig. 2.23; B, From Anderson PA, Montesano PX. Injuries to the occipitocervical articulation. In: Chapman MW, ed. Operative orthopaedics, vol. 4, 2nd ed. Philadelphia: JB Lippincott; 1993:2631-2640.) |
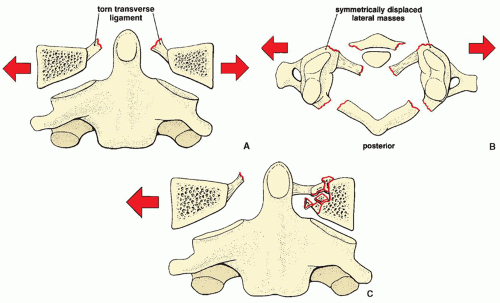 FIGURE 11.24 Jefferson fracture. The classic Jefferson fracture, seen here schematically on the anteroposterior (A) and axial (B) views, exhibits a characteristic symmetric overhang of the lateral masses of C1 over those of C2. Lateral displacement of the articular pillars results in disruption of the transverse ligaments. (C) On occasion, only unilateral lateral displacement of an articular pillar may be present. |
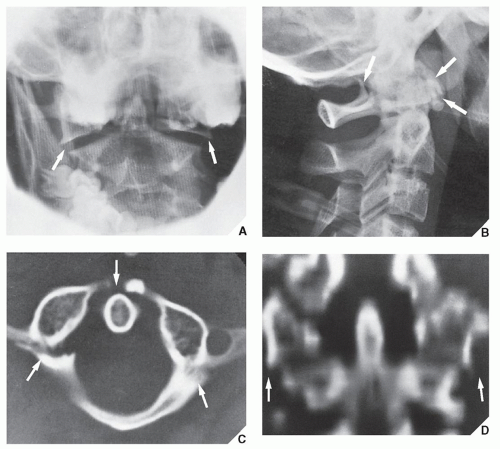 FIGURE 11.25 Jefferson fracture. A 19-year-old man sustained a neck injury while being mugged. (A) Open-mouth anteroposterior radiograph of the cervical spine shows lateral displacement of the lateral masses of the atlas (arrows), suggesting a ring fracture of C1. (B) Lateral radiograph demonstrates fracture lines of the posterior and anterior arch of C1 (arrows). (C) CT section demonstrates two fracture lines of the posterior arch and a fracture of the anterior arch (arrows). (D) CT coronal reformation confirms lateral displacement of the lateral masses (arrows). |
 FIGURE 11.26 Jefferson fracture. A 56-year-old man was hit on the top of the head during the industrial accident. (A) Later radiograph of the cervical spine shows a fracture of C1 (arrow). (B) Axial CT section and (C) 3D CT reconstructed image confirm unilateral fracture of the left anterior and posterior arches of C1 (arrow). |
which in fact constitutes traumatic spondylolisthesis of C2, is common in automobile accidents, when the face strikes the windshield before the vertex of the head, forcing the neck into hyperextension. This injury, which accounts for 4% to 7% of all cervical spine fractures and dislocations, may present as simple, nondisplaced fractures through the pedicles of the axis or as fractures through the arches with anterior subluxation and angulation of C2 onto C3 (Fig. 11.31). The fracture line usually lies anterior to the inferior articular facet of C2 in both variants, but displaced fractures are more often associated with ligament disruption and intervertebral disk injuries. The best projection for demonstrating this injury is the lateral radiograph (Fig. 11.32).
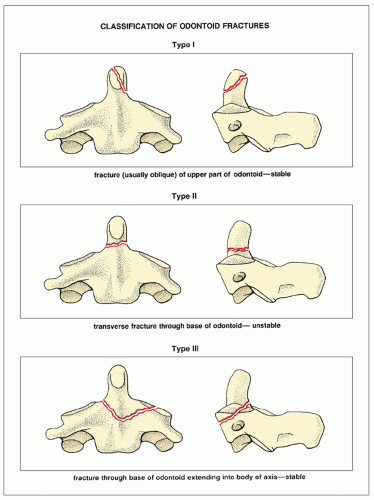 FIGURE 11.27 Classification of odontoid fractures. (Modified from Anderson LD, D’Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg [Am] 1974;56A:1663-1674.) |
 FIGURE 11.28 Fracture of the odontoid process. A 62-year-old man sustained a flexion injury of the cervical spine in an automobile accident. Open-mouth anteroposterior (A) and lateral (B) radiographs demonstrate a fracture line at the base of the odontoid process, but the details of this injury cannot be well appreciated. Thin-section trispiral tomographic sections in the anteroposterior (C) and lateral (D) projections confirm the fracture at the base of the dens. This is a type II (unstable) fracture. |
 FIGURE 11.29 Fracture of the odontoid process. A 24-year-old man fell on his head in a skiing accident. Open-mouth anteroposterior (A) and lateral (B) radiographs of the cervical spine demonstrate a fracture of the odontoid process extending into the body of C2 (arrows)—a type III stable fracture. The diagnosis was confirmed by trispiral tomography in the anteroposterior projection (C). |
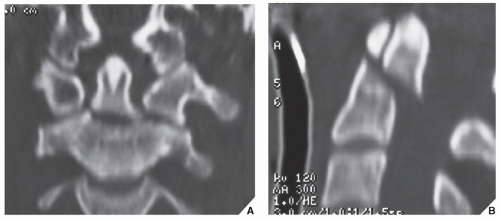 FIGURE 11.30 CT demonstration of fracture of the odontoid process. A 50-year-old man sustained a flexion neck injury during a motorcycle accident. The conventional radiographs of the cervical spine suggested odontoid fracture but were not conclusive. Coronal (A) and sagittal (B) reformatted CT images clearly demonstrate a type II odontoid fracture. |
 FIGURE 11.31 Hangman’s fracture. This injury may present as nondisplaced fractures through the arches of C2, as seen here schematically on the lateral (A) and axial (B) views, or as displaced fractures with anterior angulation (C) and (D) associated with disruption of ligaments, the intervertebral disk, or articular facets. |
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Anomalies of the Upper and Lower Limbs
Anomalies of the Upper and Lower Limbs
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


