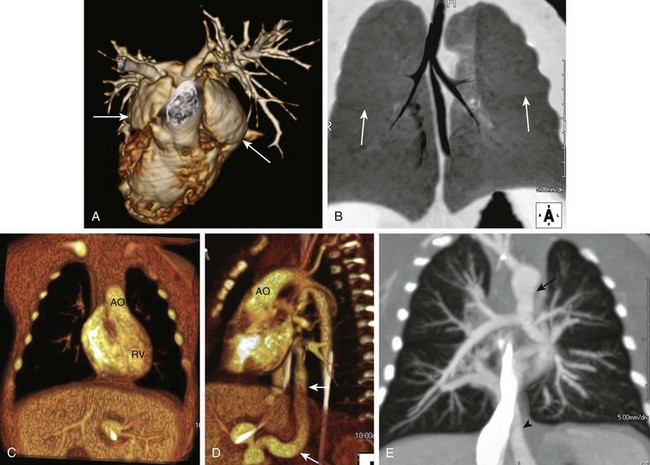
Chapter 79 A large number of syndromes, dysplasias, and chromosomal anomalies are associated with congenital or acquired cardiac and vascular disease. This chapter discusses the cardiovascular features of some commonly encountered lesions. A more extensive list is provided in Tables 79-1 to 79-3. Table 79-1 Syndromes, Dysplasias, and Their Associated Cardiovascular Anomalies Table 79-2 Syndromes that Predominantly Affect the Cardiovascular System Table 79-3 Chromosomal Anomalies and Their Associated Cardiovascular Defects Situs and Cardiosplenic (Heterotaxy) Syndromes Overview: The heterotaxy syndromes, that is, right and left isomerism, feature abnormalities of the visceral situs. These syndromes have an estimated incidence of 1 in 6000 to 1 in 20,000 live births and account for 1% of all congenital heart defects. Although heterotaxy usually occurs sporadically, familial cases have been described. Although visceral and atrial situs do not always correspond, body situs (from the Latin word meaning location) generally is divided into three types: solitus, inversus, and ambiguus. Situs solitus is the normal arrangement of the viscera in the body (see Chapter 63). Situs inversus is the mirror image of normal; it is seen in 0.01% of the population and is associated with a slightly higher incidence of congenital heart disease (3% to 5%) compared with the solitus population (0.6% to 0.8%). The most common cardiac abnormalities seen in patients with situs inversus are a right-sided aortic arch, atrioventricular discordance, and transposition of the great vessels. Situs ambiguus, or heterotaxy, encompasses all other visceroatrial arrangements. By definition, in situs ambiguus, visceral malposition and dysmorphism associated with an indeterminate atrial arrangement are present.1 Heterotaxy syndrome with right isomerism or bilateral right-sidedness is usually, but not invariably, accompanied by asplenia.1 The condition is more common in males and is characterized by bilateral systemic atria with broad trabeculated appendages (Fig. 79-1), bilateral trilobed lungs with bilateral minor fissures and short eparterial bronchi, a central horizontal liver, bowel malrotation, and the stomach in an indeterminate position (see Fig. 79-1). The abdominal aorta and inferior vena cava often are located on the same side of the spine, frequently in a posterior-anterior orientation. Other occasional anomalies include tracheoesophageal fistula, imperforate anus, absent gallbladder, pancreatic anomalies, fused adrenal glands, and genitourinary abnormalities.2 The prognosis for right isomerism is poor because of an abnormal immune status (asplenia) and the typically complex cardiac anomalies. Cardiac anomalies are almost invariable and cause the most common presenting symptoms: cyanosis and severe respiratory distress. The “right isomerism heart” often consists of a common atrioventricular canal, a single ventricle, a large ventricular septal defect (VSD), and a double-outlet right ventricle and/or transposition of the great vessels, along with pulmonary outflow obstruction or atresia and total anomalous pulmonary venous drainage (frequently obstructed) (see Fig. 79-1). The spectrum of cardiovascular anomalies also can include cardiac malposition (dextrocardia or mesocardia), tricuspid atresia, truncus arteriosus, right aortic arch, anomalous systemic venous return, and bilateral superior vena cavae.2,3 Heterotaxy syndrome with left isomerism or bilateral left-sidedness most often accompanies polysplenia. It is characterized by bilateral pulmonary atria with narrow fingerlike appendages, bilateral bilobed lungs, bilateral long hyparterial bronchi, a centrally located liver, the stomach in an indeterminate position, bowel malrotation, and multiclefted or multiple spleens (either right sided or left sided) (Fig. 79-2). An interrupted inferior vena cava with azygos continuation is the most consistent abdominal finding in left isomerism (see Fig. 79-2). Left isomerism is slightly more common in females and generally has a better prognosis than right isomerism with less complex cardiovascular disease. Other associated anomalies include ciliary dyskinesia, biliary atresia, and other gastrointestinal abnormalities including bowel malrotation and pancreatic anomalies, as well as congenital portosystemic shunts (see Fig. 79-2).2,4 Figure 79-2 This 3-year-old girl, whose mother was diabetic, has polysplenia and Abernethy malformation with hepatopulmonary syndrome. Cardiac anomalies are seen in more than 50% of patients who have heterotaxy syndrome with left isomerism. The common cardiovascular anomalies include abnormalities of the inferior and superior vena cavae, cardiac malposition, atrial septal defect (ASD), VSD, common atrioventricular canal, double-outlet right ventricle, and anomalous pulmonary venous return (usually partial).2,3
Syndromes and Chromosomal Anomalies
Syndrome
Cardiovascular Anomalies
Achondrogenesis
PDA, ASD, VSD, COA
Alagille syndrome (arteriohepatic dysplasia)
(see e-Fig. 79-13)
PS, PPS, ASD, VSD, TOF, PDA, PAT, PAPVR, dysplastic AV valves, COA
Apert syndrome (acrocephalosyndactyly)
ASD, PDA, VSD, PS, TOF, EFE, DEXTRO, COA
Arthrogryposis
CMY
Beckwith-Wiedemann syndrome (EMG syndrome)
CM, CMY, ASD, PDA, TOF, HPLH, subvalvular AS, cardiac fibromas
Cardioauditory syndromes
LVH, RVH
Cantrell syndrome (pentalogy of Cantrell) (see e-Fig. 79-14)
Combined sternal, pericardial, intracardiac, diaphragmatic, and anterior abdominal wall defects
Radiographic findings: sternal defect, ectopia cordis, CHD, ASD, VSD, PS, TOF, APVR, DEXTRO, ventricular diverticulum, intrapericardial herniation of abdominal organs; associated with Turner, trisomy 18, sirenomelia, and amniotic band syndromes
Cardiosplenic (heterotaxy) syndromes (see Figs. 79-1 and 79-2)
Right isomerism (see Fig. 79-1)
TAPVR, AVSD, pulmonary outflow obstruction or PAT, DORV, TGA, single atrium (R), single common ventricle, DEXTRO, TAT, TRU (rare), AO-IVC juxtaposition, bilateral right PAs, bilateral SVC, interrupted IVC
Left isomerism (see Fig. 79-2)
Cardiac malposition, single atrium (L), single ventricle, VSD, AVSD, DORV, APVR, interrupted IVC, bilateral left PAs, bilateral SVC
Cayler syndrome (cardiofacial syndrome)
ASD, PDA, VSD, AVSD, TOF, RAA, COA
CHARGE association
ASD, VSD, conotruncal malformations, PDA, TOF, parachute mitral valve
Degos syndrome (malignant atrophic papulosis)
MI, pericarditis, constrictive pericarditis, myocardial fibrosis, and renal, cerebral, coronary, visceral, and peripheral arteriopathy
Diamond-Blackfan syndrome (congenital red cell aplasia)
VSD, ASD, mitral valve dysplasia
Ehlers-Danlos syndrome (see Fig. 79-3)
MVP, dilated AO root, coronary and aortic aneurysms, dissection or rupture, AS, AR, TR, PS, ASD, VSD, TOF, DEXTRO, LV rupture, arteriovenous fistula
Ellis–van Creveld syndrome (chondroectodermal dysplasia)
Common atrium, ASD, AVSD
Fryns syndrome
Septal defects, arch anomalies, TOF, cystic hygroma
Hallermann-Streiff syndrome (oculomandibulofacial syndrome)
PS, TOF, ASD, VSD
Holt-Oram syndrome (heart-hand syndrome) (see e-Fig. 79-10)
ASD, VSD, MVP, PDA, HPLH, TAPVR, TRU, conduction disorder, hypoplastic peripheral vessels
Jeune syndrome (asphyxiating thoracic dystrophy)
CHF
Kartagener syndrome (primary ciliary dyskinesia) (see e-Fig. 79-11)
DEXTRO, CHD
Klippel-Trénaunay-Weber syndrome (angioosteohypertrophy syndrome)
CHF, pericardial effusion, superficial varices, telangiectatic nevi, organ hemangiomas, lymphatic obstruction
LEOPARD syndrome (cardiomyopathic lentiginosis) (see e-Fig 79-8)
CMY, conduction defect, PS, sub-AS
Loeys-Dietz syndrome (see Fig. 79-5)
Congenital heart defects include patent ductus arteriosus, bicuspid aortic valve, bicuspid pulmonary valve, mitral valve prolapse, and atrial septal defect; arterial tortuosity, stenoses, aneurysms, dissection, diffuse arterial involvement; spontaneous rupture of viscera
Marfan syndrome (see Fig. 79-4)
MVP, MR, dilation of AO root, AR, CHF, aneurysms (AO, pulmonary, ductus), AO dissection, MI, arrhythmia, TR, ASD, TOF
MELAS syndrome
CMY, CHF, conduction abnormalities
Mucolipidosis III
AR
Mucopolysaccharidoses
IH (Hurler syndrome)
Acute CMY associated with EFE, AR, MR, MS, arteriopathy (coronary, renal, AO, mesenteric)
IS (Scheie syndrome)
AS, MS
II (Hunter syndrome)
AR, CHF, valve thickening, CMY
III (Sanfilippo syndrome)
CMY, MR, AR
IV (Morquio syndrome)
AR, CMY, AS, MR, CAD
VI (Maroteaux-Lamy syndrome)
AS, MS, CMY
Neurofibromatosis type 1 (see Fig. 79-6)
PS, COA, ASD, VSD, CMY, MVP, AS, TOF, PDA, vasculopathy (coronary, pulmonary, renal, systemic), cardiac neurofibroma, arteriovenous fistula, lymphatic abnormality
Noonan syndrome (Turner phenotype with normal karyotype)
PS, dysplastic pulmonic valve, hypertrophic CMY, lymphatic abnormalities, PDA, ASD, COA, mitral valve abnormalities, AS, pericarditis, APVR, coronary anomalies
Oculoauriculovertebral dysplasia (Goldenhar syndrome)
TOF, VSD, DORV, PAT, TAPVR, RAA, COA, asplenia
PHACES
Arch atresia, aberrant subclavian origins, hypoplasia of the descending thoracic aorta, double aortic arch, COA, stenosis and aneurysm formation of the aorta and the cervical arteries, stroke
Progeria (Hutchinson-Gilford syndrome)
Accelerated atherosclerosis, CM, MI, CHF, stroke
Proteus syndrome
CHD, CMY, myocardial mass, conduction abnormality, venous dilation, hemangioma, lymphangioma
Ravitch syndrome (thoracoabdominal wall defect)
Ectopia cordis, pentalogy of Cantrell, TGA, PDA, ASD, VSD, PS, TOF
Robinow syndrome (fetal face syndrome)
CHD (right heart lesions)
Rubinstein-Taybi syndrome
ASD, VSD, PDA, COA, PS, bicuspid AO valve
Silver-Russell syndrome
CHD
Smith-Lemli-Opitz syndrome
ASD, complex cardiac anomalies
Thrombocytopenia–absent radius (TAR) syndrome
COA, ASD, VSD, PDA, AVSD, TOF
Tuberous sclerosis (Bourneville-Pringle syndrome) (see Fig. 79-7)
Rhabdomyoma, hamartoma, CHF, CMY, COA, arrhythmia, arterial aneurysm and stenosis (AO, cerebral, renal, peripheral)
VATER/VACTERL association (see Fig. 79-9)
VSD, ASD, PDA, TOF, TGA, single ventricle
Velocardiofacial syndrome (Shprintzen syndrome)
TOF, TRU, PA, VSD, absent pulmonary valve, TGA, AS, interrupted AO arch, RAA
Williams syndrome (e-Fig. 79-12)
Supravalvular AS, PPS, MR, ASD, VSD, TOF, MI, COA, interrupted arch, hypoplastic AO, aneurysm or stenosis (AO, systemic, renal, cerebral arteries)
Zellweger syndrome (cerebrohepatorenal syndrome)
CHD, PDA, VSD, DiGeorge
Syndrome
Cardiovascular Defects
Absent pulmonary valve leaflet syndrome (see e-Fig. 79-15)
Maldeveloped nodular myxoid pulmonary valve cusps with aneurysmal dilation of central PAs associated with TOF, airway compression, lobar emphysema and abnormal PA branching, CM, RAA, ASD, VSD, PDA, DORV, AVSD, Marfan syndrome, 18q deletion
Berry syndrome
Distal AP window with AO origin of the right PA and arch interruption
Bland-White-Garland syndrome
Anomalous origin of left coronary artery from PA
Congenital cardiomyopathy: hypertrophic cardiomyopathy
Asymmetric septal hypertrophy, systolic anterior motion of mitral valve, LVOT obstruction, myocardial scar arrhythmias
Arrhythmogenic right ventricular dysplasia
Fibrofatty infiltration of right ventricular myocardium, RV dyskinesia/aneurysms, arrhythmias
Eisenmenger syndrome
Pulmonary hypertension with bidirectional or reversed shunt at atrial, ventricular, or AP level; cyanosis; dyspnea; sudden death; peripartum CMY radiographic findings: dilated central PAs with tapering, PA calcification
Floppy valve syndrome
MVP, prolapse of other valves, CAD, congestive or hypertrophic CMY, ASD, MR, AR, papillary muscle or chordae tendineae rupture
Hypoplastic left heart syndrome
Combined mitral and AO obstruction (stenosis or atresia), underdeveloped LA and LV, hypoplastic ascending AO ± COA or AO interruption; may be associated with right diaphragmatic hernia, omphalocele, brain anomalies; radiographic findings: CM and pulmonary edema
Lutembacher syndrome
ASD associated with MS
Postmyocardial infarction syndrome (Dressler syndrome)
Chest pain, fever, polyserositis—several weeks postinfarction; radiographic findings: pericardial or pleural effusion, noncardiogenic edema
Postpericardiotomy syndrome
Chest pain, fever, joint pain—weeks or months after closed or open heart surgery; radiographic findings: pericardial or pleural effusion, noncardiogenic pulmonary edema, constrictive pericarditis
Romano-Ward syndrome
Familial Q-T prolongation, arrhythmias, syncope
Shone syndrome (or complex) (see e-Fig. 79-16)
Complex of multiple left-sided obstructions, parachute mitral valve, supravalvular ring of LA, sub-AS, COA
Sick sinus syndrome
Arrhythmias
Tetralogy of Fallot (see Fig. 79-9 and e-Fig. 79-15)
Combination of VSD, overriding AO, RVH, RV outflow obstruction; may be PS and PPS
Trilogy of Fallot
PS, ASD (or PFO), right-to-left shunting
Uhl syndrome (anomaly)
Congenital aplasia of RV myocardium, RV CMY
Wolff-Parkinson-White syndrome
Aberrant intracardiac ECG pathway producing arrhythmias; associated with Ebstein anomaly, IHSS, levo-TGA, giant RA diverticulum
Chromosomal Anomaly
Cardiovascular Defects
Fragile X
MVP, MR, AR, TR, dilated AO root, COA
Trisomy 13 (Patau syndrome)
PDA, VSD, ASD, DEXTRO, capillary hemangioma, cervical cystic hygroma
Trisomy 18 (Edwards syndrome)
VSD, polyvalvular heart disease (pulmonary and AO valves), ASD, PDA, COA, TOF, TGA, HPLH, VACTERL, pentalogy of Cantrell
Trisomy 21 (Down syndrome) (see Fig. 79-18)
AVSD, VSD, ASD, TOF, PDA, PS, MVP, aberrant right SCA, intimal arterial fibrodysplasia, lymphatic abnormality, upper airway obstruction and CHF
Cat-eye syndrome (trisomy or tetrasomy 22)
TAPVR, TOF
Monosomy X, XO (Turner syndrome) (see Fig. 79-19)
COA, bicuspid AO valve, AO dissection, septal defects, abnormal mitral valve, sub-AS, PS, APVR, pentalogy of Cantrell, DEXTRO, RAA, hemangioma, lymphangiectasia, venous anomalies
XXY (Klinefelter syndrome)
MVP, Takayasu arteritis, cerebral aneurysms, varicose veins
Deletion Syndromes
Monosomy 1p36 syndrome
Dilated CMY, PDA
22q11 (predominantly DiGeorge syndrome (CATCH 22), also velocardiofacial syndrome) (see Fig. 79-17)
Type B interrupted arch, RAA, VSD, TOF, TRU, COA, aberrant right SCA, isolated SCA
5p: Cri du chat syndrome
CHD
4p: Wolf-Hirschhorn syndrome
ASD, VSD, valve anomalies, complex CHD, persistent left SVC
17p: Miller-Dieker syndrome (lissencephaly type 1)
ASD, CHD, conduction abnormalities
18q syndrome
Absent pulmonary valve, PDA, AS, dilated ascending AO
Syndromes
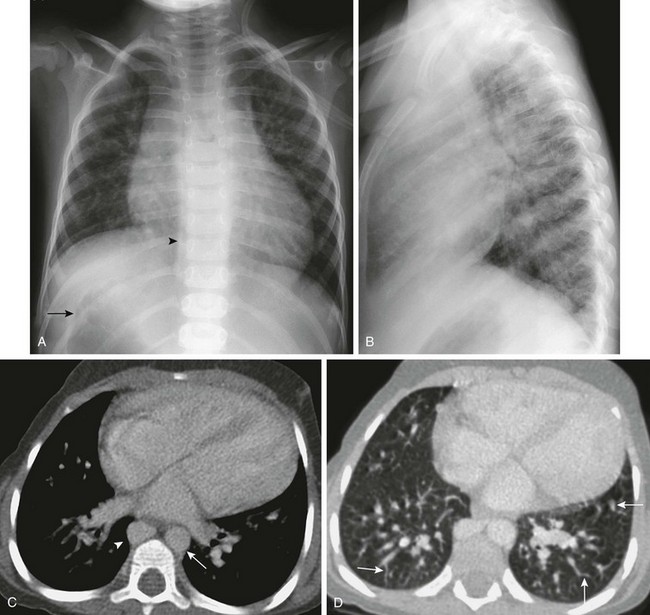
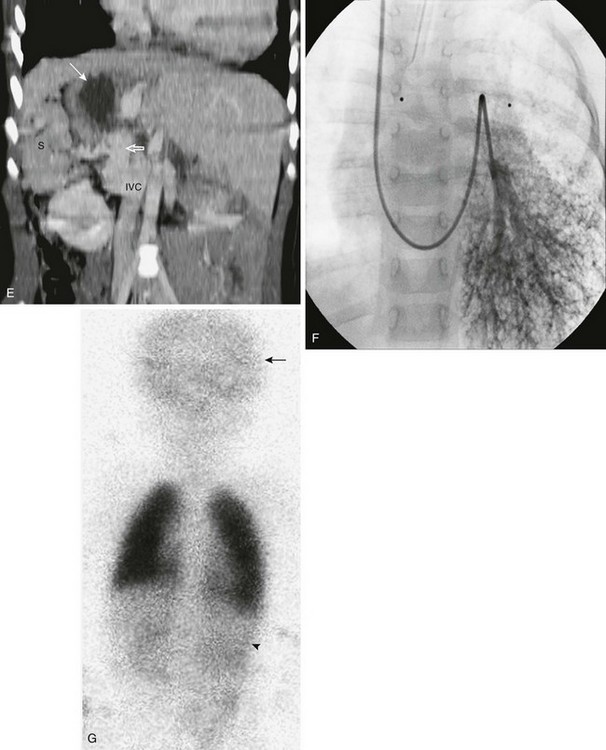
A, A posteroanterior view of the chest shows heterotaxy with a left-sided cardiac apex, right-sided stomach (arrow), and left-sided liver. Cardiomegaly and increased pulmonary vascularity (a small atrial septal defect and pulmonary arteriovenous shunting) are present. It is difficult to see the bilateral left-sided bronchi. A prominent right paraspinal line is present as a result of an enlarged azygos vein (arrowhead). B, The lateral view of the chest is notable for the absence of the inferior vena cava shadow. C, Contrast-enhanced computed tomography (CT) scan of the chest shows cardiomegaly, a left-sided aorta (arrow), prominent pulmonary veins, and an enlarged azygos vein (arrowhead). D, A contrast-enhanced CT scan of the chest displayed in the lung window shows the presence of multiple dilated peripheral pulmonary vessels (arrows). E, Coronal reconstruction from a contrast-enhanced CT scan of the upper abdomen shows right-sided polysplenia (S), a right-sided stomach (white arrow), and a left-sided liver. A large right-sided portosystemic shunt (splenic vein to renal vein) is present (open arrow). Superiorly, there is interruption of the inferior vena cava (IVC) with azygos continuation (not shown). F, A left pulmonary artery angiogram from a right jugular approach shows dilated peripheral pulmonary arteries and micro arteriovenous connections, consistent with hepatopulmonary syndrome as a result of the congenital portosystemic shunt. This child does not have liver disease, and the intrahepatic portal veins are present but small (Abernethy malformation type II). G, Perfusion portion of a ventilation-perfusion scan using technetium-99m macroaggregated albumin performed after closure of the patient’s atrial septal defect shows normal perfusion of the lungs. There is abnormal radiotracer uptake within the brain (arrow) and kidneys (arrowhead). The percentage of systemic tracer uptake was calculated at 44.7%. These findings are typical of a right-to-left arteriovenous shunt and confirm the presence of hepatopulmonary syndrome.