17 The Future: Trends and Developments in Spinal Cord Regeneration
Introduction
Many strategies are being explored to enhance recovery of spinal cord function.1 Everyone in the field of spinal cord injury (SCI) hopes that one day there will be a cure for the paralysis that follows a spinal cord lesion. Basic science has enhanced our understanding of the pathophysiology of traumatic spinal cord damage (Fig. 17.1) and demonstrated the efficacy of various interventions to improve neurological function following experimental spinal cord injury.2 The International Spinal Research Trust (ISRT) proposed a research strategy in 1996 to effectively direct resources by identifying areas in spinal cord research that would require particular attention.1 These areas are to:
- Minimize immediate harmful responses to SCI;
- Enhance trophic influence and blocking of inhibitory influence;
- Correct reconnection of damaged axons and targets;
- Optimize the function of surviving fibers (in the case of incomplete damage).
At this stage it is likely that individuals, with existing SCI, will need a combination of available therapies to restore maximum function.2,3 A single treatment to cure spinal paralysis has not emerged from research done to date. Whatever is involved in translating interventions from experimental models to humans,3,4 there remains the fundamental clinical challenge, and ultimate responsibility to patients, to know how to ask (let alone answer) the question “Does it really work?” We are still coming to an understanding of long-observed changes following acute cord insult—“spinal shock” and have recognized the need for better clinical evaluation.5–8 What follows is not acomprehensive coverage but an introduction to some of the aspects of this evolving area.
Spinal Cord Research
Research to find acure and to optimize the outcome, has to involve all the phases of care that follow inevitably from trauma to a person and the consequent physiological dysfunction of spinal cord “interruption”— beginning with effective handling at the scene of the accident, during acute care, and through rehabilitation.
At the cord level research focuses on four main areas:
- Neuroprotection
- Regeneration
- Transplantation
- Rehabilitation
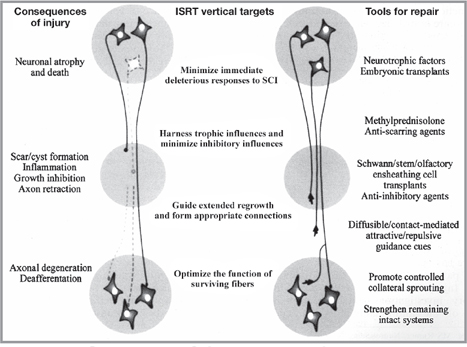
Fig. 17.1 ISRT research strategy—summary of the events subsequent to spinal cord injury.
Neuroprotection
Mechanical trauma inflicts direct neuronal damage but a large amount of axonal disruption and cellular death appears to result from secondary pathophysiological events. There is an evolving understanding of an “injury-triggered-cascade” of mechanisms, their complexity, and interactions.9–11 What actually happens in vivo in humans remains largely conjectured by extrapolation from this. Mention of a few of pathophysiological processes currently in focus may be appropriate9:
- Vascular mechanisms; loss of microcirculation, small vessel disruption, and hemorrhage, failure of autoregulation, and glutamate-mediated excitotoxicity;10
- Oxygen free radical formation and cell membrane lipid peroxidation;
- Apoptosis, the term for programmed cell death. This contrasts with necrotic death of cells at the site of trauma, which releases cell contents that cause a secondary inflammatory reaction.
Apoptotic demise of neurons and oligodendrocytes has been demonstrated postmortem in human SCI.12 Other work suggests a time course for this process of a few hours to 3 weeks, maximal around day 8 postinjury.13,14
On the basis of the evolving data of these pathophysiological mechanisms, it is possible to introduce experimentally efficacious interventions—glutamate receptor antagonists, agents affecting free radical formation and lipid peroxidation, inflammatory response modulators, targeting the molecular apoptotic pathway. (Specific agents are detailed in the referenced articles.)
Clinical trials in acute spinal cord injury are possible but difficult—the methylprednisolone and GM-1 ganglioside (Sygen) experience has been instructive.15–19 Randomized controlled trial design, execution, and reporting standards have moved on from those of the National Acute Spinal Cord Injury Studies (NASCIS) with the intention of improving the value of trial results as evidence of clinical effectiveness.20 The patterns of neurological loss (spinal cord level and completeness), the natural history of recovery and relevant outcome measures, which were considered in detail for the Sygen research remain a crucial “trial design challenge.”18
Regeneration
Is it possible to get CNS neurons to grow and regenerate? Two concepts had emerged from basic research: injured neurons lacked the intrinsic ability to regenerate; the CNS environment was not permissive to regeneration.21,3
Experiments have demonstrated that neurons can become “regeneration-capable” and regeneration-associated genes in the cell body up-regulated by the application of trophic factors to the cell body and also to the injured axon.21,3
Various strategies have been effective in facilitating “permissiveness to regeneration” at the injury site: providing a “cellular bridge” using Schwann cells, olfactory ensheathing glial cells, fetal tissue, stem cells; opposing axonal growth inhibitory molecules within the glial scar, e.g., effect of chondroitinase ABC on chondroitin sulfate proteoglycans; direct application of trophic factors such as NT3 or antibody to inhibitors—IN-1 antiNogo-A antibody.3
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


