This article highlights the range of pathology encountered in the intraconal space of the orbit including infectious, inflammatory, benign, and malignant conditions. Knowledge of the anatomy of the intraconal contents is crucial to understanding the appearance of each lesion. Key imaging patterns and important clinical considerations are provided to aid the imager in forming a helpful differential.
Key points
-
•
Significant imaging overlap exists among the spectrum of intraconal orbital pathology and consideration of corollary clinical details is crucial.
-
•
Orbital cavernous venous malformations represent the most common benign intraconal mass in adults but are not true neoplasms.
-
•
Orbital lymphoma smoothly fills the orbital contents and engulfs adjacent structures.
-
•
Optical nerve sheath meningioma demonstrates characteristic “tram-track” enhancement, which spares the nerve itself.
-
•
Metastatic lesions of the orbit most commonly arise in breast cancer and carry a poor prognosis.
Abbreviations
| CVM | cavernous venous malformation |
| ECD | Erdheim Chester disease |
| IOI | idiopathic orbital inflammation |
| LCH | Langerhans cell histiocytosis |
| NF1 | neurofibromatosis type 1 |
| ONSM | optical nerve sheath meningioma |
| OPG | optical pathway glioma |
| SFT | solitary fibrous tumor |
| TED | thyroid eye disease |
Introduction
The intraconal space or intraconal orbital compartment encompasses a conical volume of the post-septal orbit extending from the posterior globe margin to the apex defined by the planes of the four rectus muscles (superior, inferior, medial, and lateral) ( Fig. 1 ). This idealized myofascial cone encompasses the retrobulbar soft tissues to form the apical tendinous ring (annulus of Zinn) merging with the periorbita at the optical nerve canal and superior orbital fissure. The intraconal space is primarily occupied by orbital fat but also includes vital nerves (notably the optical nerve as well as branches of CN III, V, and VI) and vessels (notably the ophthalmic artery and posterior aspect of the superior ophthalmic vein). For this review, the rectus musculature, sometimes referred to as a separate “conal” space, will also be included in discussion of intraconal tissues. Conceptualization of the intraconal space (as distinct from other subsites of the orbit such as extraconal soft tissue, bony orbit, or globe) forms an important framework to understanding the wide range of potential conditions.
Anatomy ( A ) axial, ( B ) coronal, and ( C ) sagittal post-contrast CT images with color overlay. Blue: intraconal space. Red: extraocular muscles. Yellow: extraconal (post-septal) tissues.
This review highlights specific pathology encountered in the intraconal orbit, building on the above anatomic framework and recognition of imaging patterns. Further organization is provided by consideration of broad categories spanning infection/inflammatory, masses, and vascular etiologies. Note many of the lesions considered may present with multi-compartmental intraconal and extraconal involvement. As with all orbital imaging, there is significant imaging overlap among inflammatory, benign and malignant conditions, and clinical insight is critical.
Vascular
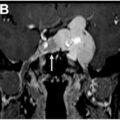
Orbital cavernous venous malformation (CVM) is the most common adult intraconal “mass,” composed of dilated “cavernous” vascular channels. As this represents a slow-flow vascular malformation rather than neoplasm, the older terminology of “hemangioma” is discouraged but still commonly used clinically. Recent work has investigated genetic alterations, highlighting a distinctive GJA4 (gap junction protein alpha 4) mutation in the majority of orbital CVMs. Typical presentation is an incidental intraconal mass in an adult of which a significant percentage will demonstrate with slow growth over time. Symptoms such as painless proptosis, diplopia or vision loss may be present when large or located in critical areas such as the orbital apex. Treatment is surgical, predominantly through orbitotomy, with low risk of recurrence. Imaging with MRI reveals a well-circumscribed T1 hypointense, markedly T2 hyperintense mass, often with a T2 hypointense thin pseudo-capsule ( Fig. 2 ). CT shows a similar homogeneous soft tissue density, rarely with osseous remodeling. The key to diagnosis on CT or MRI is a pattern of progressive enhancement—from early arterial phase poor heterogeneous enhancement to later phase avid uniform filling. Confirmation of this pattern can be obtained with tailored protocols adding arterial and venous/delayed phases. More practically, a similar effect can be appreciated on standard protocol MR comparing earlier sequences to later sequences acquired in an alternative plane.
Cavernous venous malformation (hemangioma). ( A ) Axial T2 MR shows a right intraconal well defined markedly hyperintense mass with a thin hypointense pseudocapsule ( arrow ) and subtle chemical shift artifact. ( B ) Axial T1 post-contrast image and subsequent ( C ) coronal MR image show progressive patchy enhancement becoming more uniform ( arrows ). This patient went on to radiation therapy after subtle lesion growth to preserve vision given fear for progressive mass effect upon the optical nerve at the apex.
Differential considerations include other benign vascular lesions such as the venous varix which should demonstrate characteristic increased volume on Valsalva imaging. The much less common orbital schwannoma may overlap with CVM as a T2 hyperintense circumscribed mass necessitating careful review of post-contrast imaging. If intense early arterial-phase enhancement is present, alternative vascular, neoplastic or malignant etiologies should be considered including solitary fibrous tumor (SFT) in adults versus capillary hemangioma or rhabdomyosarcoma in pediatrics. Finally, the lymphatic malformation presents in children with a strikingly different imaging pattern: a multi-spatial lobulated multicystic lesion with thin peripheral or no enhancement and characteristic fluid-fluid levels on MRI due to tendency for internal hemorrhage ( Fig. 3 ).
Orbital lymphatic malformation. ( A ) Axial T2 MR shows a lobulated lesion in the left intraconal space with fluid-fluid levels suggestive of intralesional hemorrhage and dependent proteinaceous contents ( arrow ). ( B ) Axial T1 post-contrast MR confirms absence of nodular or mass-like enhancement. ( C ) Coronal STIR MR shows corollary multi-lobulated lesion ( short arrows ) surrounding the optical nerve.
Mass
Lymphoma
Orbital lymphomas represent the most common orbital neoplasm in the adult and may involve any portion of the orbit. This review will focus on true malignant pathology, noting that much of the imaging literature discusses these in the setting of a “spectrum” of benign or reactive chronic lymphoproliferative disorders including idiopathic orbital inflammation (IOI). The typical presentation for orbital lymphoma is an older patient with indolent, painless proptosis or diplopia, usually without additional systemic symptoms. The most common pathology is non-Hodgkin B-cell lymphoma, most frequently low grade extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue subtype. Typical treatment is low dose radiation therapy with excellent local control and overall survival. In general, the risk of systemic lymphoma is increased, particularly in bilateral orbital involvement, and appropriate screening is warranted. High grade lymphoma (diffuse large B-cell or mantle cell) or secondary orbital involvement of a systemic lymphoma often presents as a more aggressive disease that may require multimodality therapy for control.
Orbital lymphoma can present with a wide variety of imaging patterns with overall unilateral disease more common than bilateral, and extraconal involvement more common than intraconal. Extraconal (lacrimal or conjunctival) lymphoma involvement is beyond the scope of this review. Intraconal involvement typically presents as a uniform mass filling the retrobulbar fat planes and engulfing adjacent structures such as the optical nerve and extraocular muscles ( Fig. 4 ). On non-contrast CT, lesions may be slightly hyperdense indicating increased cellularity. MRI demonstrates similar hypercellular corollary findings such as T2 intermediate-dark signal and restricted diffusion. FDG PET may be limited by the physiologic uptake of rectus musculature but is important for evaluation of the presence or extent of systemic disease. Unfortunately, due to the protean nature of lymphoma, there is significant imaging overlap with other orbital etiologies, most commonly inflammatory conditions. Small series investigative studies have proposed cutoff ADC values to differentiate lymphoma from IOI, , although significant individual variability limits clinical use. Lymphoma may be favored after consideration of clinical factors (such as the absence of pain or sinusitis) but usually requires biopsy for confirmation and pathologic subtyping. Additional etiologies such as orbital metastases or aggressive infection should be excluded by morphology and clinical factors.
Intraconal lymphoma examples. Patient 1: ( A ) Coronal STIR MR shows T2 intermediate hyperintense signal throughout the intraconal and extraconal fat engulfing the optical nerve ( arrow ), rectus musculature, and vasculature. ( B ) Axial T1 post-contrast MR shows infiltrating enhancement of the left intraconal ( arrow ) and superficial ( curved arrow ) tissues with resultant proptosis, although no deformation of the globe. ( C ) Axial ADC MR confirms relative restricted diffusion ( arrow ). Patient 2: ( D ) Coronal post-contrast CT shows uniformly enhancing right orbit intraconal soft tissue ( arrow ) surrounding the optical nerve. ( E ) Axial T1 MR and ( F ) ADC map show corollary homogeneous signal ( arrow ) filling the intraconal fat with restricted diffusion.
Leukemia
Leukemia (typically acute myeloid leukemia or acute lymphoblastic leukemia) can also present with poorly defined or discrete intraconal or multifocal masses representing extramedullary disease also termed myeloid sarcoma, chloroma, or granulocytic sarcoma ( Fig. 5 ). Although more commonly described in children, adult orbital leukemia may present with chemosis, blurry vision or proptosis, typically unilateral, which may precede a systemic diagnosis. Associated MRI bone marrow signal abnormality may serve as an imaging clue to a systemic process if not clinically evident. Adjacent facial and skull base soft tissue planes should be scrutinized for evidence of more aggressive disease extending beyond the orbits.
Orbital acute myeloid leukemia. ( A ) Axial T1 post-contrast fat saturated MR shows a right orbital mostly intraconal mass ( arrow ) distorting the optical nerve and lateral tissue planes. ( B ) Coronal T2 MR shows intermediate signal engulfing the lateral rectus ( curved arrow ) with broad contact of the optical nerve. ( C ) Coronal T1 post-contrast MR shows similar extent as well as hazy margins of the medial intraconal tissues ( short arrow ). Biopsy confirmed myeloid sarcoma compatible with relapse of disease is this patient with treated AML and stem cell transplant with new right-sided vision loss.
Schwannoma
Orbital nerve sheath tumors are rare but most commonly represent schwannomas or solitary neurofibromas. They may arise from peripheral branches of cranial nerves III through VI, as well as sympathetic or parasympathetic fibers, with most common origin reported as cranial nerve V branches. A handful of reported schwannoma cases associated with CN II (myelinated by oligodendrocytes) are felt to arise from small adjacent sympathetic branches along sheath vasculature or possibly aberrant Schwann cell deposition.
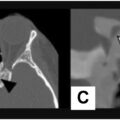
Imaging appearance is in line with schwannomas elsewhere in the head and neck, characterized by well circumscribed, enhancing masses with T2 hyper or iso-intense components, and sometimes cystic spaces if large ( Fig. 6 ). A key imaging clue to nerve sheath origin is characteristic elongated morphology along the expected course of a known cranial nerve branch, which gives rise to an often extraconal and intraconal course. Additional key imaging distinctions from CVM include T2 heterogeneity (relating to underlying varying Antoni A and B cellular patterns and cystic spaces) and lack of progressive “spreading” enhancement. Differences in MR perfusion time-intensity curves have also been described. Slow growth is typical unless malignant and smooth osseous remodeling may be present when large. Neurofibroma, unlike schwannoma, lacks a capsule and may be less well defined. Ultimate diagnosis usually requires pathologic or syndromic clinical confirmation to differentiate.
Orbital schwannoma. ( A ) Axial T2 fat-saturated MR, ( B ) axial T1 post-contrast fat saturated MR, ( C ) coronal T2 fat saturated, and ( D ) coronal T1 fat saturated MR images show a large right orbital mass with heterogeneous T2 characteristics, cystic change anteriorly, and avid enhancement with resultant proptosis. Note extension to the superior orbital fissure ( arrow ) and superior displacement/flattening of the right optical nerve ( curved arrow ). Pathology following resection confirmed schwannoma WHO grade 1.
Histiocytosis
Histiocytosis disorders represent a rare but increasingly recognized group of related but pathophysiological distinct conditions with complex multi-system clinical manifestations. Orbital involvement represents a diagnostic challenge given the broad spectrum of presentations and overlap with other multisystem imaging findings. Langerhans cell histiocytosis (LCH) is the most common subtype, although with the lowest proportion of orbital involvement, usually manifesting as defined lytic lesions in the bony orbit with associated extraconal soft tissue masses. Erdheim Chester Disease (ECD) involves the orbits in up to 30% of cases at a rate five times that of LCH. The most common orbital manifestations of ECD include discrete or infiltrative retrobulbar enhancing masses, of which the majority are bilateral and intraconal ( Fig. 7 ). Associated radiologic clues for ECD include osteosclerosis of facial bones and/or lower extremities, retroperitoneal fibrosis, intracranial masses or pituitary abnormalities with resultant diabetes insipidus. Both LCH and ECD can be associated with BRAFV600E mutation which if present will guide targeted systemic therapy. Rosai Dorfman disease most commonly presents with lymphadenopathy, although extranodal orbital involvement is reported, typically with ill-defined or bulky multi-compartmental soft tissues lesions. In general, the diagnosis of histiocytosis should be entertained in younger patients with insidious onset symptoms after recognition of the key patterns of multi-systemic involvement.
Erdheim Chester disease. ( A ) Coronal STIR MR and ( B ) T1 post-contrast fat saturated MR images show a large left intraconal mass ( arrow ), which is heterogeneous on T2 and avidly enhancing. Also note the smaller right orbital mass ( curved arrow ). ( C ) Axial T1 MR confirms bilateral disease with mass effect on the globe on the left ( short arrow ). ( D ) FDG PET CT axial fused image shows soft tissue infiltration throughout the peritoneal and bilateral retroperitoneal cavity with varying FDG avidity, confirming a multi-system process ( arrows ).
Solitary Fibrous Tumor
SFT is the correct nomenclature (based on immunohistochemical categorization) for a spectrum of tumors including the outdated terminology of orbital hemangiopericytoma. SFT represent a rare, slow-growing highly vascular tumor, most commonly presenting in middle-aged adults with female predominance. Lesions are more commonly extraconal, although purely intraconal or multicompartmental involvement is also possible. Treatment is by surgical excision with a tendency for local recurrence in the setting of positive margins. Distant metastases are rare but reported for tumors with malignant histology.
SFT imaging characteristics typically show a lobulated mass with avid early-phase arterial enhancement, in contradistinction to the late progressive enhancement of cavernous venous malformation ( Fig. 8 ). MR signal is often isointense to gray matter on T2 sequence, which also helps to differentiate them from CVM. Indistinct margins, osseous remodeling or extraorbital extension can be present based on variable rate of growth or aggressive nature.
Solitary fibrous tumor. ( A ) Axial and ( B ) coronal T1 post-contrast fat-saturated MR images show a lobulated discrete avidly and heterogeneously enhancing mass extending from the intraconal planes to the lateral extraconal and superficial tissues ( arrows ). ( C ) Axial T2 MR image shows regions of intermediate signal isointense to brain ( curved arrow ). ( D ) Axial post-contrast CT image confirms avid enhancement ( short arrows ). Note absence of the left lateral orbital wall from prior resection attempt.
Optical Nerve Sheath Complex
Optical nerve sheath meningioma
Optical nerve sheath meningioma (ONSM) most commonly presents with progressive unilateral peripheral vision loss, typically in a middle-aged female. They are estimated to represent approximately 4% of all orbital masses and 1 to 2% of all meningiomas. There may be a syndromic association with neurofibromatosis 2, particularly in younger patients or rare bilateral involvement. Characteristic findings on ophthalmologic examination include optical disc pallor and swelling with optociliary venous shunting. Pathologic classification follows that of intracranial meningiomas, and although typically low grade, critical location necessitates treatment as a distinct clinical entity. First line treatment is radiation therapy with the goal of arresting tumor growth and preserving residual vision. The risk of vision loss with surgery limits resection to cases with aggressive growth or otherwise dismal prognosis.
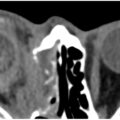
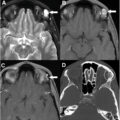
MRI provides the best characterization of an ONSM as well as the adjacent optical nerve. Post-contrast imaging with fat saturation best illustrates the typical linear/tubular, often eccentric circumferential or plaque-like enhancement of the optical nerve sheath surrounding a non-enhancing optical nerve, most commonly involving the posterior intraorbital segment ( Fig. 9 ). Characteristic imaging enhancement patterns have been described as “tram track” pattern on axial or “doughnut” sign on coronal imaging. Mild T2 hyperintense dilatation of the sheath anterior to the tumor can be seen, historically termed as “perioptic cyst.” CT may show a similar pattern of enhancement or less commonly mineralization. More recently, 68Ga-DOTATATE PET has emerged as a diagnostic tool for confirming or defining the extent ONSMs with implications for treatment planning. ,
ONSM. ( A ) Coronal and ( B ) axial T1 post-contrast fat-saturated MR images show circumferential enhancement along the left intraorbital optical nerve sheath surrounding the non-enhancing optical nerve ( arrows ). Axial images demonstrate a tram-track pattern of enhancement. ( C ) Axial non-contrast CT shows similar pattern of calcification along the optical nerve sheath ( short arrows ). ( D ) DOTATATE PET MR axial fused image shows corollary avidity ( curved arrow ) confirming elevated somatostatin receptor density, as expected in meningioma. ONSM, optical nerve sheath meningioma.
ONSM may be misdiagnosed as an intrinsic nerve pathology such as optical neuritis, in one series leading to a delay in diagnosis of 71% of patients. Other less common etiologies may also be indistinguishable from meningioma on a single imaging time point including peri-neuritis pattern inflammatory or lymphomatous disease.
Optical pathway glioma
Optical pathway gliomas (OPG) have a highly variable clinical course and presentation based on age, syndromic association and location. While the overall prevalence is similar to ONSM, the striking difference is that over 75% of OPGs present in children under the age of 10 years. Anatomically, they can be subdivided by location into anterior (pre-chiasmatic) and posterior (chiasm/hypothalamic) tumors. In children, these most often represent indolent low-grade gliomas (most common histologic subtype juvenile pilocytic) and can be sporadic or syndromic in association with neurofibromatosis type 1 (NF1). The rarer adult or malignant OPG is associated with rapid progression of vision loss, higher grade tumor and poorer prognosis. Observation is typically recommended for small anterior tumors or those associated with NF1, and biopsy is rarely required although increasingly common for identifying targets for newer therapies. Progressive vision loss or growth warrants treatment initially with targeted chemotherapy/immunotherapy in young children, radiation therapy, or surgery reserved for rare circumstances after multi-disciplinary input.
Imaging of OPG shows smooth, fusiform and tortuous long segment enlargement of the optical nerve. MR signal characteristics are similar to brain parenchyma on T1, usually hyperintense on T2, and variably enhancing ( Fig. 10 ). OPG in NF1 typically involves the anterior pathways, may be bilateral, and is often accompanied by additional intracranial or cutaneous manifestations evident in the field of view. Sporadic OPG more frequently shows posterior chiasm or hypothalamic involvement as well as more pronounced enhancement and nodularity. Enhancement may vary over time or with therapy, leaving tumor growth as the most indicative sign of progression. Differential considerations include optical neuritis, which is usually non-expansile, as well as rarely ONSM discussed above.
Optic pathway gliomas. Syndromic glioma: ( A ) Coronal STIR and ( B ) T1 post-contrast fat saturated MR images show enlargement of the intraorbital left optical nerve ( arrow ) without significant enhancement. ( C ) Axial T2 FLAIR MR image through the posterior fossa shows scattered foci of T2 hyperintensity ( short arrows ) compatible with intracranial vacuolization commonly seen in children with NF1. Sporadic glioma ( D ) Coronal STIR, ( E ) axial T2 with fat saturation, and ( F ) axial post-contrast T1 MR images show an enlarged, T2 hyperintense, avidly enhancing right optical nerve ( arrows ) with posterior extension nearly to the chiasm ( curved arrow ). This patient went on to resection due to concern for spread to the chiasm and loss of contralateral vision. Pathology yielded low-grade glioma, subclass midline pilocytic astrocytoma.
Infection
Orbital infection can be conceptualized as a spectrum from mild (pre-septal cellulitis) to severe (abscess or intracranial complications). Clinically hallmarks of any orbital infection include fever, pain and superficial orbital erythema, often in the setting of sinusitis and/or an immunocompromised state. Involvement of the intraconal soft tissues by an infectious process suggests moderate to severe aggressive extent and warrants complete characterization with both CT and MR. Management will often involve hospital admission for IV antibiotics, careful ophthalmologic monitoring and potentially surgical intervention considering morbidity including risk to the optical nerve.
Intraconal findings of infection on CT or MR are characterized by heterogenous stranding and infiltrative enhancement of the normally bland retrobulbar fat. Additional manifestations include focal soft tissue infiltration posterior to the globe in advanced scleritis or extraocular muscle enhancement as in myositis. The rare intraconal orbital abscess (as opposed to subperiosteal abscess confined by the periorbita) manifests as a defined fluid collection with peripheral enhancement and restricted diffusion within the intraconal space ( Fig. 11 ). Abscess may be seen in immunocompromised patients or in the setting of hematogenous spread. Careful imaging review is vital to evaluate for additional aggressive sequela such as cavernous sinus thrombosis, skull base osteomyelitis or intracranial extension.
Related posts:
 Orbital Imaging Modalities and Recent Updates
Orbital Imaging Modalities and Recent Updates
 Imaging of the Cavernous Sinus
Imaging of the Cavernous Sinus
 Imaging of the Globe
Imaging of the Globe
 Multidisciplinary Management of Tumors of the Orbit
Multidisciplinary Management of Tumors of the Orbit
 Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
Skull Base, Bone, Pituitary—Regions around Orbit that Affect Vision
 Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Imaging Findings after Multidisciplinary Treatment for Orbital and Ocular Adnexal Cancers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


