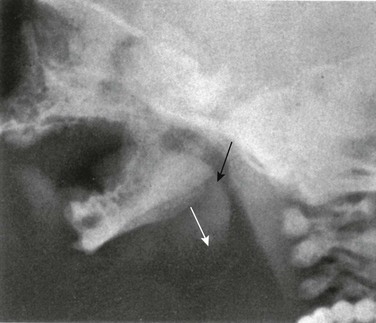
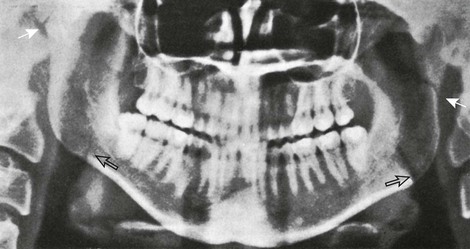
Chapter 22 At birth, the mandible consists of two lateral halves united in the midline at the symphysis by a bar of cartilage (Fig. 22-1, e-Fig. 22-2, and Figs. 22-3 and 22-4). Bony fusion of the symphysis usually occurs before the second year, but segments of the fissures may persist beyond puberty. The body of the mandible is large at birth compared with the relatively short rami and poorly differentiated coronoid and condylar processes. The rami form an angle of about 160 degrees with the body at birth. All or some of the teeth may be missing developmentally, as in persons with anhidrotic ectodermal dysplasia (Fig. 22-4).1 Because infants and children with normal dentition seem to have a plethora of teeth in radiographs (deciduous and permanent dentitions), the condition may be recognized in a newborn by the lack of dental buds. Many diseases cause loss of dentition, and recognition of premature loss of teeth can lead to important diagnoses (Box 22-1).2 The opposite condition—too many teeth with little alveolar bone—can be seen in persons with cleidocranial dysplasia, who have marked delay in shedding of the deciduous teeth. Early tooth extraction has no effect on the subsequent eruption of the permanent dentition and may result in a lengthy edentulous period for the child.3 The mandible is the only freely movable bone of the face; it articulates with the temporal bone in the temporomandibular fossa anterior to the external auditory canal (see Fig. 22-3). The range of motion is free in all directions, and the condyle moves downward and forward in the articular fossa upon opening of the jaw. The temporomandibular joint (see Fig. 22-3) is a complex joint in which a biconcave fibrous disk divides the articular space into upper and lower compartments.4–6 Gliding movements occur in the upper compartment, whereas the lower compartment functions as a true hinge joint. The articulating bony surfaces are not covered by hyaline cartilage as in other joints, but by an avascular, fibrous tissue that is separated from the underlying bone of the condyle by growth cartilage.7 Significant congenital malformations of the mandible are rare, with the most important being hypoplasia (micrognathia), which may be a cause of congenital stridor. The short, small mandible apparently causes a retrodisplacement of the tongue and obstruction to airflow (Fig. 22-5). Micrognathia occurs in a variety of dysmorphic syndromes. The combination of cleft palate and hypoplasia of the mandible defines the Pierre Robin sequence radiographically. The Pierre Robin association is nonspecific and occurs with several genetic and drug-induced syndromes and some loosely associated anomalies, as well as an isolated symptom complex.8 In the cerebrocostomandibular syndrome, it is associated with posterior rib defects, cleft palate, and, occasionally, mental retardation.9 Disorders of the temporomandibular joint are infrequent but not rare.10,11 Adventitious sounds on mandibular movement, muscle tenderness or pain, and deviation of the mandible during movement are the most common signs and symptoms. Magnetic resonance imaging (MRI) is the most precise imaging modality.12,13 Direct trauma is the usual cause of fractures, although pathologic fractures occur in association with cysts, destructive inflammations, and neoplasms. More than half of traumatic fractures are found in the body of the mandible near the canine fossa. Fractures high in the ramus frequently are overlooked on standard radiographs but are clearly defined by computed tomography (CT) (Fig. 22-6) and panographic tomography (e-Fig. 22-7). Direct trauma is the usual cause, although pathologic fractures occur in association with cysts, destructive inflammations, and neoplasms. More than half of traumatic fractures are found in the body of the mandible near the canine fossa. Figure 22-6 A fractured mandible.
The Mandible
Embryology
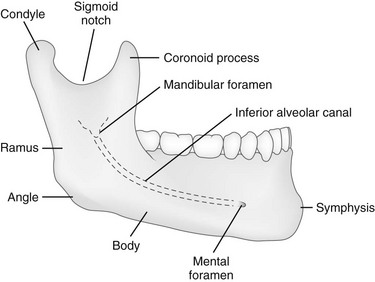
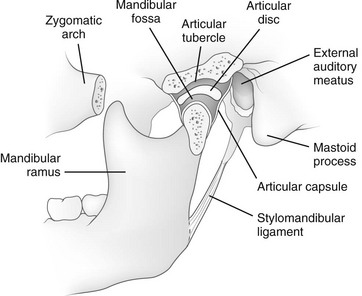
Anatomy
Diseases of the Mandible
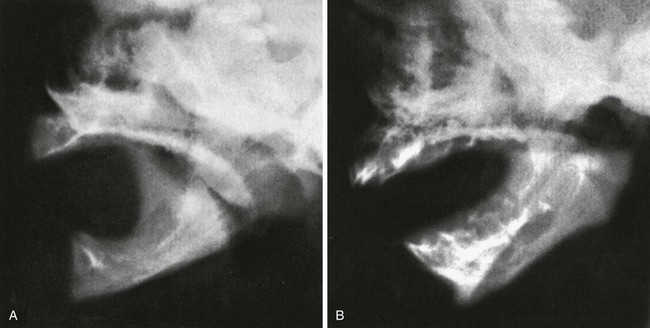
Temporomandibular Joint Disorders
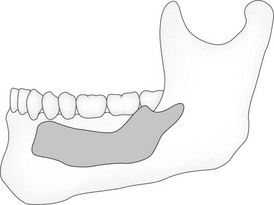
Fractures
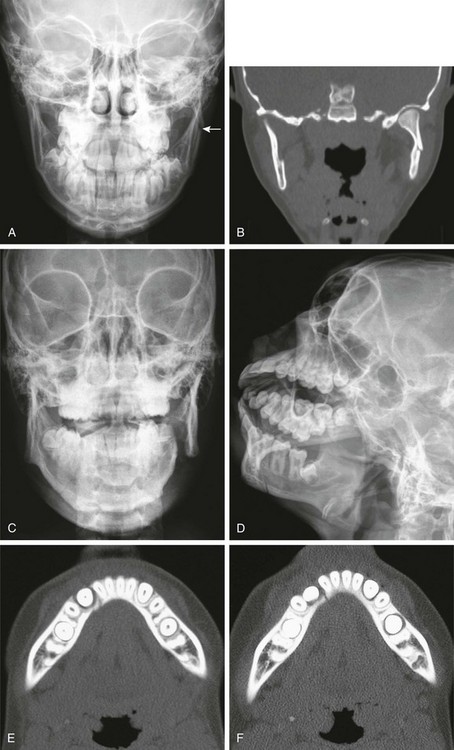
A, A 14-year-old patient with a subtle fracture of the left mandibular vertical ramus (arrow). B, Coronal computed tomography reconstruction shows the fracture. C, D, E, and F, A 14-year-old patient with an overt left mandibular fracture of the body and ramus junction and a subtle fracture through the right dentition.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine