4 The thorax
The thoracic cage
The typical rib (Fig. 4.1)
A typical rib has a head, neck, tubercle and shaft.
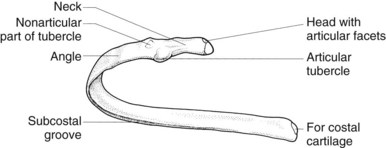
The neck of the rib is attached by a ligament to the transverse process of the vertebra above.
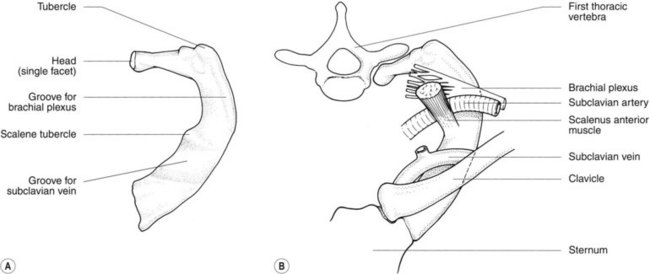
Atypical ribs
Costal cartilages
The intercostal space and vessels
Intercostal arteries
Posterior


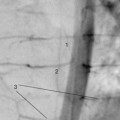
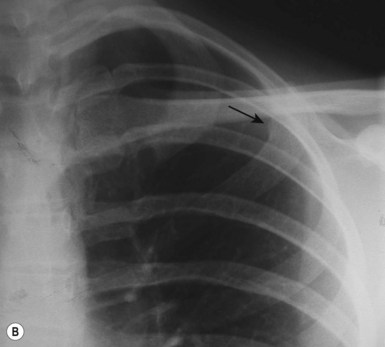
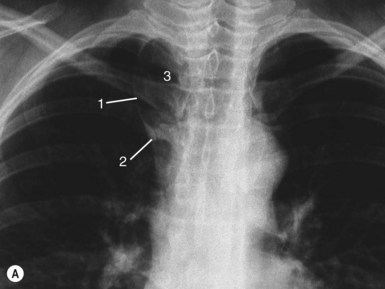
Radiological features of the thoracic cage (Fig. 4.3)


The sternum (Fig. 4.4A)

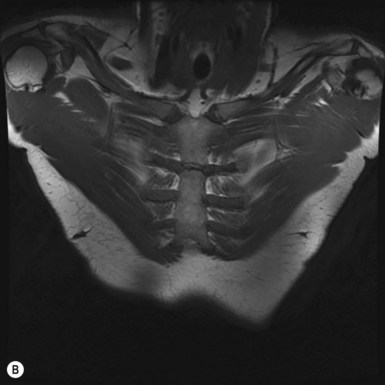
Figure 4.4 • The sternum. (A) Coronal reformatted CT image of the sternum and (B) MRI of the sternum.
The diaphragm (Fig. 4.5)
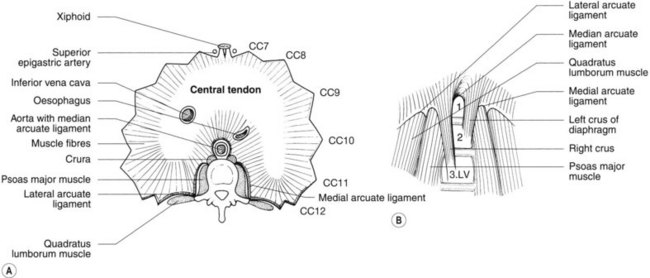
The costal part of the diaphragm arises in slips from the lower six costal cartilages.
Openings in the diaphragm
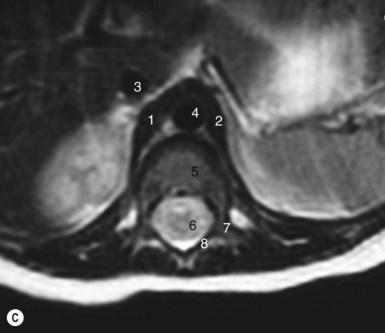
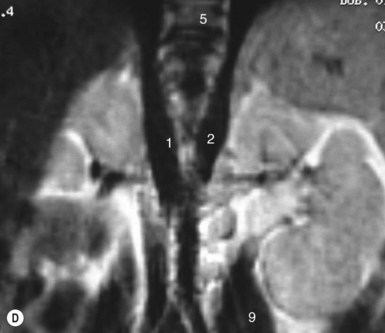
Radiological features of the diaphragm (Fig. 4.5)
PA chest radiograph (Fig. 4.6)

The range of movement of the diaphragm with respiration is as follows:
In each case the left hemidiaphragm moves more than the right.
The variation of the diaphragm with posture is as follows:
Lateral chest radiograph (Fig. 4.7)
The following anatomical details help identify the domes of the diaphragm:
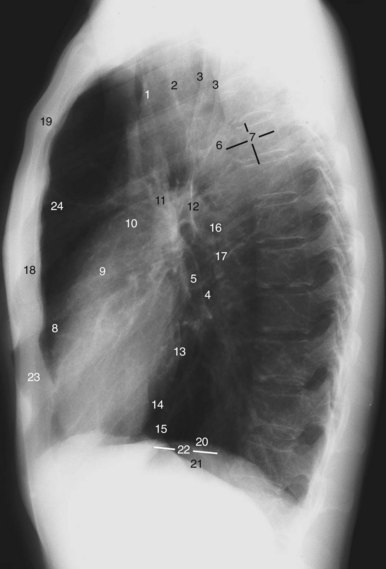
There is apparent thickness of the diaphragm on radiographs:
The pleura (Figs 4.8, 4.9)
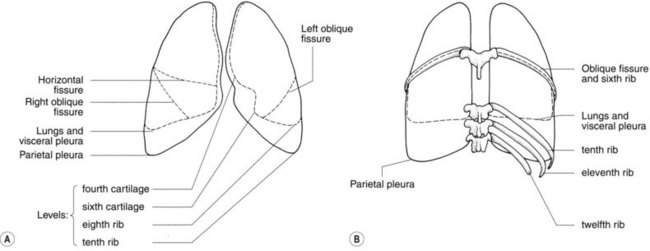

The visceral pleura extends into interlobar and accessory fissures. At rest the parietal pleura extends deeper into the costophrenic and costomediastinal recesses than do the lungs and visceral pleura (see Table 4.1 for lower limits of lungs and pleura).
Table 4.1 Lower limits of lung and pleura at rest
| Visceral pleura and lung | Parietal pleura | |
|---|---|---|
| Anterior | Sixth costal cartilage | Seventh costal cartilage |
| Midaxillary line | Eighth rib | Tenth rib |
| Posterior T10 | T10 | T12 |
Radiological features of the pleura
Plain films


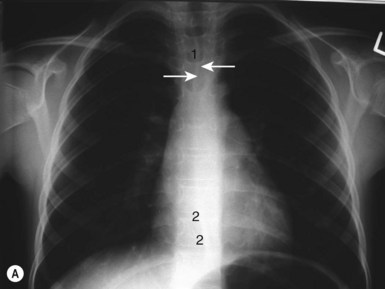
 Anterior junction line: anterior to the arch of the aorta the two lungs may come in contact with one another, separated only by four layers of pleura. This pleura is then seen as the anterior junction line on a PA chest radiograph.
Anterior junction line: anterior to the arch of the aorta the two lungs may come in contact with one another, separated only by four layers of pleura. This pleura is then seen as the anterior junction line on a PA chest radiograph.
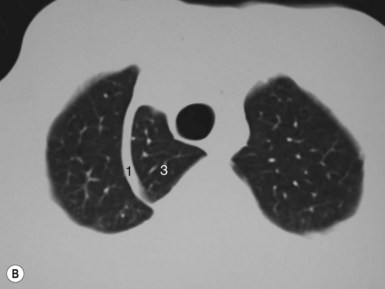
Computed tomography
On axial CT the pleura cannot usually be distinguished from the thoracic wall or mediastinum unless it is thickened (see section on fissures, p. 125). The pulmonary ligaments can occasionally be seen extending below the inferior pulmonary vein caudally and posteriorly to the diaphragm. The right pulmonary ligament lies close to the inferior vena cava (IVC), whereas the left pulmonary ligament lies close to the oesophagus.
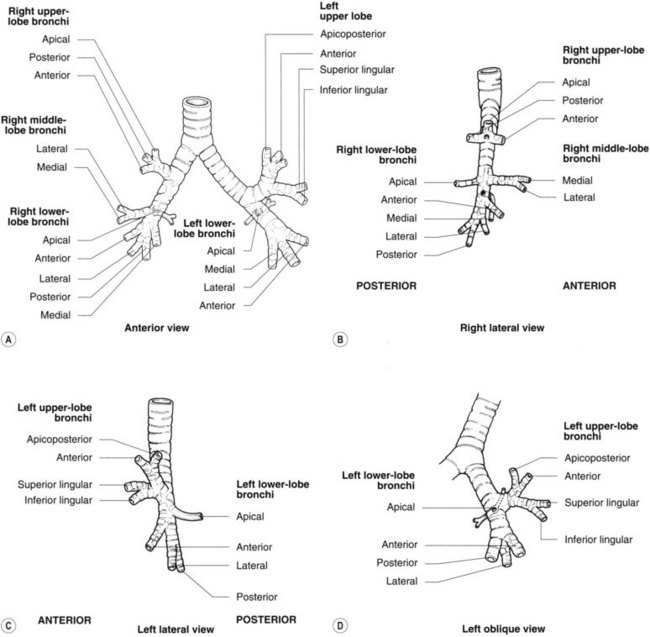
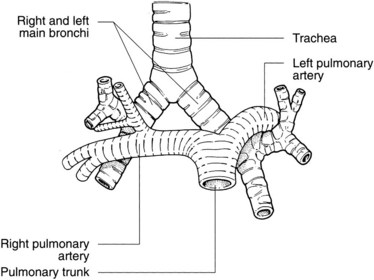
The trachea and bronchi (Figs 4.10–4.12)
The trachea
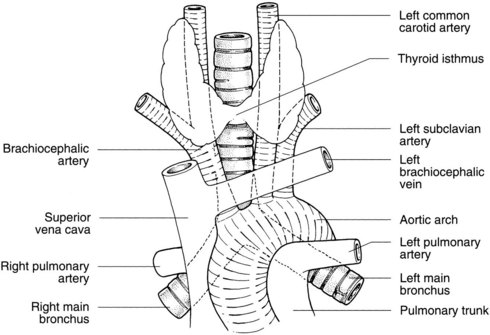
Relations of the trachea











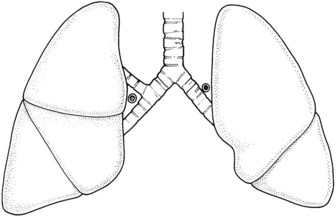
Main bronchi (Figs 4.10–4.12)


Left main bronchus (hyparterial bronchus)
The left main bronchus lies at 40° to the median plane. It is 5 cm long and 1.2 cm in diameter.
Relations
The relations of the left main bronchus are as follows:




The anatomy of the bronchial tree is shown diagrammatically in Figure 4.12. Naming basal bronchi laterally to medially is easier if the constant relationship of anterior, lateral and posterior (ALP) is remembered, with only the medial bronchus in the right lung changing its relative position.
The lungs (Fig. 4.13)
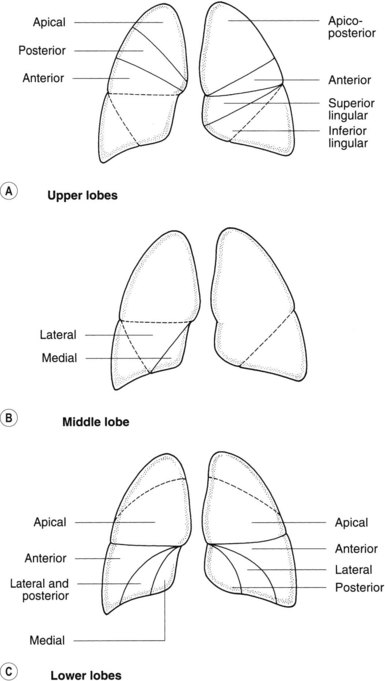
Figure 4.13 • Bronchopulmonary segments as seen on PA chest radiograph: (A) upper lobes; (B) middle lobes; (C) lower lobes.
Interlobar fissures (see Fig. 4.8)
The depth of fissures varies from a superficial slit to complete separation of lobes.
Accessory fissures
Bronchopulmonary segments (Figs 4.12, 4.13)
There is very little connection between segments except via:
The bronchial arteries
Bronchial arteries may also arise from the subclavian artery or from its internal thoracic branch.
Tissues supplied by bronchial arteries drain to pulmonary veins or bronchial veins.